Given my previous work in lab value changes in transgender
individuals on hormone therapy, I was recommended to consider discussing the
case of Olympic mid-distance runner, Caster Semenya. Although she is not
transgender, this professional runner from South Africa has won her last 30
races and been scrutinized for her muscular build as having potentially higher
levels of testosterone, a condition called hyperandrogenism. The International
Olympic Committee’s (IOC) regulations require testosterone levels to be below a
certain threshold for female athletes.
While no competitor can achieve great victories without hard
work and practice, there are certainly examples of outliers whose genetics give
them an advantage. However, I don’t think we would endorse shortening Michael
Phelps’ arms or lobotomizing chess master Bobby Fisher to decrease their inborn
advantages for a level playing field.
But this gets into an area of ethics that I’m not an expert
on, so instead I will stick to my area of science and examine what evidence may
exist to support the IOC’s policy. Then I will extrapolate the results from our
study of transgender individuals to see if hormone regulation may impact
contributions to athleticism. The most strongly shifted lab values in hormone
therapy for transgender individuals are red blood cells (including oxygen-carrying
hemoglobin) and creatinine (byproduct of muscle used to monitor kidney
function, but also reflects total muscle mass).
Once looking more closely at this topic, I realized there is
a lot to say about the contributions of 1) muscle mass and 2) red blood cells
to athleticism. So, I will discuss muscle mass this month and wait until next
month to discuss hemoglobin levels (including athletic performance by blood
removal/ doping).
Mid-distance running, which is Caster Semenya’s sport, is a
mix of anaerobic and aerobic activity. This means having more muscle would be
advantageous. This is supported by a study that was commissioned by the IAAF
(International Association of Athletics Federation), which shows a 1.8-2.6%
increased competitive advantage in short distance track events (400m, 800m and,
400m hurdles)1. However, this study had several limitations. First,
the sample size was quite low with only 22 female athletes. Next, they use a
p-value of 0.05 for significance without correction for multiple hypothesis
testing (21 hypotheses tested representing each event), which increases the
likelihood of a false positive result by chance.
What makes me curious is whether following the International
Olympic Committee’s recommendations of lowering testosterone levels would even
have a meaningful impact and improve competitiveness?
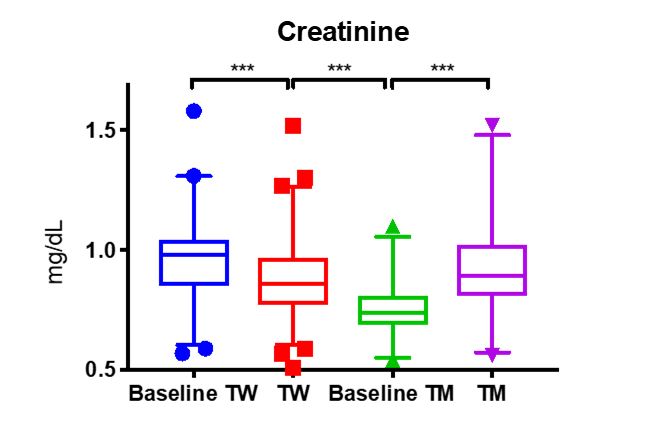
From my research, I know that adding testosterone to
individuals assigned female at birth to transition to transgender males (TM ) does
substantially increase creatinine (p<0.005, Figure 1)2 to male
levels (baseline TW). This is likely not due to changes in kidney function
(although this has not yet been proven), but rather due to increased muscle
mass.
Figure 1.
However, the inverse is not quite true for transgender women
who take combinations of estrogen for feminization and spironolactone to block
the effects of testosterone. In these patients, we see a slight decrease in the
creatinine (TW). While this decrease is statistically significant, the range is
not clinically different from male creatinine levels. This concurs with the
observations that musculature in transgender women does not change
substantially upon taking hormone altering medication.
A more rigorous examination of muscle mass, performed by MRI
measurement, determined that after 1 year of hormone therapy testosterone
increased muscle mass in transgender men to biological male levels3,
similar to our observations of creatinine. Further, they saw a significant
reduction in muscle mass from baseline of transgender women on hormone therapy
for 12 months, but it was still much higher than the muscle mass of biologic
females4.
Therefore, were Casten Semenya to take testosterone blocking
medication, I suspect there would be little impact on her overall muscle mass.
Which is one of, if not the explicit purpose of taking testosterone lowering
medicine. The strength of my conclusions is limited by the fact that we don’t
know Casten Semenya’s testosterone levels, and furthermore a hyperadrogenic
female is not the same as a male-to-female transgender woman.
As mentioned above, I will continue this discussion next
month with an exploration of how testosterone lowering therapy could affect red
blood cell levels, which would affect athletic performance differently.
References
Bermon S and Garnier P. Serum androgen levels
and their relation to performance in track and field: mass spectrometry results
from 2127 observations in male and female elite athletes. British Journal of
Sports Medicine. 2017; 51(17): 1309-1314.
SoRelle JA, Jiao R, Gao E et al. Impact of
Hormone Therapy on Laboratory Values in Transgender Patients. Clin Chem. 2019; 65(1): 170-179.
Jones BA, Arcelus J, Bouman WP, Haycraft E. Sport
and Transgender People: A Systematic Review of the Literature Relating to Sport
Participation and Competitive Sport Policies. Sports Med. 2017;47(4):701-716.
-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and advancing quality in molecular diagnostics.
A 71 year old man with a history of multiple myeloma
presented with urinary incontinence and confusion and was found to have
hyperkalemia with renal failure. Imaging showed extensive inguinal
lymphadenopathy with concern for new lymphoma.
Excisional Lymph Node Biopsy
H&E 40x
Diagnosis
Sections
show an enlarged lymph node with complete effacement of the normal lymph node
architecture by sheets of medium and large plasmablastic cells. The cells have
round nuclear contours, large prominent nucleoli and moderate amounts of
amphophilic cytoplasm. Frequent apoptotic cells and scattered mitoses are seen.
Immunohistochemical stains show that the neoplastic cells
are immunoreactive for CD138, CD38, CD19 (dim) and MUM1. They are negative for
CD20, which highlights only small admixed B-cells. The cells are kappa
restricted by kappa and lambda immunostain. The Ki-67 proliferation index is
greater than 90%.
Taken together, the morphologic and immunophenotypic
features are of a high grade plasmablastic neoplasm. The differential diagnosis
includes plasmablastic myeloma and a plasmablastic lymphoma. Given the
patient’s history of a kappa restricted plasma cell dyscrasia, plasmablastic
myeloma is favored.
Discussion
Multiple myeloma is a neoplasm of clonal plasma cells that
accounts for 10% of all hematologic malignancies. It is most commonly seen in
adult and elderly patients with a male predominance. Plasma cells are generally
characterized by the presence of a “clockface” nuclei and distinct perinuclear
Hof or clearing of the cytoplasm containing a large number of Golgi bodies. The
morphology of plasma cell tumors can range from small mature plasma cells to
anaplastic or plasmablastic morphology. In this case, the cells showed
plasmablastic (PB) morphology, which is characterized by a large nucleus, large
nucleolus, fine reticular nuclear chromatin pattern, lack of nuclear Hof and
less abundant cytoplasm than typical plasma cells.1
The differential diagnosis for cases with this morphology primarily
includes PB lymphoma and PB myeloma with extramedullary involvement. PB
lymphoma is seen more commonly in HIV positive patients or patients with other
causes of immunodeficiency. It typically occurs in adults and has a male
predominance. The tumor generally presents outside of nodes and is most
frequently seen in the oral cavity/jaw. Patients tend to present with advanced
stage and bone marrow involvement. While PB lymphoma is categorized as a
distinct subtype of diffuse large B-cell lymphoma, PB myeloma is considered an
atypical morphologic variant of multiple myeloma and is treated with therapy
geared towards plasma cell neoplasms. 2
Making the distinction between these entities is difficult due to similarities in morphology and immunophenotype. Ultimately, the diagnosis is generally made based on the clinical context. In one series of “plasmablastic” neoplasms by Ahn, et. al., 6 out of 11 cases were called PB lymphoma, 2 out of 11 were called multiple myeloma and 3 were called indeterminate. Among the PB lymphoma patients, 4 were either HIV positive or had a history of immunosuppression. All 6 cases were positive for CD138 and negative for CD20 with EBV in situ hybridization positivity in 3 out of 6 cases. The multiple myeloma cases had evidence of end organ damage without lymphadenopathy. One indeterminate case had peritoneal nodules, lytic lesions and an EBV positive neoplasm in the bone marrow, which precluded a definitive diagnosis. 3
The immunophenotypic pattern seen in this case is typical of
these neoplasms and is characterized by the expression of plasma cell antigens (CD138,
CD38, MUM1) with either weak or negative expression of B-cell antigens (CD20). A
study by Vega et. al. looked at the immunophenotypic profiles in nine cases of
PB lymphoma and seven cases of PB myeloma. They found that the profiles were
nearly identical. All cases were
positive for MUM1/IRF4, CD138 and CD38 and negative for CD20, consistent with a
plasma cell immunophenotype. PAX5 and BCL6 were weakly positive in 2/9 and 1/5
PB lymphomas and were negative in all PB myelomas. A high Ki-67, overexpression
of P53 and loss of p16 and p27 were present in both tumors. There was no
evidence of HHV8 detected in either neoplasm. The presence of EBV-encoded RNA,
was seen in all PB lymphoma cases tested and negative in all plasma cell
myeloma cases. This was found to be statistically significant. 4
Unfortunately, both PB lymphoma and PB myeloma are aggressive
high grade neoplasms with a poor prognosis. A study conducted by Greipp et. al.
assessed the prognostic significance of plasmablastic morphology in a cohort of
patients from the Eastern Cooperative Oncology Group Myeloma Trial E9486. They
looked at bone marrow aspirates from 453 newly diagnosed multiple myeloma cases
in a 5 year period. Of the 453 aspirates, 8.2% were classified as PB
morphology. The overall survival of
patients with PB morphology was significantly shorter than patients with non-PB
morphology with a median of 1.9 years compared to 3.7 years. There did not
appear to be a relationship between PB morphology to other clinical or
laboratory features such as age, sex, bone lesions or type of M-protein. 5
References
M Srija, P Zachariah, V Unni, et. al.
Plasmablastic myeloma presenting as rapidly progressive renal failure in a
young adult, Indian Journal of Nephrology,
Volume 24(1): 2014, Page 41-44.
JJ Castillo, M Bibas, RN Miranda, The biology
and treatment of plasmablastic lymphoma, Blood,
Volume 125, 2015, Page 2323-2330.
J Ahn, R Okal, J Vos, et. al. Plasmablastic
Lymphoma vs Myeloma With Plasmablastic Morphology: An Ongoing Diagnostic
Dilemma, American Journal of Clinical Pathology,
Volume 144(2): 2015, Page A125.
F Vega, CC Chang, LJ Medeiros, et. al.
Plasmablastic lymphomas and plasmablastic plasma cell myelomas have nearly
identical immunophenotypic profiles. Modern
Pathology, Volume 18: 2005, Page 806-815.
PR Greipp, T Leong, J Bennett, et. al. Plasmablastic Morphology – An
Independent Prognostic Factor With Clinical and Laboratory Correlates: Eastern
Cooperative Oncology Group (ECOG) Myeloma Trial 39486 Report by the ECOG
Myeloma Laboratory Group, Blood, Volume 91: 1998, Page 2501-2507.
–Chelsea Marcus, MD is a Hematopathology Fellow at Beth Israel Deaconess Medical Center in Boston, MA. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
Welcome back. Last month I
talked about a colleague of mine, a fellow student who’s pursuing a career
in pathology. The month before that I wrote a bit about Just
Culture and how those of us in laboratory medicine ought to act as leaders
for patient advocacy—especially when it comes to putting the needs of patients
first. And in the spirit of progressing career timelines and fortuitous
transitions, this month I want to talk about a place where Just Culture is tangible,
where “patient come first” is a mission statement, and where I just spent the
last month rotating in their Department of Laboratory Medicine and Pathology:
The Mayo Clinic.
Image 1. Commemorative statue of the Mayo brothers in a park in front of the main building of the downtown campus at Mayo Clinic in Rochester, MN.
Before I go any further, if you haven’t seen the PBS Ken Burns’ documentary,
I highly suggest you do; it’s
fantastic. There are also a few excellent books on the hospital’s history and
vision here
and here.
But back to the rotation: I can’t express how lucky I feel having spent time
there or convey how much of a privilege it was to see pathology in a uniquely
Mayo way. What I can do is try to talk a little bit about my experience and
what that translates to regarding a culture of advocacy and collaboration; and
I’ll share a case conference I presented on my last day in a topic I find
fascinating.
Image 2. Ken Burns presents The Mayo Clinic: Faith, Hope, and Science on PBS, which aired September 2018.
Mission, Vision, and
Values
As with any hospital, academic center, clinic, etc., you’re
always going to have a driving philosophy that anchors the values of that
particular institution. Some of my experiences in larger academic centers tout
their strides at the forefront of medicine and translational research, others
advertise that they treat the whole person body and spirit. Community hospitals
sometimes lean into their integral part of, well, their communities as a center
for trust and health. Sometimes institutions have specific populations to cater
to or work intensely with industry and boast strong contributions to medical
science. At the Mayo Clinic you’d be hard pressed to miss the message (in
various forms) that “The Patients Come First”—in fact that line from many years
ago comes from Dr. William Mayo delivering a commencement speech at a Rush
Medical College graduation. (I was so happy to see so many Chicago-Mayo Clinic
connections!)
Image 3. Dr. W. Mayo articulated the concept of patients’ “needs come first” in a graduation speech at Rush Medical College in Chicago on June 15, 1910.
It becomes very obvious that this culture of advocacy
permeates into the daily proceedings there. The hospital makes a strong point
to celebrate outreach, education, and research; and clinicians are given a
cultivated environment in which to flex muscles of compassion for patient
outcomes. It makes you a better clinician, and I argue, person. Everyone at
this hospital has a voice and a seat at the table. I was continuously encouraged
to interact with staff, clinicians, residents, fellows, and patients and
contribute what I thought would benefit patient care. A unique perspective as a
visiting medical student with previous MLS experience was both noted and
celebrated.
Leadership in
Pathology
In many of my pieces on this blog, I frequently discuss how
we should champion active roles in testing stewardship, policy advocacy, and
promoting positive patient outcomes. Granted, when you find yourself in larger,
resource-rich, tertiary academic centers you can really push the envelope for
progress. But generally, those of us on the ‘scopes operate in this margin
between clinical medicine and translational research. Where does our leadership
come in? What does it look like? I think it comes in the form of prolific
contributions to societal guidelines and interdisciplinary work. Nowhere have I
seen this more than my month in Rochester.
So many of their residents contributed abstracts and
presentations at this year’s USCAP conference, some winning awards. The
academic cycle of producing something great requires strong support from your
home institution and that’s exactly what I saw. Not only were folks supported
for their trips to conferences per usual, they were celebrated—hallway handshakes,
accolades at morning conference, discussions post-meeting, and social media
shares. Which, by the way, social media is now a leadership staple. You can’t
go far in the present day without utilizing technology both inside and out of
your practice. The Pathologist
recently celebrated their first #TwitterPathAward for residents like Dr. Tiffany
Graham at UAB for contributions to medical education and advocacy in pathology.
Mayo clinicians, including residents, consultants, pathologist’s assistants,
and more share case studies, educational material, and cutting-edge pathology
news in terabytes! I now find myself increasingly active on social media
representing pathology and interests within our field.
Image 4. A spring 2015 issue of The Pathologist discussed the increasing presence of pathology in social media and the trends of utilization for medical laboratorians abound.
Side note: I’ve followed a number of these social media
pages about cases in pathology for a while, and when I was fortunate enough to
be part of ASCP’s Top 40 Under Forty 2017, I connected with lots of awesome
laboratorians. Some of which I got to meet this month! Including a fellow
blogger on this site, some celebrated path assistants, and a prolific
parasite-discussing clinical microbiologist.
Case Conference
So, my presentation was intense! I’ve given plenty of case
reports and conference discussions before, but this was an opportunity for me
to explore quite a rare case in genetics and connect it with my interests in
hematopathology. This was a case of a patient with Li-Fraumeni Syndrome (LFS)
who developed therapy-related Acute Myeloid Leukemia. It’s not a current case
and has since been signed-out and closed, but I’ll only be talking about the
pathologic entities involved.
Image 5. Remember that power of social media I mentioned earlier? Well, what better way to share information for other medical students interested in pathology and interested in visiting Mayo Clinic! Having my presentation grab an honorable mention amidst their productive and busy residents was great! #path2path #hemepath #lablogatory
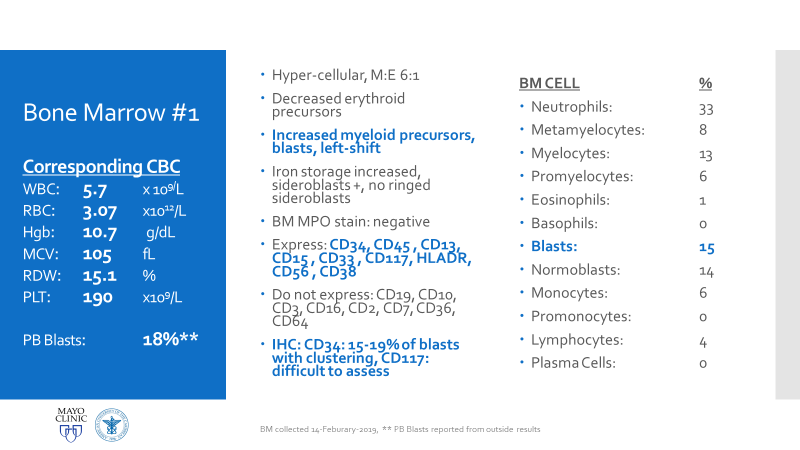
Essentially, this patient was found to have Li-Fraumeni after
the second manifestation of an acute sarcoma—the first being osteosarcoma in
her teenage years and the second breast cancer in her 30s. Both cancer
diagnoses were treated accordingly, and this patient was going through routine
work-up for anemia before being referred to the Mayo Clinic. By the time the
patient reached there, the clinical investigation included a battery of testing
for causes of anemia—all within normal limits—so a bone marrow examination was
performed which revealed a significant, though not acute (<20% blasts),
myelodysplastic process. A follow-up in-house bone marrow collection revealed
hypercellular marrow, now in acute myeloid proliferation, with abnormal myeloid
cell maturation and very complex cytogenetics. She had a very complex karyotype
and several detectable mutations which were consistent with the WHO’s
classification and description of therapy-related myeloid neoplasm as a sequale
to the treatments she received for her prior cancers. In the setting of a
patient with LFS, it is almost impossible to avoid malignancy. The following
slides are a (very abridged) summary taken from my presentation of this
patient’s case:
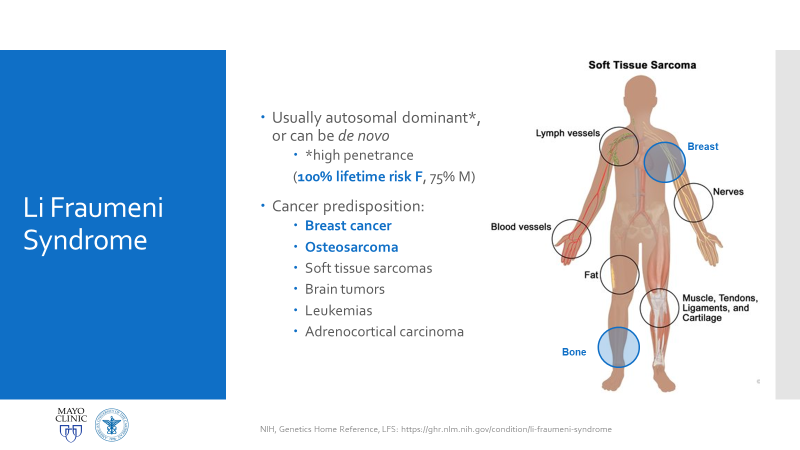
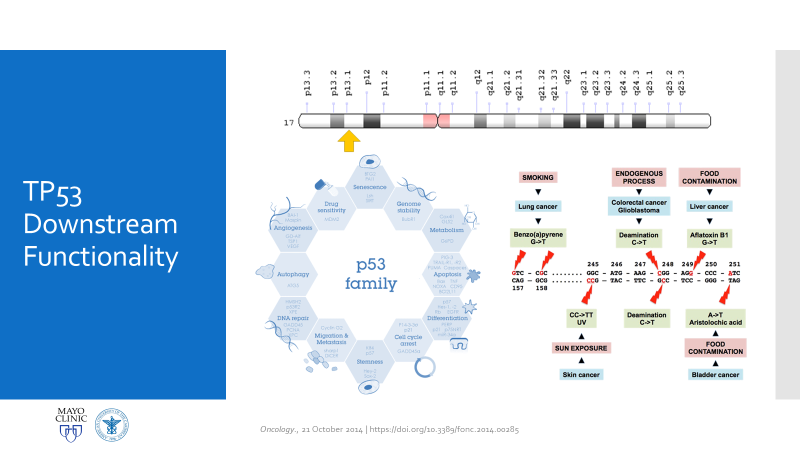
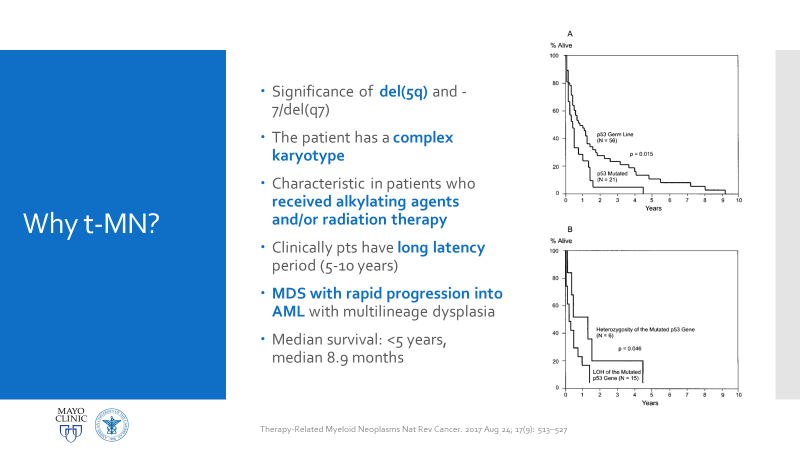
Figure 1. Official LFS and AML discussion. As mentioned, this is the case of a patient with a history of osteosarcoma and breast carcinoma, both treated, now presenting status-post initial work-up for evaluating possible causes for anemia. Ultimately, when reaching a bone marrow examination, certain myelodysplastic features were discovered, referring this case for close investigation and expanding the differential to include various hematologic malignancies.Figure 2. This bone marrow biopsy was evaluated at an outside institution and was reported to this patient’s case at Mayo Clinic. Note the presence of myeloid lineage blasts cells in the peripheral blood (PB) and bone marrow (BM) evaluations, however, at less than 20% this would not immediately indicate any acute myeloid crisis. There is a definitive left-shift in maturity with myeloid dysplasia. Figure 3. This bone marrow evaluation was done about a month after the previous reported one. Note the significant increase in myeloid blasts present in both peripheral and bone marrow specimens. This time, there was significant dysplasia noted in multiple lineages as well as particular changes in granulocytic lines including left-shift and pseudo Pelger-Huet cells present. This diagnosis was upgraded from myeloid dysplasia to acute myeloid leukemia in the setting of myelodysplasia. The blast count has now crossed the 20% threshold and there are marked changes to morphology in several cell lines. Hypercellularity and cytogenetic testing were also highly contributory in this diagnosis. Not included in this slide but CD34+ cells that previously expressed CD15, CD33, and CD38 were now negative for those three markers. This indicates decrease in maturity and a poorer prognostic and clinical assessment of this malignancy.Figure 4. A peripheral blood smear at the time of the second bone marrow specimen. In almost every field photographed, there were myeloid blast cells present. No Auer rods were seen, but many blasts had granules. There was left shift, and some immature granulocytes were present. Erythroid immaturity was demonstrated with morphology and circulating nucleated RBCs. Abnormalities in granulocytic lineages were present with hypogranular neutrophils and pseudo Pelger-Huet morphology.Figure 5. At nearly any age, this bone marrow needle core biopsy on H&E stain would qualify as hypercellular. At low to medium power this is clearly evident. At higher powers, note the presence of predominantly immature granulocytes (with very few, if any, mature PMNs) as well as numerous blasts—on H&E blasts appear differently, but appreciate the increased number of cells with active nuclei, condensing chromatin, and prominent nucleoli. Figure 6. Back to traditional hematology staining, you can still appreciate this bone marrow aspirate’s hypercellularity. There is a labeled megakaryocyte (which appears slightly abnormal) to scale against the numerous, immature and left-shifted granulocytes which overrun the fields. Myeloid blasts are seen in high numbers, with granules and prominent nucleoli. Increased levels of mitotic activity, abundant (and some abnormal) myeloid precursors, and a highly proliferative picture is appreciated.Figure 7. Li-Fraumeni Syndrome (LFS) is a rare genetic predisposition to soft-tissue sarcomas. It is a germline mutation of either TP53 or CHECK2, more often the former. The mutation usually has an autosomal dominant inheritance pattern and has very high penetrance, more so in females (possibly due to the fact that the most common presentation of tumor formation in LFS is breast cancer). Note that this patient had a clinical history significant for both breast carcinoma and osteosarcoma which were treated with chemotherapy and radiation.Figure 8a. Patients with LFS often have a germline mutation in p53, a very significant tumor suppressor gene, which is implicated in a wide host of cellular functions. Located on the short arm of Chromosome 17, when mutated this gene affects a myriad of pathways including cell senescence, growth cycle response, proliferation, DNA damage repair from mutations, epigenetic, or exogenous causes, and programmed cell death. If this downstream protection against severe DNA compromise is lost, this becomes a highly pre-cancerous environment for Knudsen’s “second hit” to negatively affect cells and ultimately lead to a vast array of malignancies. Figure 8b. I mean just look! P53 is a serious player in cell survival and DNA damage recovery. It is the archetype example of a tumor suppressor gene and is implicated in an ever-growing number of cell survival and growth cycle pathways—of course a loss of p53 function would set the stage for high-risk.Figure 9a. The World Health Organization (WHO) and its updated guidelines for diagnosing and addressing hematologic malignancies now includes a lot of new data regarding the molecular biology of cancer. Its applications to diagnostics in hematopathology are growing daily. In these guidelines, the WHO classify AML into seven general categories. For reasons relating to her clinical history of cancers and treatment, as well as the timeline she presented with, t-MN or therapy-related myeloid neoplasm would be an appropriate diagnosis. Figure 9b. The American Society of Hematology (ASH) and the College of American Pathologists (CAP) co-wrote guidelines for the diagnosis of AML and published a number of recommendations in The Hematologist in 2017-2018. Essentially, proper laboratory test utilization and incorporation with significant clinical history is crucial. Staying organized and operating within WHO guidelines for hematologic malignancy diagnosis is just as important. The ASH/CAP guidelines tell diagnosticians to think about several key questions when approaching AML which further underscores the values of consistency, efficiency, and appropriate utilization.Figure 10a. The reason for establishing a diagnosis of therapy-related AML is a significant one. The use of Topoisomerase II inhibitors, alkylating agents, antimetabolites, and radiation therapy all affect the genetic components relating to this particular leukemia. To correlate further, the patient had a 5q deletion, a complex karyotype, a history of receiving all treatments related to this entity, and a presentation of myelodysplasia which rapidly progressed to AML.Figure 10b. LFS can cause leukemia on its own, AML can present as a hematologic malignancy on its own too; but this patient’s clinical history and treatment history lean the diagnosis away from de novo cancer to a myeloid process in response to a latent treatment effect.
Why All of This
Matters
There are two main reasons why all of this is important
enough to discuss in a case conference. First, as clinicians from the bench to
the bedside we should all strive to talk through the toughest diagnoses and
share with each other what best practices, lessons, and goals we can reach
together. In the setting of Li-Fraumeni Syndrome it becomes critical to
evaluate new onset (especially myeloid) neoplasms. TP53 mutations are associated with the lowest survival rates in
acute myeloid leukemia, which has its own diagnostic and prognostic
classifications set forth by the World Health Organization. Furthermore,
understanding appropriate patient history, clinical information, and what
appropriate lab investigation means is crucial. It not only keeps the needs and
interests of the patient first, but also translates to the proper utilization
of resources for the best results in the best timelines. Potential future
implications of concurrent ongoing work in hematopathology and molecular
genetics may yield therapeutic and diagnostic benefits we are not yet aware
of—we must constantly include updates as we practice.
Second, this was an opportunity to share insights into the
diagnosis and discussion of AML that came from my clinical experiences before
rotating there. I previously mentioned the demonstrated value of including
clinical viewpoints for the benefit of patient care outcomes, so appropriately
I incorporated these topics into this case conference and included the
following points to consider:
Hematologic
premetastatic niches
When I was in graduate school at Rush
University in Chicago, I did some research in hematopoietic responses to
various therapies in the context of proliferation and understanding
mobilization for transplant and engraftment. In this work, I became familiar
with the concept of a reactive stroma and a “pre-metastatic niche.” There are
small microenvironments in which hematopoietic, mesenchymal, and endothelial
cell lines in the bone marrow thrive and develop which are full of cytokines
and cell-cell interactions. My work focused on mobilizing all three lines with
a CXCR4 target, but the concept holds true when considering germline and
somatic mutability. In effect, those cells with pre-malignant mutations can
cluster and affect the environment of other cells maturing in the same setting.
The same way invasive cells can break through barriers to metastasize and
spread past their in situ conditions,
the same mobilizing spread can grow from pre-metastatic clusters. This, again,
opens the discussion for treatment targets in future LFS and/or AML patients as
molecular pathology expands.
Acute
Myeloid Leukemia and Myeloid Sarcoma
In a recently published paper in Histopathology, I was part of a team at
the UAB hospital’s department of pathology which discussed their experience
with patients diagnosed with myeloid sarcomas (MS). The point was to look for
correlations with MS to connect the entity with age, sex, location of tumor,
AML status, genetics, etc. Ultimately, what became the highest predictor of
disease was a complex karyotype, consistent with other concurrent literature.
With respect to this patient, what if there was another soft tissue (or other
location) sarcoma alongside her myelodysplastic picture. What if she had a low
blast count, or hypocellular bone marrow, or necrosis/fibrosis, or had received
G-CSF? Would AML with myeloid sarcoma be considered in this diagnostic setting,
would myeloid sarcoma be something to worry about in her future or in her
clinical history as a misdiagnosis? The take-home message would be to pay close
attention to patient clinical history and stay both focused on the current
diagnostic work-up but also open enough to avoid pitfalls in diagnostic
challenges.
Misdiagnosis
in clinical settings
In a case report from 2017 I discussed a
patient who had bilateral lung nodules several years after being treated for
breast carcinoma. It was initially thought to be relapse but was later
correctly diagnosed as de novo
peripheral T-cell lymphoma (PTCL). This could have very well been the same
clinical scenario, with a different cell lineage. The lesson gleaned here is
the same as those ASH/CAP guidelines: stay organized, consistent, and
purposeful with your testing and investigation. What came down to a few
immunohistochemical markers in this PTCL case could make all the difference in
another case. Missing the clinical history and specific genetic mutations
present in this LFS/AML patient could have led to a diagnosis of a
myelodysplasia related AML instead of a therapy-related one, especially in the
setting of such a severe germline pre-disposition.
Future
plans for this patient
I thought it was ultimately important to
discuss the patient’s future plans with the audience. In pathology we often
sign-off after we sign-out. So, in order to make sure we emphasize the
patient’s best interests moving forward from a poor prognostic diagnosis, we
discussed her enrollment in a trial aimed at improving bone marrow donor
matching based on HLA and KIR combination typing. This a relatively new and
promising concept in the literature which I hold high hopes for.
If anything, this was something I learned last month: in
order for you to call the quality of care the highest possible, you have to
uphold many standards, both clinical and non-clinical. Clinically we all have
to share with each other the latest and greatest in modern literature and
advances in interdisciplinary or translational research. Aside from this,
however, we have to keep each other human and connected to our patients. I
never like to hear the stereotypes
in pathology that place us in lab medicine miles away from patient care;
instead, we do things every day that impact our patients’ lives greatly. And
when we keep ourselves connected to that fact, like the philosophy at the Mayo
Clinic, then we can boast our quality of care—from small community hospital to
academic trauma center. Because its not the size of the lens on the scope, it’s
the vast scope of impact we look through in a lens of compassion.
There you have it. That’s my month at Mayo and a case conference in a nutshell. It was a fantastic experience and I have to say it—I had a blast!
Thanks for reading, I’ll see you next time!
And have a Happy Lab Week 2019!
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student actively involved in public health and laboratory medicine, conducting clinicals at Bronx-Care Hospital Center in New York City.
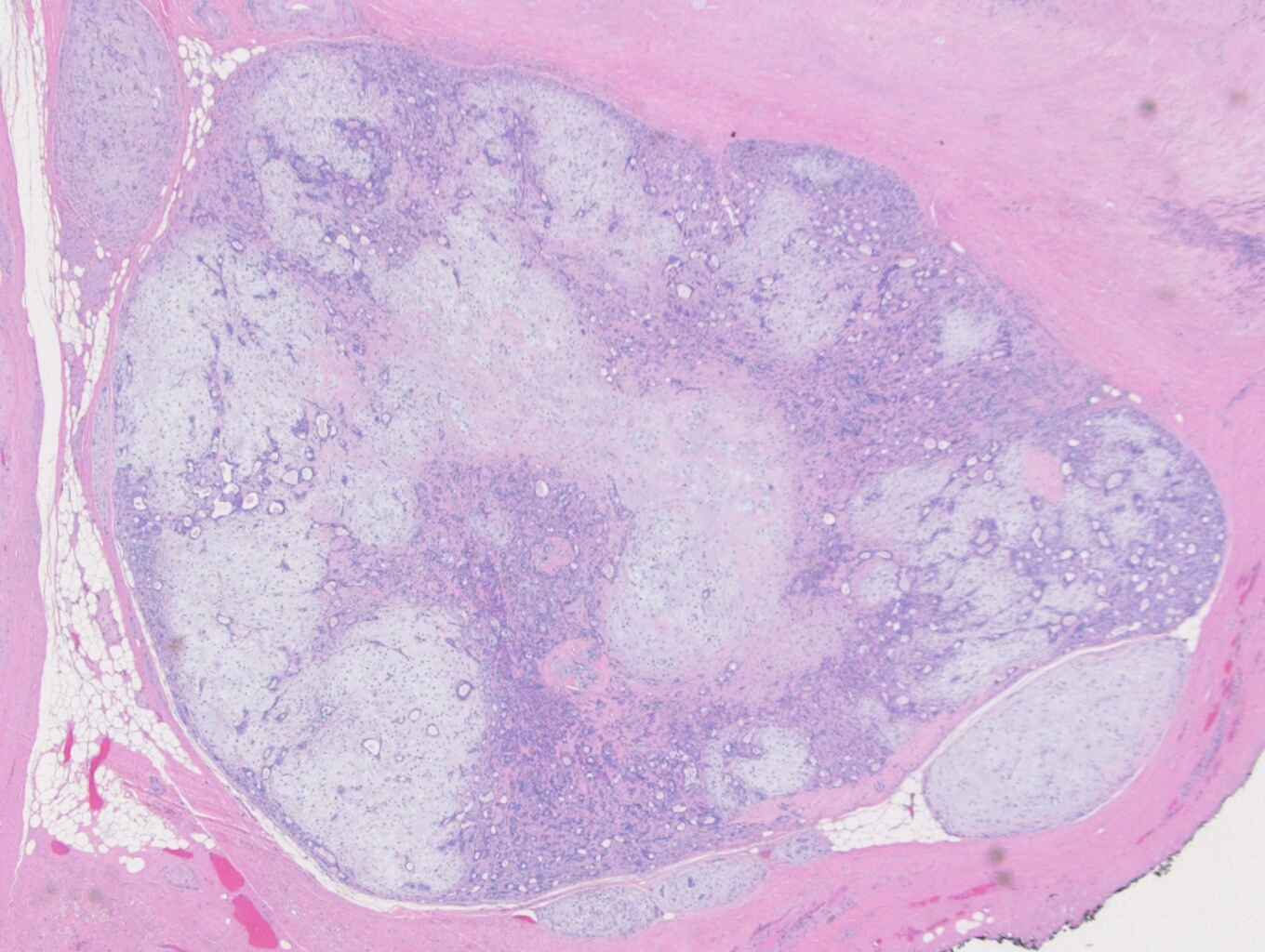
A 63 year old man presented with a long standing history
of a recurring pleomorphic adenoma of the parotid gland. As a child, the
patient had radiotherapy to the bilateral parotid glands for parotid swelling. He
then developed a left parotid mass ~15 years later and underwent parotidectomy. After
another recurrence ~15 years after the initial parotidectomy, he underwent a
second resection of multiple masses in the preauricular region. The patient
then developed a recurrence ~20 years after the second resection and underwent
neutron beam therapy. The patient tolerated the treatment well noting mild dry
mouth, which is persistent, and left ear pain, but otherwise has no major
long-term sequelae from the treatment. Eighteen years after the neutron beam
therapy, the patient developed a left submandibular mass. A subsequent biopsy
of the mass revealed a pleomorphic adenoma. Enlarged left and right submental and
submandibular nodes were noted, with biopsies performed at an outside hospital
of these nodes demonstrating metastatic poorly differentiated carcinoma within
three lymph nodes. It was noted on this pathology report that the histological
features, in light of the history, could represent a carcinoma ex pleomorphic
adenoma. A CT scan of the head and neck revealed a large multiloculated, cystic,
rim-enhancing mass within the left parotid gland, as well as large enhancing
lymph nodes within the right anterior and posterior cervical triangle and the
right submandibular space, the largest of which measured 2.1 cm. A PET scan
showed increased activity within the right neck. Upon meeting with
otolaryngology, a 4.0 x 7.0 cm lobular, non-fixed left parotid mass, and two
level 1B right sided nodes, were palpated. Based on the patient’s history,
physical exam, and prior biopsy results, it was decided to proceed with a parotidectomy
and bilateral neck dissection.
Diagnosis
Received
in the Surgical Pathology laboratory is a soft tissue mass resection from the
area of the left parotid gland measuring 9.0 x 6.0 x 4.2 cm. The specimen is
oriented by a single long stitch designating the superior aspect, and a double
long stitch designating the lateral aspect (Figure 1). The specimen is entirely
inked black, and then bisected to reveal multiple discrete, white-tan,
partially cystic masses ranging in size from 0.2-4.0 cm in greatest dimension and
measuring 7.0 x 3.5 x 3.0 cm in aggregate dimension (Figure 2). The largest
mass is partially cystic with the cystic component measuring 1.2 cm in greatest
dimension. This largest mass abuts the anterior, medial and lateral margins. The
remaining tumor deposits are located:
– 1.2 cm
from the inferior margin
– 0.4 cm
from the superior margin
– 0.9 cm
from the posterior margin
No gross
salivary gland tissue is identified. The remainder of the specimen consists of
unremarkable yellow adipose tissue and red-brown skeletal muscle. The specimen
is submitted as follows.
Cassette
1: superior margin
Cassette
2: representative sections of
anterior margin
Cassette
3: anterior superior margin
Cassette
4: anterior inferior margin
Cassette
5: posterior margin
Cassette
6-9: representative sections of mass
with approach to lateral margin
Cassette
10: representative sections of mass
with approach to medial margin
Cassette
11: mass in relation to
surrounding skeletal muscle
Cassette12-15: representative sections of mass
On
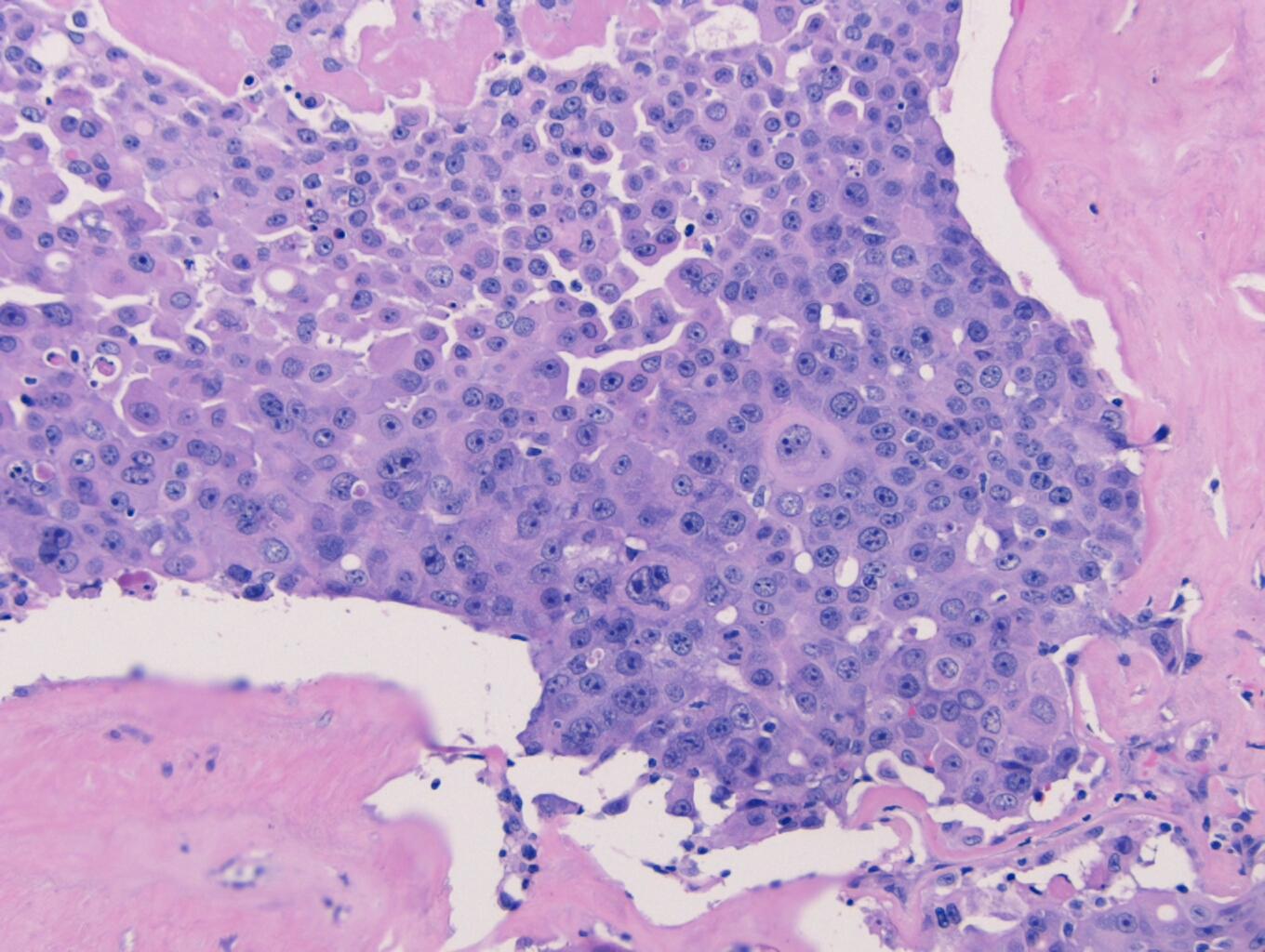
microscopy, the specimen contains nests of tumor cells ranging in size from 0.2
to 4.0 cm within a dense fibrous matrix. Although these deposits may represent
lymph node metastases, no residual lymphoid tissue is present. The tumor is
represented by residual pleomorphic adenoma and numerous soft tissue deposits
of pleomorphic adenoma (Figure 3). Admixed are broad areas of high grade
carcinoma with necrosis (Figure 4). Most regions show adenocarcinoma, although
a rare focus of squamous differentiation is also present. The lateral margin is
positive for carcinoma, and a pleomorphic adenoma component approaches within
0.1 cm of the medial margin. The anterior, posterior, inferior, and superior
margins are all free of tumor. No salivary gland tissue is identified.
In
addition, eleven frozen sections are submitted from various areas surrounding
the mass, with five of the eleven frozen sections demonstrating tumor deposits.
A right neck dissection is performed with following results:
Level
IB: 2 of 3 positive (largest deposit: 1.8 cm)
Level II
and III: 1 of 14 positive, Level II (1.9cm)
Level
IV: 1 of 8 positive (2.0 cm)
Based on
these results, the specimen was signed out as carcinoma ex-pleomorphic adenoma,
and designated as pT4aN2cMx
Figure 3. 2x photomicrograph showing a classic appearing pleomorphic adenoma with satellite nodules along the periphery
Discussion
Carcinoma ex pleomorphic adenoma
(CXPA) is a carcinoma that arises in a primary (de novo) or recurrent benign
pleomorphic adenoma (PA). While a PA is the most common salivary gland tumor,
accounting for approximately 80% of all benign salivary gland tumors, a CXPA is
quite uncommon, accounting for only 3.6% of all salivary gland tumors. CXPA is predominantly
found in the sixth to eighth decades of life, with a slight predilection for
females. CXPA arises most commonly in the salivary glands, in particular the
parotid and the submandibular glands. CXPA can also arise in the minor salivary
glands in the oral cavity, although these tumors tend to be smaller than their
counterparts in the parotid and submandibular gland. There have also been cases
of CXPA in the breast, lacrimal gland, trachea, and nasal cavity.
Clinically, CXPA presents as a firm, asymptomatic mass that can go undetected for years since they are not generally invasive. When the patient does experience any symptoms, with pain being the most common, it is usually due to the mass extending to adjacent structures. If the mass was to involve the facial nerve, paresis or palsy can occur. Other signs and symptoms include skin ulceration, mass enlargement, skin fixation, lymphadenopathy, dental pain, and dysphagia. The onset of symptoms can range anywhere from 1 month up to 60 years (such as with this case), with a mean onset of 9 years. Half of patients will have a painless mass for less than 1 year. Since these symptoms are similar to those of a benign PA, it’s important that the treating physician be aware of the possibility of a CXPA, especially considering the rarity of the cancer.
Grossly, CXPA appears as a firm,
ill-defined tumor, and can vary greatly depending on the predominant component.
If the PA is the predominant component, the mass may appear gray-blue and
translucent, and it could be possible to grossly differentiate between the PA
areas and the CXPA areas. If the malignant component predominates, then the
mass may contain cystic, hemorrhagic and necrotic areas.
Microscopically, CXPA is defined as having a mixture of a benign PA, admixed with carcinomatous components. Zbaren et al, in an analysis of 19 CXPA cases, found 21% of the tumors were composed of less than 33% carcinoma, 37% of the tumors were composed of 33-66% carcinoma, and 42% of the tumors were composed of greater than 66% carcinoma. Most often, the malignant component is adenocarcinoma, but can also include adenoid cystic carcinoma, mucoepidermoid carcinoma, salivary duct carcinoma, and other less common variations. In cases where the entire tumor is replaced by carcinoma, the diagnosis of CXPA will be based on the presence of a PA on the previous biopsy. Conversely, you could also have a tumor that is predominately composed of a PA, with sparse areas of malignant transformation, such as nuclear pleomorphism, atypical mitotic figures, hemorrhage and necrosis. The likelihood of malignant transformation increases with the length of the PA being present, from 1.5% at 5 years, up to 10% after 15 years.
CXPA can be further sub-divided into four categories based on the extent of invasion of the carcinomatous component outside the capsule: in-situ, non-invasive, minimally invasive, and invasive carcinoma.
#1) In-situ carcinoma occurs when nuclear pleomorphism and
atypical mitotic figures are found within the epithelial cells, but do not
extend out beyond the border of the myoepithelial cells (Figure 5).
#2) Non-invasive CXPA, which can include in-situ carcinoma,
is maintained within the fibrous capsule of the PA, but extends beyond the
confines of the myoepithelial cells. Non-invasive CXPA may begin to show
malignant transformation, but will overall behave like a benign PA.
#3) Minimally invasive CXPA is defined as <1.5 mm
extension into the extracapsular tissue, with a mix of benign PA components and
carcinomatous components.
#4) Invasive CXPA is defined as a > 1.5 mm extension into
the extracapsular tissue, and will begin to demonstrate more carcinomatous
components, such as hemorrhage and necrosis.
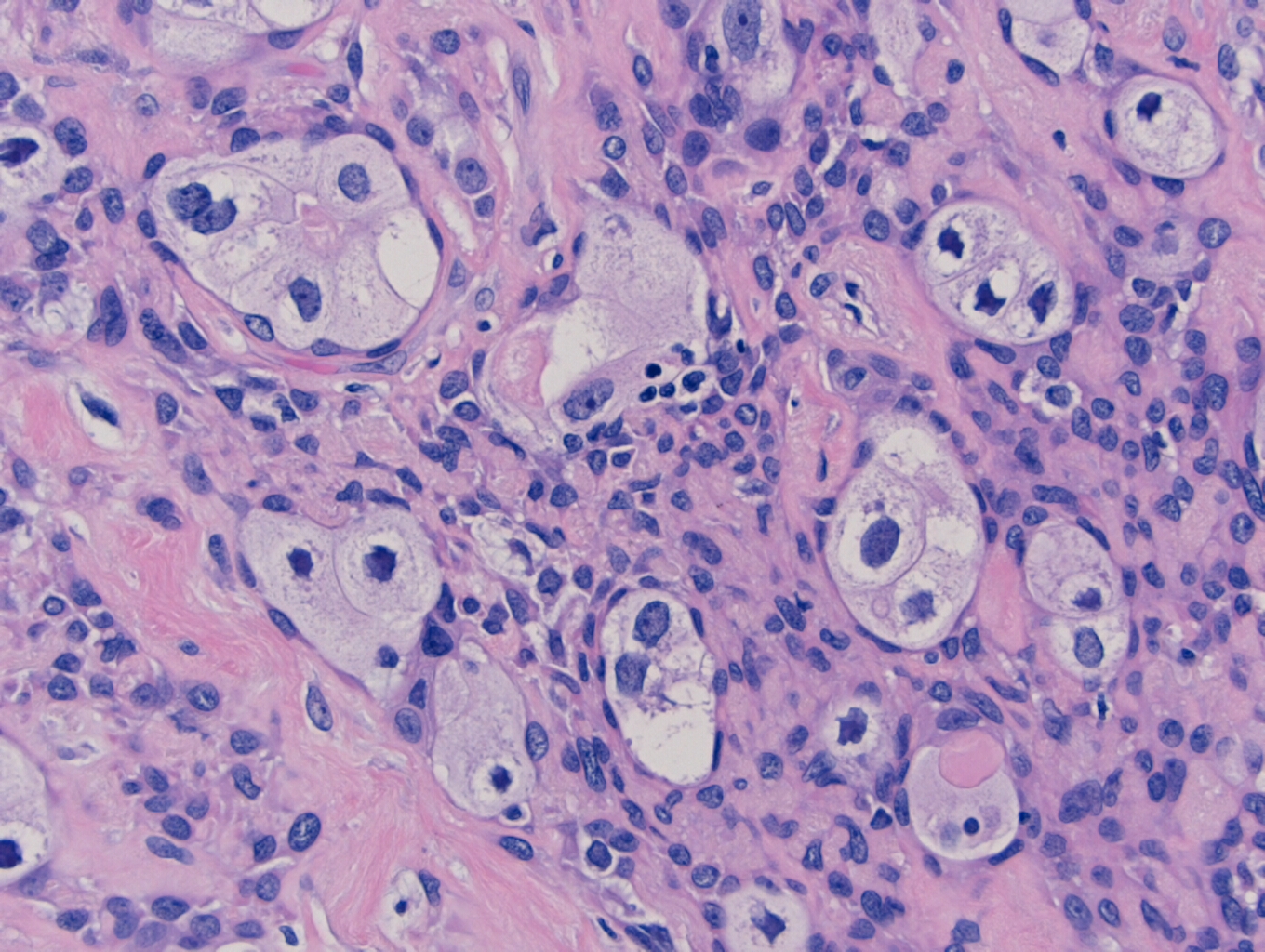
As the carcinomatous areas begin
to increase in prevalence, the PA nodules will begin to be composed of
hyalinized tissue with sparse, scattered ductal structures, and the malignant
cells will begin to decrease in size as they move away from the site of origin.
Perineural and vascular invasion can be easily identified as the tumor extends
into the neighboring tissue (Figure 6).
The development of CXPA has been
shown to follow a multi-step model of carcinogenesis with a loss of
heterozygosity at chromosomal arms 8q, followed by 12q, and finally 17p. Both
PA and CXPA demonstrate the same loss of heterozygosity, however, the carcinomatous
components exhibit a slightly higher loss of heterozygosity at 8q, and a
significantly higher loss of heterozygosity at 12q and 17q. The early
alterations of the chromosomal arm 8q in a PA often involves PLAG1 and MYC,
with the malignant transformation of the PA to a CXPA being associated with the
12q genes HMGA2 and MDM2.
Treatment for CXPA involves
surgery, radiotherapy and chemotherapy, with a parotidectomy being the most
common procedure performed. If a benign PA had originally been resected, but
residual remnants of the PA were left behind, then satellite PA nodules will
arise in its place (Figure 3). If in-situ, non-invasive or minimally invasive
carcinoma is suspected in the superficial lobe of the parotid gland, than a
superficial parotidectomy can be performed. Invasive carcinoma will result in a
total parotidectomy, with every attempt made to try and preserve the facial
nerve. If metastasis is suspected to the cervical lymph nodes, a neck
dissection may also be performed. Reconstructive surgery following the removal
of the tumor may be necessary, depending on where the tumor was resected from. Other
treatment options currently being considered include a combination therapy of trastuzumab
and capecitabine, as well as the possibility of a WT1 peptide based
immunotherapy.
Figure 5. 40x microphotograph demonstrating an in-situ carcinoma confined within the myoepithelial cells Figure 6. 10x photomicrograph of carcinoma at the lateral margin with areas of perineural invasion
References
Antony J, Gopalan V, Smith RA, Lam AK. Carcinoma ex pleomorphic adenoma: a comprehensive review of clinical, pathological and molecular data. Head Neck Pathol. 2011;6(1):1–9. doi:10.1007/s12105-011-0281-z
Chooback N, Shen Y, Jones M, et al. Carcinoma ex pleomorphic adenoma: case report and options for systemic therapy. Curr Oncol. 2017;24(3):e251–e254. doi:10.3747/co.24.3588
Di Palma S. Carcinoma ex pleomorphic adenoma, with particular emphasis on early lesions. Head Neck Pathol. 2013;7 Suppl 1(Suppl 1):S68–S76. doi:10.1007/s12105-013-0454-z
-Cory Nash is a board certified Pathologists’ Assistant, specializing in surgical and gross pathology. He currently works as a Pathologists’ Assistant at the University of Chicago Medical Center. His job involves the macroscopic examination, dissection and tissue submission of surgical specimens, ranging from biopsies to multi-organ resections. Cory has a special interest in head and neck pathology, as well as bone and soft tissue pathology. Cory can be followed on twitter at @iplaywithorgans.
Last
month we discussed the rules and requirements for how to properly perform
proficiency testing (PT) within your laboratory. In part 2 of this 3-part
series we’ll review the rules associated with evaluating your results, and how
to investigate any unsuccessful surveys. Still to come in part 3 we will look
into how to utilize your PT results to monitor for trends and shifts in your
values.
The
rules:
Performance Review: Laboratories must initiate and document a review of their PT performance evaluations within 2 weeks of notification that results are available. This includes a review of both graded and non-graded/educational analytes and events as well.
Key
things to note: Even though educational samples are not formally graded, you
should still verify the accuracy of your results, with appropriate follow-up
for any failures. CAP specifically requires you to evaluate these educational
challenges as well. Whether the sample is graded or not does not change the
fact that you had an incorrect result.
Unsatisfactory Performance: For any unsatisfactory results,
you are required to perform a root cause analysis to determine why (see below
for guidance). This also includes any clerical errors – you need to evaluate
your process and find ways to prevent these simple errors from happening again.
If they are happening with PT samples, it is possible they are happening with
patient samples as well.
Cessation of Patient Testing: Unsatisfactory events indicate
that there was a problem with that particular survey; whereas unsuccessful events indicate
there has been a pattern of unsatisfactory events/samples and a larger problem
exists. If a pattern of poor performance is detected, you may be asked by your
local state department of health to cease all testing for a particular analyte.
Key
things to note: This also applies to clerical errors. Even if there was no
technical problem with the accuracy of your results, failure to submit results
on time or clerical errors made while submitting can also have severe impacts
on your ability to continue offering that test.
Remedial Action: If you’ve been notified by your
PT provider or state DOH to cease testing, there are extensive steps that must be
completed to prove that the problem was correctly identified and corrected. You
must also identify where samples will be referred to for tests you are unable
to perform in-house.
Key
things to note: If testing has been removed from your laboratory, you will be
required to demonstrate successful performance in 2 consecutive PT survey
events for the analyte(s) in question before being granted permission to resume
patient testing. This can cause significant delays and financial impact for
your organization.
Root Cause Analysis: Investigate to determine who,
what, why, when, and how the event occurred. Be sure to evaluate all phases of
testing to ensure you identify all potential causes.
Pre-Examination:
Human Resources – evaluate the training and competency records for staff involved in the handling and testing of samples.
Facilities – reagent inventory control & storage temperatures, equipment maintenance and function checks
Standard Operating Procedures (SOPs) – staff compliance with written policies, bench excerpts are current and valid, document version control up to date
Specimen –test requisition/order entry (was the correct test code ordered/performed?), labeling (were aliquot/pour off tubes properly labeled?), transport (was appropriate temperature requirements maintained until testing performed), quality (was there visible deterioration with the sample prior to testing or cracked/damaged tubes received?), quantity (was the original sample spilled or leaking causing an incomplete aspiration of sample by your instrument?)
Examination:
Method
Validations – were instruments current with calibration requirements, any bias
noted during instrument correlation studies, values being reported within the
verified AMR
Environmental
Controls – temperatures/humidity within tolerance limits, for light sensitive
studies (bilirubin) was there excessive exposure of the samples to light prior
to testing, excessive vibrations occurring that may have affected results
(nearby construction or a running centrifuge on a shared work bench)
Quality
Control – did QC pass on the day of testing, was QC trending or shifts noted
that month
Analytical
Records (worksheets) – were sample results transcribed correctly between the
analyzer and worksheet, between the worksheet and LIS
Instrument
Errors – were any corrective actions or problems noted for the days before,
during, or immediately after testing of PT occurred
Testing
Delay, Testing Errors – were samples prepared and not tested immediately
leaving them exposed to light or air which may affect results (blood gas
samples), any errors or problems noted during testing that may have caused a
delay or affected accuracy of results
Post-Examination:
Data
& Results Review – check for clerical errors, was data trasmitted correctly
from the instrument into LIS, was data entered correctly on your PT provider
entry submission forms
Verification
of Transmission – did your results correctly upload to the PT provider website,
was there an error or failure with submission
Review
of LIS – are your autoverification rules set up correctly, is the
autoverification validation current with no known issues
Patient
Impact – perhaps
the most important step to take when reviewing PT failures, you need to
determine what impact your failure had on your patient results. Depending upon
the identified root cause and how different your values were from the intended
response, this can potentially pose a severe impact on your patient values
tested at the same time as the PT samples.
Involve
your medical director to determine if the discrepancy in results is clinically
significant. Perform a patient look-back to review patient values for the same
analyte with the failure during the time period in question. Evaluate the bias
that was present, and if deemed to be clinically significant then corrected
patient reports will need to be issued with a letter from the medical director
explaining why. If it was decided that the discrepancy is not clinically
significant, document this in writing and keep on record with your complete
investigation response.
Corrective Actions/Preventative
Actions– use the following set of questions to help guide you
in ensuring that the problem identified during your root cause analysis will
not occur again:
What
changes to policies, procedures, and/or processes will you implement to ensure
there will not be a repeat of this problem?
Do
any processes need to be simplified or standardized?
Is
additional training or competency assessment needed? If so, identify specific
team members to be trained, and who will be accountable for performing and
documenting this training.
Is
additional supervisory oversight needed for a particular area or step?
Are
current staffing levels adequate to handle testing volumes?
Would
revision or additional verification of the LIS rules address or prevent this
problem?
How
can the communication between laboratory, nursing, and medical staff be
improved to reduce errors in the future?
Continuous Process
Improvement –
after identifying the true root cause(s) for the failure and implementing corrective/preventative
actions, you need to evaluate the effectiveness of those improvements. Have
they been sustained? Are they working to correct the original problem? Have you
created new problems by changing the previous process?
Quality
Management Meetings – if necessary, increase the frequency of these meetings
during the evaluation period for timely feedback to management and staff
Implement
internal audits and quality indicators to check for potential issues
Access
the specimen transport conditions to ensure they meet test requirements
Evaluate
and monitor your turnaround time metrics to track problem specimens and impact
of testing delays
If
necessary, increase the frequency when QC is performed or calibration frequency
if stability issues are identified
Performing
a thorough root cause analysis for any failures will allow you to implement
appropriate corrective actions that will address the true issues. Having a
robust quality management program will help ensure these issues are identified
and corrected in a timely manner, and reduce the potential for the dreaded
Cessation of Patient Testing letter from your local DOH.
Coming
up in the final installment of this series on PT testing, we’ll review all of
the quality indicators and data that can be found in your PT evaluation reports
to help ensure you’re on track for accurate patient values.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s 2018
Top 5 in the 40 Under Forty recognition program. She has worked in the
medical laboratory profession for over 18 years. In her current
position, she transitions between performing laboratory audits across
the entire Northwell Health System on Long Island, NY, consulting for
at-risk laboratories outside of Northwell Health, bringing laboratories
up to regulatory standards, and acting as supervisor and mentor in labs
with management gaps.
Outside the city of New Bern, in Craven County, North
Carolina, there is a particular system for residents to dispose of their
garbage. Locals must go to the nearest participating gas station and purchase
stickers which cost about $2.00 each. These stickers must be placed on each bag
of garbage generated in the household, otherwise they will not be picked up
during the weekly trash collection. In order to save money, a group of widows
has formed a club in which members scout out the open dumpsters in town
(usually behind stores or gas stations). Then they call and let group members
know where they can covertly dump their trash for free that week.
This story may seem funny, but for the most part, it is
true. I have no doubt this also occurs in other parts of the country where the
system for trash collection is similar. Why do people behave this way? Are they
purposely trying to circumvent the trash collection system in place or is the
system just not easy for locals to utilize? If you’re having difficulty getting
people to change safety behaviors (like PPE compliance) in your laboratory, you
might need to determine that for the systems you have in place and ask similar
questions.
In one laboratory the manager struggles with staff who work
part of the day in a clean office and another part in the lab itself. When the
employees go into the lab for brief periods, they often fail to don their PPE.
Upon further investigation, you would learn that staff are not allowed to keep
their lab coats on their chairs and that all PPE is kept in one lab store room
located on the opposite side away from the offices. The system is set up to reinforce
PPE non-compliance.
In another lab the manager placed a permanently-mounted
counter face shield in the chemistry department so that staff would be forced
to use it when popping specimen caps. Staff loaded instrument racks behind the
shield, but when they carried the racks over to the analyzers, their faces were
not protected from splashing. Exposures continued to occur. Here the system is
at play again. A face shield was put in place to change behaviors, but it was
only a partial solution. In order to protect staff fully here, they would need
goggles or a face shield that can be worn. Offer light-weight reusable or
disposable face protection that staff can use easily. Be sure to give them a
say in whatever option is chosen.
Sometimes the system issues are not apparent until there is
a safety event, and unfortunately, that can result in bigger problems. If your
training program does not include regular fire safety training, a small fire
situation may get out of hand quickly. Does your staff have experience handling
a fire extinguisher? Would they easily be able to put out a fire? Do they know
their evacuation routes and meeting places, and could they get there with ease?
What about the lab emergency management plan? Have staff participated in a
table-top drill so they have a basic understanding of how to respond during a
chaotic disaster? These are examples of some safety systems that need to be in
place to keep staff ready and safe at all times.
When people take shortcuts or find ways to circumvent the system, there is usually a pretty good reason, Often, it is the design of the system. In New Bern, elderly women can’t lift large heavy trash bags, so they use smaller bags. They don’t want to pay the same price for a garbage bag sticker that others are paying for big bags. There’s a problem with the system- and those ladies found a way around it. What problems do you see in your lab safety system? If you don’t know what they are, ask around. Staff will talk. It’s better to find out what the workarounds are now and to fix them before an injury or exposure occurs.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years
experience as a certified medical technologist. Today he is the
Laboratory Safety Officer for Sentara Healthcare, a system of seven
hospitals and over 20 laboratories and draw sites in the Tidewater area
of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Jennison Hartong, MLS(ASCP)CM,
PA(ASCP)CM, is a Pathologists’ Assistant who recently went to
Ethiopia to teach grossing techniques. The editors of Lablogatory asked her a
few questions about her experiences.
Lablogatory: How’d you get involved with ASCP’s Center for Global Health?
Jennison: Dr. Milner, Chief Medical Officer of ASCP, initially reached out to one of the pathologists at M.D. Anderson to inquire if any Pathologists’ Assistants (PAs) would be interested in attending a workshop in Nigeria. I reached out and expressed my interest in teaching grossing techniques rather than public speaking (not one of my strengths). Dr. Milner then told me about this opportunity in Ethiopia where pathologists were requesting advanced, gross training in lymph node dissections on breast and colon specimens. I immediately jumped at the opportunity to help in this way.
L: What were your motivations for going?
J: Whether with basic health needs or more complex areas like cancer treatments, I’ve always wanted to use my education and experience to help others and impact lives in areas around the world where certain aspects of healthcare may not be accessible. Before becoming a PA, I was a medical technologist and was always interested in working with Doctors Without Borders, however, I did not have the years of experience to apply. I decided to go to PA school and was disappointed to learn that Doctors Without Borders does not utilize PAs. I figured that dream would have to be accomplished another way, which was why I was so eager to work with the ASCP and their global health initiatives.
Another motivation for going on this trip was
experiencing the work and organizational skills required for making a trip like
this successful. I am currently finishing my second master’s degree in public
health with a focus in health policy and management. I was very interested in
learning everything I could about planning programs to help developing
countries as well as being able to network with like-minded health
professionals.
L: What did you hope to accomplish while you were there?
J: My main goal of this trip was to help advance Ethiopian residents and pathologists in certain grossing techniques. More specifically, I aimed to assist with lymph node dissections and, as it turned out, how to locate and sample the radial margin in colon cancer cases. I also wanted to experience a different culture than my own, step out of my comfort zone and challenge myself as a PA by teaching others. At the end of this experience, I can say that this trip was definitely a life changing experience and one I am extremely grateful for.
Image 1. Jennison (black scrubs) training residents from St. Paul Hospital to locate radial margins on colorectal cancer cases.
L: What did you learn about lab medicine in Ethiopia?
J: During my week in Addis Ababa, I quickly realized that it was up to me to make this trip as successful as possible. Never before in my professional career were all the decisions up to me, and at first, it was slightly uncomfortable. I was worried I would come across as too bossy or even condescending. However, after meeting Eshetu Lemma, the ASCP local representative, along with the other participants and experiencing their kindness and eagerness to learn, I was newly determined to make this trip an absolutely positive experience for everyone. I made some changes to the training sessions and after the first day, the rest of the week ran smoothly. I learned a lot about how lab medicine is practiced in Ethiopia. I learned that, in the case of a power outage, you carefully set your blade down and wait it out. I learned that resources like aprons and sleeves are not thrown away unless completely used up. I learned that due to cassette shortages, tissue submission is done quite thoughtfully- more so than in the United States. I learned that the overwhelming majority of cancer cases are presented at stage 4 due to issues surrounding resources, fear, myths, and lack of cancer education. But most importantly, I learned that the labs in Addis Ababa, Ethiopia, are doing an amazing job with the resources they are given and are eager for opportunities to positively impact patient care.
L: Is what you learned there applicable to your work in the States?
J: I’ll take what I learned there and incorporate it into my work here in the States. I’ve gained confidence in my ability as a health professional and reignited my passion to help others.
To put it simply, this trip has been life
changing. It has allowed me to experience and accomplish a lifelong dream for
which I am forever grateful. I’m hopeful that my future holds more
opportunities to serve other communities and help strengthen cancer programs in
developing countries.
Image 2. View from St. Paul Hospital.
-Jennison Hartong,MLS(ASCP)CM, PA(ASCP)CM is a board certified Pathologists’ Assistant, specializing in surgical and gross pathology working mainly in oncology cases. Before attending graduate school, she worked as a Medical Laboratory Scientist (MLS) at Lurie Children’s Hospital of Chicago, Illinois. Upon graduating, Jennison started working at Memorial Sloan Kettering Cancer Center. In 2018, she relocated to Houston and currently works at M. D. Anderson Cancer Center in Houston, Texas. In May of 2019, Jennison will graduate with a second Master’s in public health with a focus in health policy and management from New York Medical College. She plans to use her extensive lab experience and newfound knowledge of public health to help bring basic healthcare to communities that would otherwise not have access to these necessities.
Maryam Zenali1*, Dmitriy Akselrod2, Eric Ganguly3, Eswar Tipirneni4 and Christopher J. Anker5*
1
Department of
Pathology, 2 Department of Radiology, 3 Division of
Gastroenterology, and 5 Division of Radiation Oncology, The
University of Vermont Medical Center (UVMMC), Burlington, VT and 4
Department of Hematology Oncology, Central Vermont Medical Center (CVMC), The
University Of Vermont Health Network, Adult Primary Care, Berlin, VT
*corresponding authors
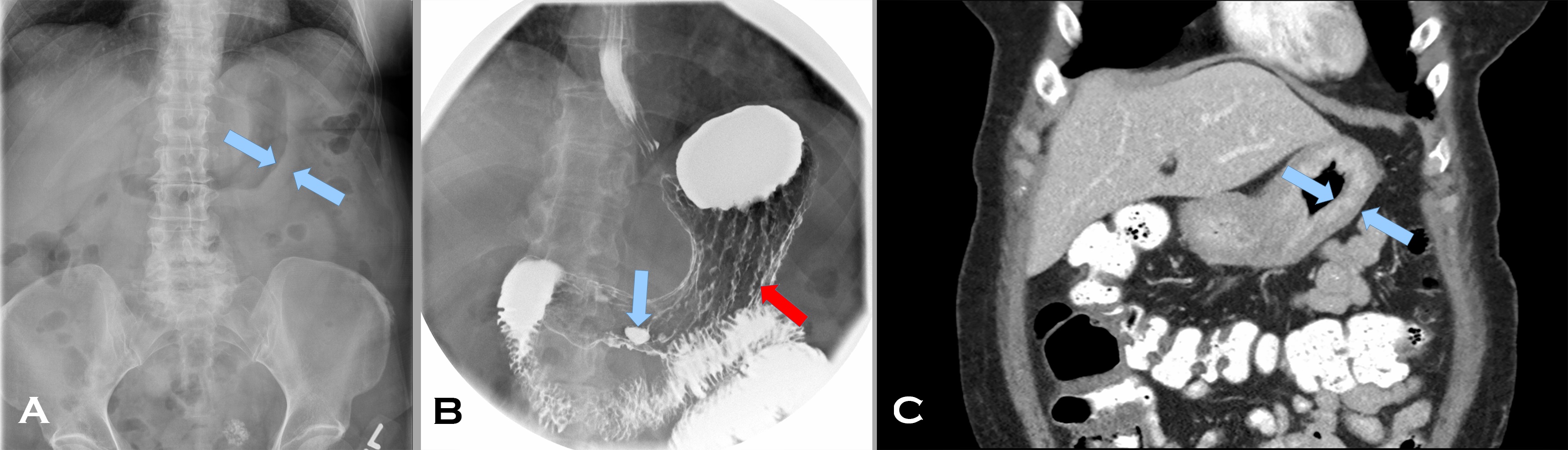
A 57 year old woman with a personal and family history of breast cancer presented with early satiety and dysphagia for 5 months. Her abdominal computed tomography (CT) scan (Image 1 A) showed marked thickening of an apparently featureless gastric wall (A, blue arrows indicating the mucosal [rightward pointing] and serosal [leftward pointing] aspects of the gastric wall). Prominent gastrohepatic lymph nodes were noted as well. Her fluoroscopic upper GI study (Image1 B), following administration of barium and effervescent crystals (a double contrast effect to allow for mucosal evaluation), showed thickened rugal folds (B red arrow) and pooling of barium within an antral ulcer (B blue arrow). A subsequent CT scan (Image 1 C) after administration of intravenous and enteric contrast, confirmed marked diffuse gastric wall thickening (C blue arrows again indicating the mucosal [rightward pointing] and serosal [leftward pointing] aspects of the gastric wall) (Image 1, composite radiographs A-C).
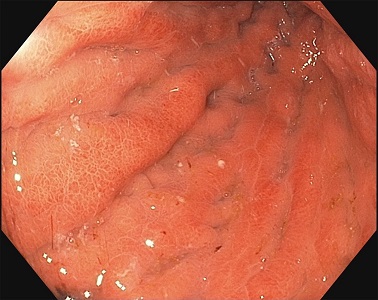
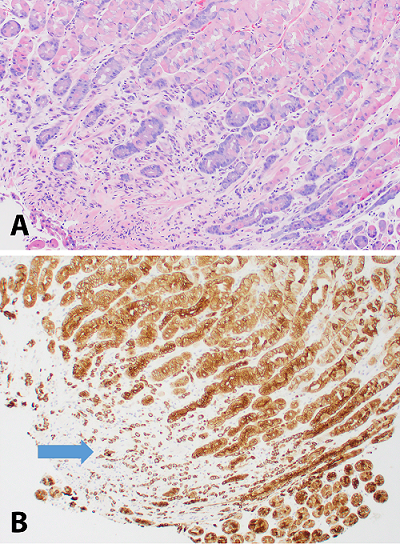
The gastric body distended poorly with insufflation and demonstrated thickened, erythematous, edematous folds with erosions (Image 2, endoscopy image). On endoscopic ultrasound, the total thickness of the stomach was 12 mm with expanded wall layers in the proximal stomach to the antrum and a thickness of 3.5 mm in spared areas. Biopsies were obtained; the corresponding H&E and keratin stains are provided (Image 3, composite photomicrographs A-B).
Image 1. Composite radiographs.
Image 2. Endoscopy image.
Image 3. Composite photomicrographs.
Based on the original radiographic imaging that led to the biopsy, what are the differential diagnoses?
Generation Y is coming and they are coming in strong! It is
fast becoming the world’s largest working generation and their impact on the
workforce will become even clearer in the next few years. These digital natives
find communication natural, in any shape or forms it comes. They prefer texting
and instant messaging, but also appreciate face-to-face meetings and
hand-written notes. They use social media for both personal and professional
use and consider it essential to know how and where to access information.
Instant gratification has become one of this generation’s key values, because
they grew up with the world of information at their fingertips. They value
professional development and feedback and they are at work to learn and grow.
When working with a Millennial the first step is to show
them that you respect them and what they bring to the table. This generation
has received more negative attention than other generations, but they have a
tremendous amount to offer to the workplace (as do all the other generations).
They value collaboration and learning opportunities, so they are typically
quick to adjust when giving constructive feedback. Because of their
collaborative approach, they value inclusion and Social Media to bring people
together. They are well versed in finding information and can typically solve
smaller technological issues without any help.
This generation is focused on having their work mean
something, to have a purpose that is larger than simply getting a paycheck.
They dislike long email and voicemails and anything that is a waste of paper.
They appreciate flexibility and sending documents electronically. They
experiences high academic pressures, so they are comfortable working in a
fast-paced environment. They are comfortable multitasking and handling multiple
projects simultaneously.
Millennials who work in larger organizations are on the
brink of entering leadership positions. However, there are many self-starters
who have had to learn leadership skills along the way. Because this generation
values collaboration, leaders tend to encourage group work and giving people an
acknowledgement for trying. They dislike people who are afraid or do not want
to learn new technology and cynicism as they are a generally very positive
generation.
When working with Millennials, note that they respond well to a participation work environment so ask for their input and suggestions. Be open about any processes, systems, and share information freely. Provide them with lots of feedback to help them learn and grow. Millennials respond well to a faster pace work environment, so do not try to slow them down. They dislike formality and stiffness, so allow flexibility whenever possible. For example, invite them to provide input for their own goals and do not hover over them. Give them multiple things to work on simultaneously so that they can go from project to project when their energy shifts. This generation is crucial to bring your organization to the next level, so mentor them, help them grow and develop and you get their dedication, passion, collaboration, and positivity in return.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
What’s the purpose? That’s the question that most Gen Ys, or
commonly known as Millennials, ask of their job. Why am I here? Can I make a
difference in the world if I remain doing what I am doing?
The Baby Boomers worked because they felt an obligation to
put in a hard day’s work whether they liked doing what they were doing or not. It
was a job. The Generation Xers introduced a focus on work-life balance, which
was not the case for the Baby Boomer. The Boomers never heard of the concept of
“work-life balance” until their children, the Gen Xers, made it a job
requirement and reality.
As for the Millennials, they need to really believe in their
job and what they are doing. Millennials ask questions that the Boomers and Gen
Xers wouldn’t think of asking. This is often misinterpreted as being lazy or
looking for the easy way out. This is not the case. The Millennials took the
best of their predecessors. Most Millennials have a good work ethic and they definitely
look for balance. However, they’re also searching for a purpose.
My favorite story of a Millennial is centered on the importance of taking lunch at work. This topic surfaced from a Roundtable Discussion with laboratory professionals last October 2018, at the ASCP Annual Meeting in Baltimore. The actual topic for this Roundtable Discussion was “diversity.” However, that quickly changed when the nine people at the Roundtable focused on generational differences. This roundtable was rich in generational diversity. The table was comprised of Boomers, Gen Xers and Millennials. Boomers stated that they found it both necessary and easy to work through lunch. Why? It’s because they pride themselves in their incredible work ethic. The Boomers praised themselves for being better than “most Millennials” who often don’t and won’t work through lunch. Instead of that mindset, perhaps the better approach would be “What can we learn from Millennials in the work place?” That answer is “purpose and balance.”
-Catherine Stakenas, MA, is the Senior Director of Organizational
Leadership and Development and Performance Management at ASCP. She is
certified in the use and interpretation of 28 self-assessment
instruments and has designed and taught masters and doctoral level
students.
I had the pleasure of talking recently with Danny Milner, Jr., MD, MSc(Epi), who serves as the Chief Medical Officer of ASCP. He has worked to improve diagnostic access and improve laboratory medicine services in low- and middle-income countries [LMICs] his entire career. I recently read his book for which he served as editor for titled “Global Health and Pathology.” This highly informative compilation of articles written by the foremost experts in the field is a MUST READ for anyone interested in global health! You can order your copy here: https://www.elsevier.com/books/global-health-and-pathology-an-issue-of-the-clinics-in-laboratory-medicine/milner/978-0-323-58158-5.
After reading the book, I hoped to learn more about Dr.
Milner and how he became a leader in global health and pathology. Below you
will find his fascinating narrative of his career and his reflections on the
importance of providing high quality pathology services worldwide.
Q: Dr. Milner,I’m curious to know where your service in
global health began and how your career in pathology has intersected with that?
A: Truly, many
events occurred that were serendipitous in shaping my career and life. I grew
up very poor in a rural community in Alabama, in an area known as the
“black-belt” of the southern states due to the rich black soil found there.
This area was home to many of the relocated former slaves after the end of the
civil war and is now home to a 50/50 mix of Caucasian and African-American members
of the community.
Towards the end of high school, I was awarded a scholarship
for high achievement and a scholarship geared to support healthcare
careers. At the award ceremony, a person
giving me an unrelated award knew of my scholarship for pre-med and said to me
and the crowd, “go become a doctor”. When I was in college, I worked as a
nurse’s assistant for a physician and became interested initially in primary
care . After some careful consideration, I decided to embark on a path that
would take me to medical school, finishing my pre-med requisites and graduating
in three years. I was accepted to the MD/PhD program at the University of Birmingham
[UofB] wanting to do my PhD in Medicinal Chemistry. Unfortunately, this
particular PhD wasn’t allowed, so I decided to pursue a MD only.
In medical school, I decided to slow down my fast track through
school– so I applied to a post-sophomore fellowship in Pathology and at the
same time applied for a summer program offered by UofB that entailed working in
a clinic in The Gambia. This would be the first time that I had traveled outside
the United States. I first went to Africa, with my fellowship to follow on my
return.
In The Gambia, I lived in a compound with 12 people in an extremely
rural area with no running water or electricity. I spent four weeks working in
a clinic with a Gambian doctor, seeing patients without the use of diagnostics.
I was traumatized by the extreme suffering of the patients we saw. My take away
from the experience was the idea that it would have been so much easier to help
had there been any sort of
diagnostics available – a malaria smear, a microscope, anything that could have
helped us do a better job than we were doing.
When I returned from Africa, I started my post-sophomore
fellowship and my first rotation was autopsy. There was a neuropathologist
there named Angelica Oviedo, and she had just gotten back from Malawi. Hearing
about my recent trip to The Gambia, she encouraged me to pursue more work in
global health. She put me in contact with Terrie Taylor – who is an internal medical
physician who has been working in Africa since 1986. It was in the 1990’s and she
had just started a cerebral malaria autopsy study which would become the
largest study on this topic in the world.
This post-sophomore fellowship really inspired me to pursue
pathology. I was thrilled to be offered a position at the Brigham and Women’s
in Massachusetts for pathology residency.
I finished medical school by spending time in Germany and then under the
supervision of Terrie Taylor in Malawi working on the cerebral malaria autopsy
study. I continued to work with her for thirteen years following this.
In residency, it was a natural fit for me to gravitate
towards all things related to global health which meant a focus on infectious
diseases. I continued to work in Africa and traveled there 4-5 times during
residency, scrounging together any time and any money that I could to try to
help. It was during my second time in
Malawi, around 2001, that I was surprised to find that all the cases crossing
the surgical pathology bench were cancer – there was nothing but cancer, and it
was often very advanced. This was 15 years before the WHO resolution on cancer.
I was suddenly very interested in this aspect of care. Up until this point, I
was heavily focused in infectious disease, and how this related to oncology,
but now I wanted to really focus on cancer. I was not encouraged by my elders
to try and tackle this because they said, “they are all going to die anyway.”
Fast forward, I finish a fellowship in Microbiology and am
joining the Brigham as faculty to work in infectious disease pathology. During
this time, I continue to go to Malawi and I am continuously signing out cancer
cases for Africa. This was tragic since there was no intervention at that time,
and every case was essentially a death sentence. The first oncologist did not
arrive in Malawi until somewhere around 2008-2009.
During my time at the Brigham, Partners in Health [PIH]
began sending tissue biopsy cases to us to diagnose. Every year, the cases
increased more and more. Because cancer started to become the majority, PIH
decided to strategize the best way to meet this need. Larry Shulman, the lead
for PIH based at Dana-Farber in Boston, reached out to me to build a pathology
laboratory in Haiti, but since that idea was quickly followed by an epidemic of
cholera, it was decided to build a pathology lab in Rwanda instead – this was
in 2011. After a massive effort entailing equipment installation, capacity
building, infrastructure, and staff training, Butaro Cancer Center officially
opened 6 months later. With the help of a few other volunteers, we continued to
run the lab remotely using static image telepathology. In 2016, a full-time local
pathologist took over the lab and ASCP brought in whole-slide telepathology
services.
In 2015, I met Blair Holladay in person for the
first time. He shared his vision for ASCP to expand their global outreach and
we had a healthy discussion about the details of making it happen. Blair asked
me to volunteer to become part of the team, and I worked together with ASCP to
launch the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
The project grew and ASCP reached out to recruit me to work as the Chief Medical
Officer and lead the global health team. I was excited to have the opportunity
to work in global health full time.
Dr. Milner (left center, front row) with members of the Partners Initiative local team at the 2017 ribbon cutting ceremony to celebrate the opening of the second telepathology lab in Rwanda.
Q: Why is pathology
the essential cornerstone of global health?
A: First, you
should consider how important the laboratory is in medicine. An often-quoted
study says approximately 70% of the clinical decision making is based on
laboratory results. In certain subspecialties of medicine, like surgery or
oncology, these clinicians are nearly 100% dependent on the laboratory for delivering
care. In fields like psychiatry, it is going to be much less dependent on the
laboratory. Even so, it is reasonable to say that almost all medical decisions
are best informed by high quality laboratory results.
Starting with that statement, the laboratory is what allows
clinicians in certain fields to function. In the field of cancer, which is a
major problem in LMICs, you cannot treat the patient without a diagnosis – and
the diagnosis must come from the laboratory.
Q: Historically, pathology
hasn’t always been associated with creating global health solutions. Why do you
think that is now that we know it is an essential component of building health
systems?
A: It’s a general
challenge in global health that pathologists haven’t been involved as much as
they could be. This could be due to multiple reasons. The need for pathologists
to serve in low- and middle-income countries hasn’t traditionally been
recognized. This may be due to a disconnect in understanding our potential to
make an impact. We, like surgeons and radiologists, require electricity,
supplies, and resources in order to volunteer in very remote settings
worldwide. This is unlike clinicians and emergency medical doctors for
instance, that can see patients without extensive resources available – they
are more readily available to serve in small, remote communities. An exception
would be the use of cytology which can, with very limited resources, be
extremely effective even in remote areas. However, as a specialty, pathologists
are typically able to serve in larger cities in LMICs and, there, have an
enormous impact. So, there are plenty of opportunities for pathologists to
practice their specialty in improving global health and make an impact.
It may also be that people and their families have concerns
about their safety, or they don’t have the support of their institution in
terms of time, or they may not feel they have a connection to a potential site.
The desire may be there but there are perceived obstacles.
ASCP works to create relationships and facilitate connections, as well as allay fears for safety concerns. We also offer institutional support, for example, we provide a letter of explanation and support for our Trainee Global Health Fellows. We try to bridge the gaps for people to feel that they have the ability and are empowered to volunteer, remove the barriers to participation, and make it as easy as possible for people to do so.
-Dana Razzano, MD is a Chief Resident in her third year in
anatomic and clinical pathology at New York Medical College at
Westchester Medical Center and will be starting her fellowship in
Cytopathology at Yale University in 2020. She was a top 5 honoree in
ASCP’s Forty Under 40 2018 and was named to The Pathologist’s Power
List of 2018. Follow Dr. Razzano on twitter @Dr_DR_Cells.