I have been hearing many concerned questions about Monkeypox lately, and I wanted to add onto the great job already done by Dan Scungio in his previous post on how laboratorians should be safe around Monkey pox suspected samples. As a part of the queer community, I’ve heard from several people who are very concerned as this is predominately spread among men who have sex with men. I’ll be focusing on what is new about Monkeypox, how it is different, where it is spreading, and what can be done about it so far. I’ll address questions like should we be sequencing Monkeypox like COVID-19 and does your smallpox vaccination will protect you.
What is Monkey Pox?
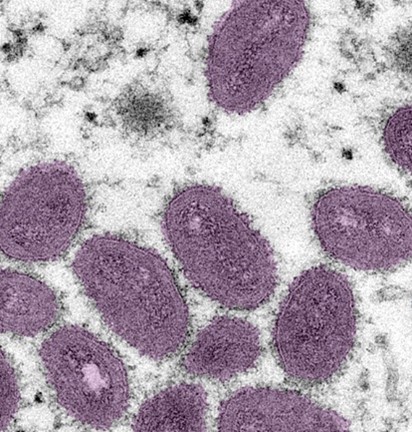
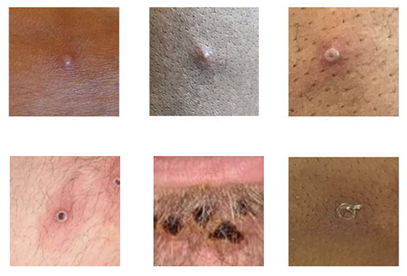
This is an orthopox virus that is from the same family as smallpox, which was so effectively cleared from human circulation that vaccines were discontinued in the U.S. in the early 1980’s. It causes a systemic disease characterized by lesions that start as a red, flat rash (macula) then form vesicles that break open, crust and resolve in 2-4 weeks. If you ever had chicken pox, you may recall how painful it was, and this is the major symptom that requires medical management.
Initially case increases were attributed to undiagnosed disease just as happened with COVID-19 initially. However, now that commercial labs are testing for it and access to testing is not an issue, we still see case counts increasing. This indicates that the rapid spread is real and concerning. That rapid spread is one reason that it has now been declared a national public health emergency.
How is it tested for?
Initially testing was sent out to one of the CDC regional testing centers. However, there were only 60-70 of these sites and they had limited capacity for high throughput testing. Then Labcorp and Quest they can each perform PCR testing, which has expanded access greatly. However they have different specimen types they accept:
Labcorp: Lesion swab in VTM sent frozen or refrigerated (room temp not acceptable)
Quest: Lesion swab in VTM
What is new?
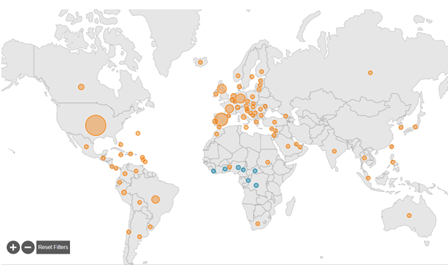
It has been in Sub-Saharan Africa for a long time.
Early summer it began to spread into other continents like Europe.
U.S. now has the highest levels of Monkeypox cases.
This all reinforces the impact of communicable diseases in a global society.
Thornhill JP, et al. Monkeypox Virus Infection in Humans across 16 Countries — April–June 2022. NEJM. July 2022. DOI: 10.1056/NEJMoa2207323
–Jeff SoRelle, MD is Assistant Instructor of Pathology at the University of Texas Southwestern Medical Center in Dallas, TX working in the Next Generation Sequencing lab. His clinical research interests include understanding how lab medicine impacts transgender healthcare and improving genetic variant interpretation.Follow him on Twitter @Jeff_SoRelle.
“The world is moving so fast, that we have few true experts on tomorrow. All we have are experts on yesterday.” –GYAN NAGPAL, The Future Ready Organization
One of my ingrained memories from my time at Harvard was the set of criteria needed to be promoted up the academic ranks within the medical school. At the “last” level—associate to full professor—one of the criteria was that you have an established international reputation and expertise in a particular area which is clearly demonstrated by your body of written work as well as the external opinions of 20+ people (in formal letters) who have never directly worked with you. Although that may sound like a tall order in words, it is something that musicians, actors, and influencers can easily demonstrate, although their “particular area” is not necessarily something tangible but certainly entertaining. In academia overall, achieving such documented prowess may appear easier for some fields than others. For example, behavioral psychology has spawned an entire industry of self-help books across every possible genre which all are based on the same principles; yet, no one really cares about the reproductive processes of Chytridiomycota. There are many people who call themselves experts in behavioral psychology and so many conventions, book signings, and meetings about the topic that those experts are probably never lonely. But our buddy who studies Chytridiomycota probably doesn’t have lunch with someone every day that includes a spicy discussion about mycelial separation. In certain areas of academia—for example, astronomy and physics—the inclusivity of publications and sharing of credit for collective work is so common that the above criterion really makes no sense but, at the same time, they are an integrated, harmonious community who all know each other and likely have raging keggers where nothing less than all of the known universe is discussed. Unfortunately, in the medical field, there are a plethora of expert cliques (Oncology, Dermatology, Surgery, Pathology, etc.) and then there are many individuals who are experts in their narrow area that the “cool kids” don’t really care about. COVID demonstrated that the cool kids do care when their house is on fire and those dejected experts are the only ones with a fire extinguisher—but I refuse to write any more about COVID. I am declaring it officially dead to me (but still staying on top of it). To quote a friend, I’ll just call it, “our recent unpleasantness.”
The take home is that expertise is excellent for society but for the individual who is burdened with a particular expertise that is uncommon (or unsavory), daily life can be lonely. Of course, there are people around that one can talk to, but they want to talk about mundane things like work, taxes, politics, Instagram, television shows, or actors. No one wants to get down and dirty into Chytridiomycota!! And we all know those folks—and love them—for their enthusiasm and their quirks. But this loneliness is much more common that we’d like to assume. When I was at Harvard, there were a cadre of people—all of different backgrounds and in different specialties—that were “global health” people. I have waxed on in previous blogs about the complex and expansive definition of “global health”, but the point is that anyone who identifies that way speaks a common enough language and has read the same books to have an engaging conversation about the topic. When I moved from Harvard to my current role at ASCP, the pool of immediate colleagues dwindled but my day-to-day job kept me in touch with so many global health people that I was even more engaged. Then the recent unpleasantness struck, and I relocated for remote working. I love my neighbors dearly but none of them have heard of global health. Moreover, because my day involves a computer terminal, innumerable meetings and emails, cross-coverage of activities, and evolving roles to meet the rapidly evolving world, the virtual global health quotient of my week has dwindled further. And sure, I could join a Facebook group or a WhatsApp thread or follow a Twitter thread about global health (and I do all of those things) but it still a little lonely most of the time.
Eureka! I was invited to give a talk—in person, ya’ll! With live people! —in Seattle in late April/early May at the behest of the Binaytara Foundation on Cancer Health Disparities. Most of the people who were invited to this summit were people I already knew but hadn’t seen in 2 years. I was happy to join but under the presumption that, “I’ve heard all this” but thought it would be great to see everyone. I was so wrong!!
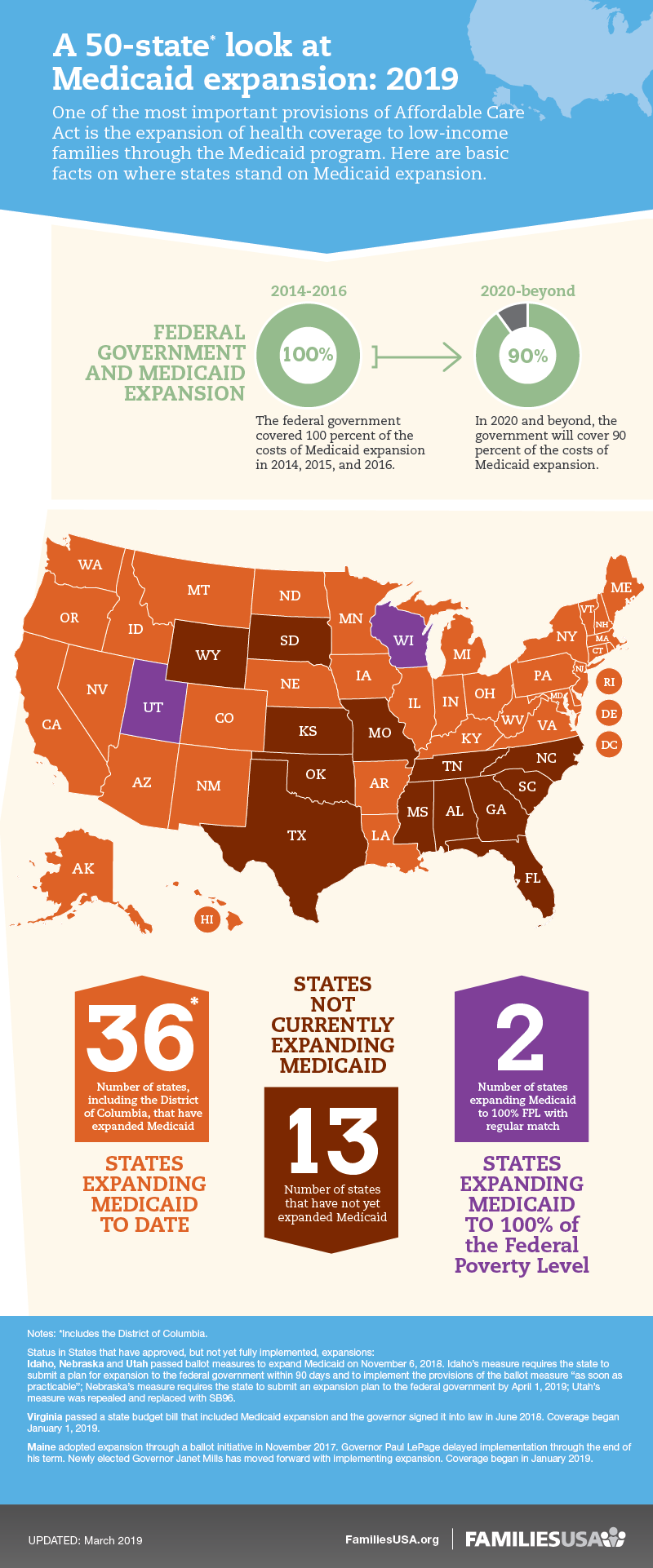
The initial session was about health insurance coverage disparities in general and for cancer, and I savored every word. Many of you will read this and likely be highly informed in this area and others may know nothing about it. For me, I’ve been busy with global health disparities (primarily in Africa) and hadn’t paid enough attention to the continued disparities in my own back yard. I was humbled, a little ashamed, but delighted to learn. There were multiple specific projects and programs, presented by the leads, demonstrating how access to insurance programs and other payment programs massively reduced and resolved disparities in particular communities—minorities, inner city, homeless, etc. There were multiple data sets demonstrating how the Affordable Care Act had drastically increased access to care and reduced self-pay (a major barrier to proper cancer care outcomes). But it was not all “rainbows and butterflies”. There was a very upsetting presentation on the Medicaid expansion for cancer coverage which was allowed by the ACA that included descriptions of early expanding, slowly expanding, and nonexpanding states. It is important to note that this Medicaid expansion was money from the federal government to states to allow them to complete this coverage for more people with cancer including screening and early diagnosis. When the ACA became law, the federal government paid 100 percent of the cost of expansion coverage (from 2014 to 2016). After that, the federal share decreased, and now it pays 90 percent (as of 2020). Although the percentage has dropped from 100 to 90, the non-expansion states did have the opportunity to opt-in when there was 100% coverage. From Barnes et al (2021), “Early Medicaid expansion was associated with reduced cancer mortality rates, especially for pancreatic cancer, a cancer with short median survival where changes in prognosis would be most visible with limited follow-up.”1 What was also demonstrated was that, where expansion occurred, many health disparities were reduced. From Han et al (2018), “Disparities in the percentage of uninsured patients by race/ethnicity, census tract-level poverty, and rurality were diminished or eliminated in Medicaid expansion states but remained high in no expansion states, highlighting the promising role of Medicaid expansion in reducing disparities among sociodemographic subpopulations.”2 Medicaid expansion was free money from the federal government so why wouldn’t states take it if it can decrease cancer mortality and eliminate obvious disparities? According to familiesusa.org, Medicaid expansion has benefitted state economies, boosted job growth, and helped working but uninsured individuals improve their health and economic situations.3 The infographic shows the expanded, expanding, and nonexpanding states. Moreover, the decrease in the uninsured rates provided by the Medicaid expansion has provided offsetting savings (less uncompensated care provided by hospitals, more tax revenue on healthcare plans, etc.) that has more than covered state costs for the expansion. I will let you draw your own conclusions about why some states wouldn’t take free money from the government to care for minority groups and the impoverished. But all of that was just a taste of the conversations. And, for some of you, perhaps it sounds like the mating habits of Chytridiomycota. But these were my people and engaging with them for 3 days was an excellent cure for the mental loneliness of the past two years.
So, what did I learn from this event—other than a lot about health insurance, training people in disparities research, LGBTQ+ health access program, etc.? Convening is a very important part of the academic and professional and human process. Convening in person with other people in the same room creates safe dialog, allows for preposterous questions and new ideas, field tests opinions, and introduces people for more collaboration. Prior to our recent unpleasantness, with my global health team at ASCP and in my global health volunteer work at Harvard, we had been using video conferencing tools for years. I was a beta tester for Zoom before it was Zoom. I had been on 5 different meetings in one day using 5 different platforms. Videoconferencing was just a tool that we had to use to talk quickly and constantly with people all over the world. But we still had coffee in the break room, weekly in person meetings, and curbsides with other staff, etc. When the switch to complete videoconferencing occurred for all day work and, along with it, the inevitable virtual conference to replace a live meeting, the loneliness of expertise grew to an almost insufferable level. The cure, however, exists and it is in the live, in person meeting.
Note: Thanks to Matthew Schultz, Jeff Jacobs, and Suzanne Ziemnik of ASCP for their insightful ideas about this topic and input on this blog post.
Barnes JM, Johnson KJ, Boakye EA, Schapira L, Akinyemiju T, Park EM, Graboyes EM, Osazuwa-Peters N. Early Medicaid Expansion and Cancer Mortality. J Natl Cancer Inst. 2021 Jul 14;113(12):1714–22. doi: 10.1093/jnci/djab135. Epub ahead of print. PMID: 34259321; PMCID: PMC8634305.
Han X, Yabroff KR, Ward E, Brawley OW, Jemal A. Comparison of Insurance Status and Diagnosis Stage Among Patients With Newly Diagnosed Cancer Before vs After Implementation of the Patient Protection and Affordable Care Act. JAMA Oncol. 2018 Dec 1;4(12):1713-1720. doi: 10.1001/jamaoncol.2018.3467. PMID: 30422152; PMCID: PMC6440711.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
The concept of disruption often has negative connotations. Everyone on the planet can understand the phrase, “COVID-19 has disrupted our lives” without explanation. Although this disruption has been global, the disruption and ensuing impact this has had on non-COVID-19 related healthcare and, specifically, oncology, have been dramatic.
Surgeries, chemotherapy and other medical treatments were canceled or delayed by months, and volumes of testing across the cancer landscape dropped to minimums. Existing infrastructure furthered the deployment of telehealth consultations and, eventually, clinics were reopened; however, there is no question that many people with cancer face being diagnosed at a more advanced stage of disease, with worse outcomes.
On 25-26 October, the World Cancer Leaders’ Summit, organized by the Union for International Cancer Control and hosted by the American Society for Clinical Pathology, brought together more than 600 leaders from some 100 countries. One of the major topics of discussion was, “What do we do for oncology after COVID-19?”
In addition to examining heart-wrenching data on disruptions to cancer services, there were also positive discussions about what we have learned from this pandemic, how we have adapted, and what novel approaches we should keep that could create optimal, more efficient, or more impactful cancer care.
The positive side of disruption
When applied to innovative technologies or ways of thinking, “disruption” can be positive, particularly when we consider the many advancements happening so quickly with treatments, including immunotherapies like check-point inhibitors, mRNA cancer vaccines, CAR-T therapy, epigenetic therapies, that the different members of the cancer community are often running to catch up.
Some of these advances are simply operational efficiency (i.e., getting more output from the system by improving the inputs and the usage) while many are transformative innovations (i.e., immunotherapy for lung cancer and melanoma). And some advances are considered “disruptive” because they are not just a new way of doing something better but allow an entirely new approach that previously wasn’t available and that radically improves prevention, diagnosis, treatment or supportive care.
A disruptive revolution in cancer detection
In oncology, a true disruptive innovation is taking place with universal cancer screening (UCS) or multi-cancer early detection (MCED). The earlier a cancer is detected and the patient can start treatment, the higher the chance of survival. The current paradigm for cancer care is suspicion of cancer leads to diagnosis, which leads to treatment. Suspicion rests in either the results of a screening test or when a person shows symptoms, and diagnosis involves a biopsy that must be analyzed.
Primary care doctors and not just oncologists will be able to use UCS and MCED testing platforms. Tests will be performed on a timescale (e.g. annually, every five years) relevant to the person’s age, medical and family history as well as the type of cancer being detected for, rather than wait for a patient to present with symptoms. Furthermore, these platforms will be able to detect 20 to 50 or more cancers from a single sample and for myriad cancer stages, including precursor or pre-invasive cancer, and there is no need for a separate diagnostics phase: the result itself would dictate a treatment because the UCS/MCED platforms not only detect the cancer but can, in theory, give an origin and medical response parameters.
Whereas the current paradigm involves primary care, oncology, surgery, radiology, pathology, nursing, etc., this new paradigm would only involve primary care and an insurance provider.
Innovating, Creating and Breaking Down Barriers
The transition from traditional oncology to such novel platforms – as with all disruptive technologies – will not be smooth as we are talking about entire businesses and careers connected to traditional oncology possibly become obsolete. People with cancer, however, are expected to have shorter, more efficient journeys, likely with better outcomes and at a lower cost.
In LMICs, where oncology care systems are not nearly as developed as in HICs and where governments, unlike the US, are generally assumed or expected to pay for cancer services, UCS/MCED will require fewer dollars and provide better results than investing in the infrastructure required to create traditional cancer care systems. If this theoretical framework (UCS/MCED for cancer) does demonstrate the value in promises, it would set the stage for similar paradigms in other non-communicable diseases for which infrastructure and resources in LMICs are often lacking.
UCS/MCED was a hot topic at the WCLS. The leaders that were involved in the meeting sit on either side of a fence with regards to this innovation. There are those that support this technology’s development as quickly as possible, anticipating better patient outcomes, more efficient systems, less healthcare spending and more revenue. There are also opponents to this innovation, who throw up barriers resulting from fear of losses (revenue, employment, testing volume, referral networks, etc.).
The barriers they present, however, are important only if they are true barriers and not just perceived barriers. Why? True barriers are likely to require the engagement of the traditional oncology system to overcome; yet the act of overcoming those barriers may herald the disruptive innovation they fear. When an existing system must participate in its own creative destruction, can such a disruptive innovation take place?
No doubt the participants of the WCLS will continue to ask this question and let’s hope they find some answers for the sake of our patients.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
On October 6th, 2021, the Lancet Commission on Diagnostics launched the “Transforming access to diagnostics” commission report with a virtual program and release of several publications. One of the publications included a study led by Dr. Sue Horton on access to diagnostics using data from 14 countries, mostly in Africa, from 2004 to 2018 with single timepoint data used to evaluate the relationship of access to diagnosis with a variety of factors. The diagnostics that were evaluated did not include histopathology, crucial for the diagnosis of cancer; however, the study did show importantly that income and population density had demonstrable relationships with access to diagnostics at the primary care level. For hospital-based access, there was no relationship which led the authors to conclude, among many other and relevant points, that access to diagnostics in “primary health care is the diagnostic so-called last mile and particularly affects poor, rural, and marginali[z]ed communities globally; appropriate access is essential for equity and social justice.” In the Commission report, the authors describe a tiered system with three levels that countries should incorporate into a national laboratory strategy and suggest that the burden of affording this system should fall on the governments. Moreover, they demonstrate the extremely important data around use of global markets to show that while the top four countries supply nearly 50% of all diagnostics, those same four countries only supply 24% of pharmaceuticals. In the opening statements to the Lancet Commission launch, Dr. John Nkengasong espoused very strongly the importance of manufacture of diagnostics WITHIN LMICs as one much needed solution.
For example, I was assisting a colleague with access to immunohistochemistry antibodies for which they were currently paying $700 USD for one vial of CD20. I traced the manufacture back to the US supplier (where the antibody was produced) and attempted to buy a vial as a private citizen with a credit card and was surprised to see that I could do so for $220 USD. This is the exact same vial of CD20 antibody. Why was my colleague paying a 218% markup? When I inquired with the company of manufacture, they reported that they had existing contracts to supply 2nd, 3rd, and 4th party vendors that they could not violate (i.e., they could not sell directly to a purchaser on the continent of Africa). The local supplier charging the $700 USD suppled a very large number and breadth of medical supplies including other diagnostic tests and reagents. Those reagents were reasonably priced, and several were on sustained government contracts. However, the CD20 antibody was not. Why is that the case? Let’s assume you are a supplier of widgets and wobbles. Your demand for widgets is huge and you sell more than 100,000 widgets per month to 20 different consumers. For wobbles, one person orders one wobble once per year. Your widgets ship room temperature but your wobbles require a cold chain, lest they be destroyed. What would you do? You could choose not to sell wobbles. You could choose to charge a ridiculous price for wobbles so that the excess time, energy, and expense of getting one wobble to your consumer is worth the effort. But you would not sell the wobbles for a similar profit margin as your widgets. It just wouldn’t make business since. Now imagine that the wobbles are manufactured in a country other than your own and to get them, you buy them from a country supplier who buys them from a regional supplier. So, wobbles already come with additional markups. You do have a third choice which is to manufacture wobbles locally, cut out the middle people, and charge much less but still make more profit. This is a great model if wobbles can be easily manufactured; however, when wobbles require an enormous capital investment, is it worth it to sell a couple of wobbles a year? Of course not. This business-based example is one of the drivers for a $700 USD vial of CD20. If a local manufacturer, in country or in a neighboring country, could manufacture and sell, this reagent would be more affordable and feasible as an available diagnostic. Specifically, patients with lymphoma would have access to rituximab for CD20.
But note the Commissions finding that almost 50% of diagnostics are made in the top 4 countries. This means, naturally, that the pricing for these reagents and supplies will be based on that economy and/or GDP, not on the economy or GDP of every country down to the lowest on any given scale. Consider the Big Mac Index, which looks at buying power relative to the US dollar. The only African country used in the Big Mac Index is South Africa and it is third from the bottom. To be clearer, if you have 100 South African Rand, you could get about $6.69 USD if you exchanged it directly (ignoring fees). If you want to buy a Big Mac in the USA, the average consumer price is $5.65; however, in South Africa, it’s 33.50 Rand. Based on the Dollar:Rand exchange rate, we are paying only $2.24 USD in South Africa for the same sandwich that would cost us $5.65 in the US. So, the Rand is undervalued. Now, let’s look at our vial of CD20 (not revealing the country to protect identities). According to the current exchange rate, you get $4.34 USD for every 10,000 units of this countries currency. Based on this model, if the CD20 was being EVENLY exchanged with cash (as opposed to being undervalued or discounted as we saw with South Africa), it should cost 450,586 units of this country’s currency. Instead, it is costing them 1,612,053 units. If we assume that this country could/should achieve a Big Mac Index equivalent discounted of the CD20 as we see with the Big Mac itself in South Africa, it should cost them 307,057 units or $133 USD. The difference? The Big Mac is manufactured and locally distributed directly to the customer in South Africa. The CD20 is not. So, one step to achieving an equitable pricing structure in healthcare for LMICs, especially in Africa, needs either direct discounted by US- and European-based manufacturers—unlikely to occur because of fear of alternative market access—or these products need to be manufactured and supplied locally.
What I have trouble agreeing with completely and, in some cases, even it part, is the concept of all healthcare costs falling on the government of a population with the expectation that they deploy a “one size fits all” approach to any aspect of healthcare. When we consider the US and Europe (again, the top four producers of diagnostics), we find one as a largely private commercial system driven by government pricing for elder care and the other a socialist system with universal healthcare enhanced by private care. For both systems, there is a huge economic base which either drives capitalism across the system from raw materials to final product or an enormous tax base that can cover the bulk of the costs of the systems. As we move from these four down the GDP ladder to LMICs, we don’t see, despite that we would like to nicely categorize countries into clear groups, a solution that would work “globally” because major pieces of economic development are needed as pre-requisites for a capitalist open market or one payer system. Each country has a unique set of circumstances (e.g., history, genetic diversity, geography, natural resources, tourism, disease burden, language, population size, etc.) that cannot be reduced to simply a GDP value or Big Mac Index factor. Moreover, it is wholly within the realm of colonialism, which we supposedly abandoned 70 to 80 years ago, to think that we can propose a system for “all countries” that would even remotely approach the solving the problems of these countries. Although it is an excellent mental exercise to idealize a healthcare system as having something as simple as three tiers and trying to allocate what tools and resources are needed at each level to accommodate the population, the reality is that such a framework is only a starting point with a lot of work needed to fully realize what type of system would be best for a given country. Very small islands and small nations may have only one hospital to serve its entire population and insufficient patients of a given type to justify the expense of certain tools. Extremely large countries with large populations will need a myriad of systems with their own tiers that support patients based on location, socioeconomic status, language, etc. and these systems likely overlap in geography. And the expertise to best determine that system is the health and government leadership of that country, not an external set of non-specific instructions. The external set of instructions, however, are extremely important, as noted, as a starting point, but each country that identifies a gap in their diagnostics, for example, has to assess their specific situation. At the heart of this problem is the need to stop talking about the challenges of global healthcare and start (or continue) directly working on fixing them.
At ASCP, we approach our global outreach through assessment, gap identification, implementation planning, and execution (AGIE). Through that approach, we have deployed and/or support 19 sites in 15 countries with telepathology; however, in an additional 10 countries, we have active programs that have not yet reached a point of telepathology deployment. Had we said, from the beginning, “We are going to give everyone telepathology”, we would have wasted an enormous amount of time and money. By following an AGIE approach, we have navigated to the specific problems of each site with whom we collaborate and attempted to solve them. And we do so with more than 80 collaborative partners. The Lancet Commissions on Diagnostics most recent launch is an excellent first alert for those who have not been engaged in global health for the last 20 years that there are still major challenges and problems in global healthcare and diagnostics. Our hope is that funders, governments, industry, health system members, patients, and advocates will view this as a rallying cry to direct resources and energy to join those of us who have been engaged in this work to move the needle even further. Access to diagnostics for every patient everywhere. It is ASCP’s simple mantra, and we hope, together, we can achieve that goal.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
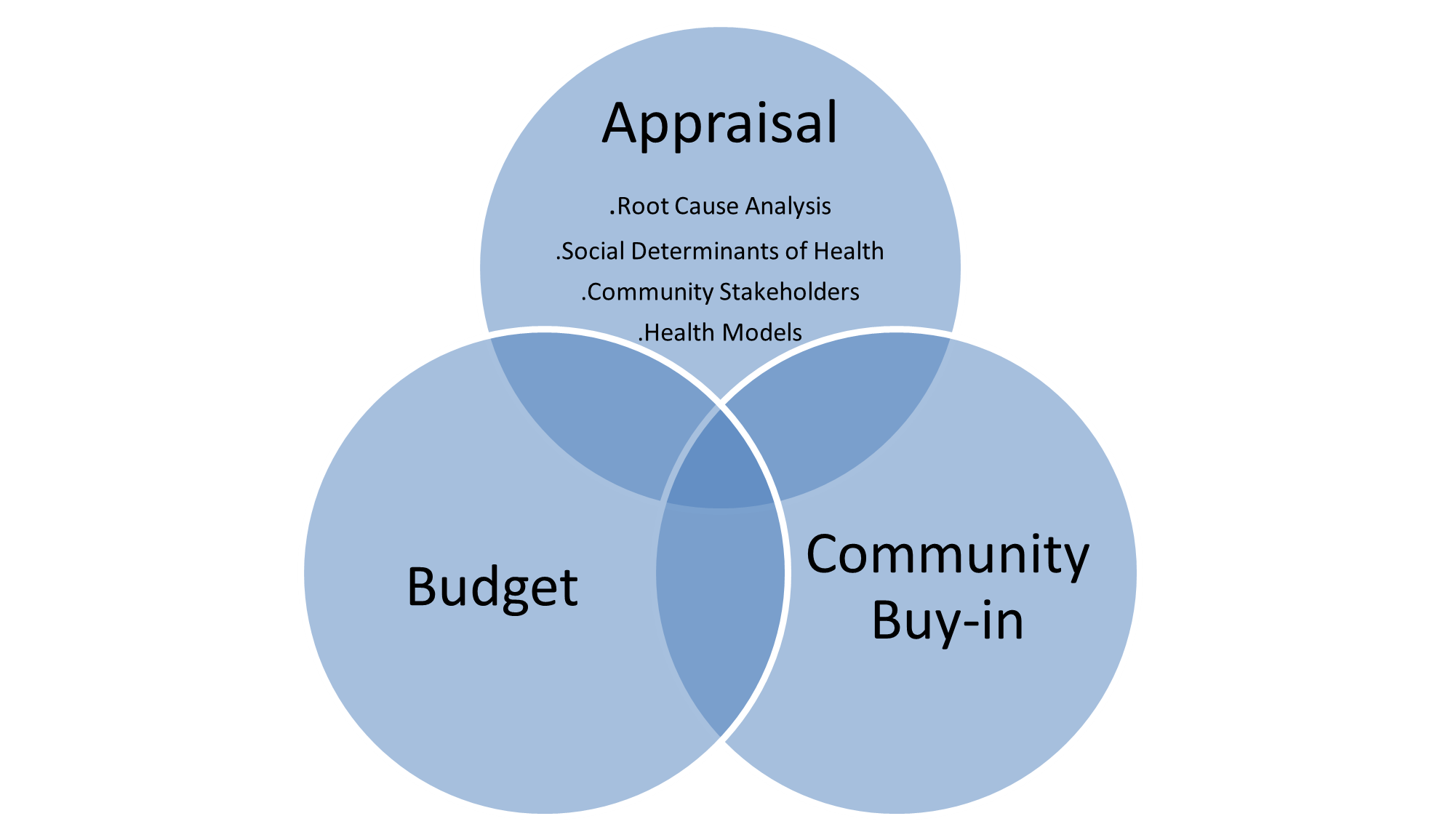
If there is anything the COVID-19 pandemic has taught us, it is the fact that the world is a global village with no country being completely immune from the effects of disease and pathogens. With migration across borders along with its attendant effects of disease dissemination, public health initiatives aimed at improving the health outcomes of populations must be designed with the target population in mind and long-term sustainability prioritized. The health of a community is dependent on the overall health of its people. Public health initiatives are often designed to modify health and disease patterns within groups of people. A key measure of success of any health initiative is its long-term sustainability. Therefore, a framework to guide program planners at the design stage of any public health program is critical to success. This framework can be summed up as the ABCs for designing sustainable public health initiatives.
Appraisal: Appraisal is defined as an act of assessing something or someone. It is an evaluation of a process, system, or population. An appraisal of any given situation or entity is carried out to give the full picture, without redundancy or superfluity. When a thorough appraisal is carried out, it elaborates the situation on the ground, and the best approaches to tackle any challenges. For an appraisal of a public health problem, the following key activities should be included in the program design.
Root Cause Analysis: A Root Cause Analysis (RCA) is a term that describes techniques and tools used to uncover the causes of a problem or failure.1 A RCA is often carried out to get to the bottom of a problem, and not to only focus on the offshoot of the problem-the observable symptom. A thorough RCA defines the problem, answers all the ‘why’ questions, and proffers solutions that lend themselves to evaluations which address the problems.
Social Determinants of health: What makes one community healthy, and the other unhealthy? What factors contribute to the well-being of communities? The social determinants of health are a consortium of factors apart from medical care that can be influenced by social policies and shape health in powerful ways.2 It is important to note that what may positively impact the health of one community, may negatively impact the health of another. Public health practitioners must be able to determine the most important influencers to health and diseases in any community, to potentiate the cost-effectiveness of any intervention. The social determinants of health can be summed up as the 3 G’s:
Geography-The physical environment and all the elements of nature. These include access to clean drinking water, healthy food portions, climate change, global warming, etc.
Goods-These includes the social and economic environment. People’s relationships, income levels, social status, education levels, etc.
Genes-These includes a person’s genetic make-up, which has been shown to have a great impact on health and certain diseases.
Therefore, a thorough analysis and understanding by public health practitioners on the most important contributor to health, and targeting resources to such areas, will increase the likelihood of success of any health intervention or campaign.
Influence of Community Stakeholders: A stakeholder’s analysis is a process of systematically gathering and analyzing qualitative information to determine whose interests should be taken into account when developing and/or implementing a policy or program.3 The stakeholders in a process are actors (persons or organizations) with a vested interest in the policy or program being implemented.3 After conducting a stakeholder analysis of the key interest groups, it is imperative to determine the influence of community stakeholders on the proposed public health initiative. Community leaders have a great influence on their constituents. Therefore, the success or ultimate failure of a project depends in part on the role of these key community actors. Vital questions must be asked and answered including but not limited to: what is their interest in the project? What is their knowledge of the project? Do they have an adequate understanding of the major root causes of the problem? Do they proffer alternate ways to address the problem? What is their voting power in the decision-making process? These are some of the key factors that may be considered when trying to determine the influence of community stakeholders on the proposed health intervention.
The Role of health models on disease causation, interpretation, and outcomes: The role of the models of health on disease incidence and survival cannot be overlooked. At the crux of any public health problem is the answer to some ‘why’ questions. It is a well-known fact that models of health including the religious, biomedical, psychosomatic, humanistic, existential and transpersonal all have a role to play in disease incidence and survival to varying degrees.4 While one model may play a more significant role in one community, the same may not be the case in another community. For example, while infections and communicable diseases are still a huge burden in many developing countries5 due to environmental and biophysical concerns including limited access to immunizations, the same is not the case in developed countries. Developed countries tend to grapple more with chronic diseases6 such as obesity, diabetes, hypertension, cancers. It is therefore the responsibility of program planners to determine during the design stages of projects, the models with greater impacts on disease causation and outcome. This approach may increase the likelihood of success than the failure of the intervention.
Budget: A budget is a financial statement detailing the income and expenditure of an entity over a given period. Proper budgeting encompasses adequate planning, both for foreseeable and unforeseeable expenditures. A budget should also include the fixed assets and in-kind or monetary contributions of the program to the execution of any public health initiative. A comprehensive budget should take into account direct and indirect costs including but not limited to personnel costs, travel costs, equipment/supplies, consultants, printing/duplication costs, postage, staff training, rent, telephone expenses, heavy machinery, etc. A project with an insufficient budget would be more likely to encounter challenges that may pose as threats to its sustainability, than one which is adequately funded. Therefore, program planners must ensure that their budgets are sufficient enough to run through the entire lifecycle of the projects.
Community buy-in: It would be an effort in futility if after going through the planning and design phases of a project, you discover that a community is not interested in that line of intervention. This would amount to a humungous waste of time and valuable resources. Therefore, program planners must ensure during the design phase of any project, to get the community’s perspective on that particular line of program approach. This is imperative because apart from getting the community’s perspective on a particular proposal, they may also be able to provide valuable pieces of information that may enhance the sustainability of any project. Community buy-in works in tandem with the role of the community’s stakeholders. Successful programs are designed for the people and with the people. In summary, at the crux of any planned public health intervention is the issue of long-term sustainability. Program planners should become familiar with addressing fundamental elements of successful program interventions. A good place to start is ensuring
Braveman P, Gottlieb L. The social determinants of health: it’s time to consider the causes of the causes. Public Health Rep. 2014;129 Suppl 2(Suppl 2):19-31. doi:10.1177/00333549141291S206
Tamm ME. Models of health and disease. Br J Med Psychol. 1993;66 ( Pt 3):213-228. doi:10.1111/j.2044-8341.1993.tb01745.x
Tadesse GA, Javed H, Thanh NLN, et al. Multi-Modal Diagnosis of Infectious Diseases in the Developing World. IEEE J Biomed Health Inform. 2020;24(7):2131-2141. doi:10.1109/JBHI.2019.2959839
Silvaggi F, Eigenmann M, Scaratti C, et al. Employment and Chronic Diseases: Suggested Actions for The Implementation of Inclusive Policies for The Participation of People with Chronic Diseases in the Labour Market. Int J Environ Res Public Health. 2020;17(3):820. Published 2020 Jan 28. doi:10.3390/ijerph17030820
-Evi Abada, MD, MS is a Resident Physician in anatomic and clinical pathology at the Wayne State University School of Medicine/Detroit Medical Center in Michigan. She earned her Masters of Science in International Health Policy and Management from Brandeis University in Massachusetts, and is a global health advocate. Dr. Abada has been appointed to serve on the ASCP’s Resident’s Council and was named one of ASCP’S 40 under Forty honorees for the year 2020. You can follow her on twitter @EviAbadaMD.
Successful healthcare systems rely on strong, efficient and reliable pathology and laboratory services. In developed countries like the United States, the role of pathology and the lab in service delivery cannot be overemphasized. Through multidisciplinary tumor board conferences, the central role of pathologists in patient management has become more critical. This reality was further emphasized for me during a tumor board conference, where an oncologist wanted clarification on the difference between invasive ductal carcinoma with mucinous differentiation vs. mucinous carcinoma of the breast. I later learned that the distinction was necessary because of different prognosis and treatment. As pathologists, we work in concert with treating physicians which makes for more efficient and reliable patient care.
However, the situation is not the same in low to middle income countries (LMIC) where the pathology and laboratory workforce is currently suboptimal. One reason that has been attributed to this situation is a lack of awareness of the central role of pathology and lab medicine in developing countries with fragile health care systems. This has led to ineffective policy decisions and inadequate budgetary allocations to the lab, with the attendant catastrophic effects on patient care and outcomes.1
West Africa for example has seen a steady decline in healthcare delivery standards, even though diseases such as Burkitt lymphoma were first described in Africa, followed by the growth of the first human lymphoma/leukemia cell line (the Raji cell line).2 In addition, ‘Cancer in Five Continents’, a publication of the International Agency on Cancer Research, used data from Ibadan-Nigeria and Uganda cancer registries in its early years of publication. Unfortunately, during the years the countries in these regions have not been able to keep up with technologic advances that have since reshaped healthcare service delivery and research.3 Several barriers to sustainable pathology and laboratory services in LMIC have been identified including an inadequate workforce, substandard infrastructure, inadequate education and training, and quality assurance problems.1
Despite these challenges, there are opportunities to improve healthcare delivery systems in LMIC through effective laboratory and pathology services. One area that needs to be prioritized is the education and training of qualified pathology and laboratory personnel. This can be achieved through cross-cultural competency training and the building of collaborative networks through short term visitor exchange programs. In addition, continuing medical education (CME) opportunities should be made available to training institutions in these countries so they can keep up with modern day standards.
Another opportunity for growth in pathology and lab services in LMIC is through the implementation of accreditation and regulatory programs. These accreditation services should set standards by which lab services operate in these countries to ensure reliable and consistent operations. Such efforts may improve health service deliveries and ultimately improve patient outcomes.
One factor that has been a huge problem in disease prevention in LMIC is lack of adequate screening programs for chronic diseases, including several cancers. In many countries, misplaced priorities, in addition to lack of adequate personnel has been the bane of the healthcare systems. Therefore, policies that promote screening programs in LMIC should be prioritized. This strategy if implemented properly could lead to significant improvements in the healthcare systems, which would ultimately have an impact on patient care.
Furthermore, collaborative healthcare should be prioritized. The care and management of patients should be done collaboratively through clinicians across different specialties with proper communication channels in place. There have been instances where a clinician treating a patient may not have access to laboratory results requested by another clinician, which ultimately impacts the outcome of patients.
The role of efficient and functional laboratory and pathology services in healthcare systems cannot be overemphasized. Systems which lack these services experience catastrophic patient outcomes and until local and international governments prioritize the labs in these low-resource settings, patient outcomes will continue to remain suboptimal.
References
Sayed S, Cherniak W, Lawler M, Tan SY, El Sadr W, Wolf N, Silkensen S, Brand N, Looi LM, Pai SA, Wilson ML, Milner D, Flanigan J, Fleming KA. Improving pathology and laboratory medicine in low-income and middle-income countries: roadmap to solutions. Lancet. 2018 May 12;391(10133):1939-1952. doi: 10.1016/S0140-6736(18)30459-8. Epub 2018 Mar 15. PMID: 29550027.
Pulvertaft JV. Cytology of Burkitt’s Tumour (African Lymphoma). Lancet. 1964 Feb 1;1(7327):238-40. doi: 10.1016/s0140-6736(64)92345-1. PMID: 14086209.
Adeyi OA. Pathology services in developing countries-the West African experience. Arch Pathol Lab Med. 2011 Feb;135(2):183-6. doi: 10.1043/2008-0432-CCR.1. PMID: 21284434.
-Evi Abada, MD, MS is a Resident Physician in anatomic and clinical pathology at the Wayne State University School of Medicine/Detroit Medical Center in Michigan. She earned her Masters of Science in International Health Policy and Management from Brandeis University in Massachusetts, and is a global health advocate. Dr. Abada has been appointed to serve on the ASCP’s Resident’s Council and was named one of ASCP’S 40 under Forty honorees for the year 2020. You can follow her on twitter @EviAbadaMD.
In this last part of our four-part series on pathology value chain, where we are using the patient’s best outcome as the maximized value, we examine two areas: Marketing/Sales and Service. The former has inherent challenges, some of which were mentioned in the last blog on outbound logistics. The latter is becoming an increasingly important component of oncology care for which many pathology labs are grasping for solutions.
In traditional business budgeting, the first step is for the marketing and sales department of a firm to provide a projection of revenue for a given period based on their knowledge of trends, markets, prior years, competition, competitive advantage, etc. These projections are then paired with costing exercises to shoot for a margin of profit. If we are going to sell $1,000,000 in widgets and it costs us $750,000 in total to make those widgets available to our customers (including costs of goods sold, administrative expense, taxes, and interest), we would have a $250,000 profit to use as retained equity or to distribute to our shareholders. When we look at pathology services for cancer, a new laboratory with no prior history may find this process extremely challenging without an enormous amount of data. An existing laboratory with many years of work may have a much easier time and, short of drastic changes in supply prices, inflation, and taxes, could likely use a simple percentage growth approach for this calculation.
But unlike widgets or iPhones or Quarter Pounders or golf clubs, no one wants to have a tissue biopsy and certainly no one wants to have suspected cancer. If we turn to epidemiological data, we can predict (and do so below) the expected number of patients in a given population to likely have cancer in the coming year (although this is clearly not the only data point we need). For a new laboratory in a place where there are no other laboratories (e.g., a small low- to middle-income country with a new Ministry of Health mandate to fight cancer), such an estimate is important for determining both if we should even have a lab (or use a regional approach) and, if we do have a lab, what our maximum volume would be assuming 100% access. The former part has been addressed previously such that there is a threshold below which is difficult to justify a lab because of the cost per sample. The latter part, however, is crucial because a “marketing campaign” (i.e., patient education and clinician education about cancer, how to diagnosis it, and how labs are part of this process) is the only way to have any volume in this laboratory.
We would except it to start slow and build but we have a finite endpoint for cancer cases in mind. But note, importantly, that the marketing campaign described has nothing to do with the pathology laboratory itself. In an existing, highly-developed market (e.g., Boston, London, Montreal, Sydney), there is a population that we can assume represents our cancer risk pool but there are also many competing laboratories (and health systems), transient use of services (e.g., Ms. Smith from Iowa decides to go to Boston for cancer care), and levels of care (i.e., low-stage cancer care in a community setting versus later-stage cancer with comorbidities in a tertiary care setting). None of these things can a given pathology laboratory control if they are in that market, but must they use all of this information to understand the projected revenue and create their budget? Or can they just assume a percentage increase? From the patient perspective, all of this is irrelevant because patients most commonly do not choose the pathology laboratory that is going to see their biopsy as it is a function of the health system to which they subscribe for their care. In that context, marketing and sales for cancer diagnostic services is largely a negotiation between laboratories and clients (e.g., clinicians, hospitals, health plans) which is often contractual. Such contracts are difficult to negotiate, take a long time, and usually last for an extended period like 1 year or longer. This very concept is contrary to the activities of the marketing and sales department which must constantly pivot, update, and change their strategy to achieve their projected revenue. It is worth noting that in many poorly developed cancer systems, patients do directly take their samples to pathology laboratories of their choice and examples of systems with kick backs to shift these samples away from government laboratories toward private practice facilities (at a much higher cost to patients) are well documented.
In the Value Chain model, service is the after-market activities of a firm to maintain their product(s) for a customer, create customer loyalty and resales, and enhance their competitive advantage through maximized firm-customer relationships. The popularity of subscription services (e.g., Amazon Prime, Netflix, Massage Envy, car leasing) stems from the increased opportunity to interact with customers continuously in low-cost ways that enhance the customer’s experience with the firm. Although a service like rending a definitive pathological diagnosis may appear to be a one-time event, recent evolution in the practice of oncology and increasing research needs have created unique servicing opportunities for pathology laboratories. The emergence of biomarkers that dictate treatment unrelated to the diagnostic process has created gaps in quality due to inefficient systems, entry cost barriers, volume challenges, and intellectual disconnect from the traditional diagnostic process. However, streamlining the biomarker process, for example, can create a competitive advantage for a laboratory and improve client loyalty and rapport.
Marketing and Sales
This activity focuses on “strategies to enhance visibility and target appropriate customers.” This activity in diagnostic anatomic pathology specifically for cancer speaks to the first part of the value chain for the patient; namely, the timely presentation of a patient to the clinical system for evaluation of cancer at the earliest possible time. As such, whether a patient presents incredibly early or very late makes no difference to the pathology laboratory because the customer choosing the pathology service is either an independent clinician or a health system. Private practice pathologists may advertise or market to community hospitals or hospital systems in hopes of capturing their volume (and revenue). Marketing for second opinion review by a pathologist can also occur and may be directly to patients. This activity is challenged from the beginning, however, due to the small market. For every 1,000,000 patients in the United States, there are about 5500 cancers per year. Assuming the accuracy of a clinical decision to obtain a biopsy is around 50% (i.e., the “malignancy rate” – when a clinician decides a biopsy is needed for suspected tumor, 50% of the time it is cancer and 50% of the time it is not), that’s 11,000 suspected cancer biopsies per million per year. Extrapolating to the US population, we get 3.6 million biopsies per year. Given that there are ~10,000 anatomic pathologists, that equates to, on average, 361 biopsies per year per pathologist (or, roughly 1 per day). Since most pathologists could easily sign out 20 cases every other day working Monday – Friday with 4 weeks of vacation annually, that’s a ratio of 1:8 (average:capacity).
The point of all of this math is that the volume of pathology work in the US that is for cancer is small relative to the total biopsies performed (or capable of being performed) by the pathology community and, thus, the market for cancer diagnostic services appears saturated. We can adjust the dial of this to take the malignancy rate to 5% (i.e., massive over biopsy setting), and find that pathology would be overwhelmed at 130% capacity just for suspected cancers; however, as we move back towards 50% malignancy rate, the average capacity is around 25% for volume. If we move on the other side of 50% towards lower biopsy rates or “improved clinical acumen,” capacity quickly drops to below 9% with a great excess of pathologists. With the promise of artificial intelligence to assist pathologists in faster sign out of higher volumes, the capacity for cancer diagnosis increases possibly 10-fold. But if you ask your average pathologist if they are busy, they report that they are. This is because the pathology laboratory, as all laboratorians are aware, processes more than just suspected cancer biopsies. Medical kidney, medical dermatology, screening colonoscopy, colposcopy, breast core needles, melanotic and non-melanotic skin lesions create a huge portion of the volume that is not part of the specific calculation above that adds many millions more samples per year to the pathology revenue stream. One framing of this case pool is that cancer biopsies, because they aren’t technically elective, are cross subsidized by providing all of the other services which are equally billable. However, this large bulk of cases are still not through direct marketing to the patient but rather to providers or health systems.
As we turn this activity towards LMICs, we instantly have a problem. There is no system in most places to support routine services for medical kidney, medical dermatology, screening colonoscopy, colposcopy, breast core needles, melanotic and non-melanotic skin lesions (especially in Black patient populations for the last). Without the cross-subsidization that these billable biopsies bring in, pathology laboratories are left with the low volumes of suspected cancer cases. As mentioned above, these laboratories are often overwhelmed to begin with so the marketing and sales activity, which would theoretically increase volume, is likely not to be a priority. In these settings, however, what will increase volume and improve the quality of care for patients is large pre-analytical efforts by governments and other entities to educate the public and the general practitioner about cancer screening and diagnosis, community awareness about cancer care systems, specimen transport networks from the most rural directly to pathology laboratories, and government spending on prevention of cancer.
Service
This last set of activities are to “maintain products and enhance consumer experience.” For a diagnosis of cancer, once rendered, there are many potential touch points with both the patient and the treating clinician that can enhance the outcomes for the patient. These include maintenance of tissue in repositories for future studies, performance of future studies related to newly available treatments, access to clinical trials, and, as mentioned in the outgoing logistics, increased, and enhanced communications around the diagnosis and subsequent information. In LMICs, there is a great desire to provide such enhancements especially in settings where these activities can facilitate local research and generate much-needed local clinical trials with pharmaceutical and other industry partners. As the other steps of the value chain are improved, the continue service will come into focus and can include such activities as external quality assurance, laboratory accreditation, personnel certification, documented compliance with standards, awards, and other accolades.
To conclude, from the patient framework, the maximum value for a patient with cancer involves the earliest possible detection of the tumor and a rapid, accurate diagnostic report matched to treatment options that lead to survivorship. For a pathology laboratory, the best outcomes for patients and the best revenue model for the laboratory results from a high-volume of small samples (i.e., biopsies) reported with complete clarity. Cross subsidization of cancer diagnostic services (especially those for later staged, complex cancer patients) with other non-cancer, pathology-based reporting is crucial to create a sustainable revenue stream and ensure highest quality outcomes. Competitive advantage in pathology services specific to cancer are currently and will continued to be largely tied to the after diagnostic service and support to keep the patient on the most beneficial cancer journey.
References
Porter, M. (1985). The value chain and competitive advantage, Chapter 2 in Competitive Advantage: Creating and Sustaining Superior Performance. Free Press, New York, 33-61.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
Globally, colorectal cancer (CRC) is the third most common cancer in men and the second in women.1 It is the fourth main cause of cancer death in the world, with nearly 1.8 million new cases and 881,000 deaths in 2018.2 As alarming as these numbers, some progress has been made in terms of disease occurrence and outcome in many developed countries through the design and implementation of effective screening programs. With better access to healthcare services and overall improvements in treatment of CRC, patients in developed countries can have their pre-malignant, in-situ and minimally invasive polyps detected and removed in time through effective colonoscopy screens and disease interpretation by pathologists. Unfortunately, this progress is not uniform across the globe. Many developing countries across Latin America, Africa and Asia are experiencing increases in their CRC cases.3-5 A number of factors are responsible for this disparate reality.
With limited healthcare resources, many developing countries still struggle with efficient and effective health services. Several studies have shown the significant role of effective screening programs in detecting early colorectal adenomas. However, channeling scarce resources to support preventative health services is still a luxury many of these countries cannot afford. In addition, making sure these services actually work, would require effective laboratory services, laboratory professionals and pathologists. Unfortunately, due to limited resources and ambiguous priorities, laboratory services in some areas are not equipped to prioritize preventive health services, with direct impacts on CRC incidence and survival.
Image 1. Hematoxylin and Eosin-stained composite image of Medullary Colon Cancer. Left side (4x magnification) shows colonic mucosa with a well-demarcated solid nest of tumor cells with conspicuous lymphoplasmacytic infiltrates. Right side (20x magnification) shows a higher magnification of the pleomorphic tumor cells with irregular nuclear membranes, vesicular chromatin, prominent nucleoli and multiple mitotic figures. Medullary colon cancers are usually right-sided and have a better prognosis compared with poorly-differentiated or undifferentiated adenocarcinoma of the colon.6
Even though the majority of CRC occur through somatic events, some however, do progress through well-defined germline mutations including inherited cancer syndromes including Lynch syndrome (Hereditary Non-Polyposis colon cancer/HNPCC), Peutz-Jeghers syndrome and the Familial Adenomatous Polyposis (APC mutations) pathway. Unfortunately, cancer genetics and molecular diagnostics is still not mainstream in healthcare institutions in many developing countries. Therefore, patients and their families with affected mutations may find it extremely difficult getting access to the care they need in terms of diagnosis and treatment.
The rising incidence of CRC in developing countries may also be explained by the rising trends in Westernized practices which leads to several modifiable risk factors including the consumption of diets rich in saturated fats, lack of physical activity, diabetes, obesity, alcohol consumption and smoking. Preventive health services through effective public health education on the dangers and risks of these environmental practices may play a role in disease prevention and outcomes.
At the crux of CRC prevention and early detection is effective screening programs. As March marks colorectal cancer awareness month, it is imperative to emphasize that any sustainable health policy program must consider the unique role that effective pathology and laboratory services has to play. We must be invited to stakeholder discussions as the value we bring to such discussions cannot be overstated. A failure to recognize our position as central to improving patient outcomes has made many healthcare systems less effective in addressing public health challenges.
Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424.
Bosetti C, Malvezzi M, Chatenoud L, et al. Trends in colorectal cancer mortality in Japan, 1970‐2000. Int J Cancer 2005;113:339–41.
Center MM, Jemal A, Ward E. International trends in colorectal cancer incidence rates. Cancer Epidemiol Biomarkers Prev 2009;18:1688–94.
Souza DL, Jerez‐Roig J, Cabral FJ, et al. Colorectal cancer mortality in Brazil: predictions until the year 2025 and cancer control implications. Dis Colon Rectum 2014;57:1082–9.
Cunningham J, Kantekure K, Saif MW. Medullary carcinoma of the colon: a case series and review of the literature. In Vivo. 2014;28(3):311-314.
-Evi Abada, MD, MS is a Resident Physician in anatomic and clinical pathology at the Wayne State University School of Medicine/Detroit Medical Center in Michigan. She earned her Masters of Science in International Health Policy and Management from Brandeis University in Massachusetts, and is a global health advocate. Dr. Abada has been appointed to serve on the ASCP’s Resident’s Council and was named one of ASCP’S 40 under Forty honorees for the year 2020. You can follow her on twitter @EviAbadaMD.
In the first two installments of this blog series, we looked at inbound logistics and operations in which we can conclude that competitive advantage may be challenging to achieve. Now we turn to outbound logistics or, in simplest terms, the pathology report.
No document can be more terrifying for a patient than a pending pathology report from a biopsy, as it may contain a benign diagnosis, a malignant diagnosis, or something entirely unexpected. These reports are so important that unsuspected (non-malignant) and malignant diagnoses are included as “critical values” requiring a call and documentation to the clinical team as soon as they are discovered. Pathology reports in HIC are often not immediately available to the patient (unlike other laboratory tests) because the reports are often complex, may contain confusing terms, and may use language that patients inappropriately react to without the guidance of their clinician for meaning in their care. For example, cytology reports may be highly informative to a clinician by simply stating, “No evidence of malignancy” but may be stressful to a patient without guidance because there is not a definitive answer to what a lesion was. Similarly, a colon resection that states, “Invasive adenocarcinoma confined to the mucosa” is good news to the clinician but the first two words (and the internet) may be disturbing for the patient. The important point here is that pathology reports are written for clinicians and not written for patients as an audience. To that end, pathology reports should be highly aligned with the clinical decision-making process, an approach which is naturally aided by standardize or synoptic reporting of cancers using guidelines such as those of the College of American Pathologists, the Royal Colleges of the UK and Australia, and/or the International Collaboration on Cancer Reporting (a consortium of CAP, RCUK, RCA, ASCP, and others). These templates for a given cancer are complex, not easily committed to memory, nuanced, and require a high degree of pathology knowledge to apply correctly from the gross to the final histology findings. Thus, the value in these templates is in use by a pathologist directly, making task-shifting in this area nearly impossible without the aid of tools such as whole slide imaging and artificial intelligence (which still require a pathologist to finalize the report). Like operations, we see that a “standard of care” or a “standardized approach” to reporting cancer reduces the variability or uniqueness that can be achieved with a pathology report, infringing on competitive advantage.
Outbound Logistics – This activity covers the distribution of the final product to the consumer. For the maximum value to the patient, a report should be organized to match the treatment plan, available immediately upon completion, and provide an unambiguous answer than can be acted on. Although the first two activities generate the most important information for the patient and do so with “standards of care”, this activity involves communicating the results to the clinical team members who will act on it and, therefore, can open opportunities for competitive advantage. A new diagnosis of cancer is considered a “critical value” and requires a communication with documentation to the clinical team. However, much of pathology’s role in cancer care includes work with existing cancer patients so rapid communication of any result (not just the first cancer diagnosis) can add value. For example, integration of the pathology laboratory information system into the electronic medical record creates immediate results to clinicians. Alert systems including text messages, instant messages, emails, faxes, etc. add value by informing the busy clinician that the result is there. Photographs of the tumor grossly, histologically, or the results of specials studies can be included in printed or digital reports. Pathologists can attend tumor boards or other in-person or virtual meetings to present the results and explain them if there are questions. The more information that is transmitted with clarity to clinicians, the higher value the patient will obtain. The challenge in this activity is that the payment for the laboratory services ends with the diagnostic report and appropriate coding and, thus, laboratories may have to upcharge for their services to add these features. These further communications, which we can see adds value to the patient, does not add value to the laboratory’s revenue model without upcharges. In fact, it likely costs more to have such active communications as it takes pathologists away from the higher volumes which do equate to higher revenue (as we saw in operations). Streamlining these types of communications with electronic systems is key in cost and time savings and is the basis for the laws and regulations, for example, in the USA which require electronic medical records including laboratories. However, as laws, regulations, and guidelines evolved, these electronic communications are becoming standard of care requiring the entire system to increase the costs to have them but eroding the competitive advantage of providing such concierge services. Consider the change COVID-19 has had on communications between patients, clinicians, and the laboratory where a multi-person discussion of a case with images and consensus opinions can be done in a few minutes over a video conference without anyone leaving their office. Has this crisis provided a new way to capture time (and therefore revenue) but still provide concierge services? Or has it (more likely) created a new normal that everyone has to adopt (eroding competitive advantage)?
When we turn to LMICs and observe the activities of the pathology laboratory, communication with clinical teams on the front or back end has been uncommon and traditionally not done. Oncological practices in HIC are filtering down to LMICs including tumor boards, frozen sections (i.e., rapid, in surgery diagnostics), etc. and being instituted with some frequency. These activities improve patient value and outcomes, educate the teams in both directions, and are clearly beneficial to the system. But they take time and effort away from already understaffed systems which detracts from the value of other patients ultimately. However, when we observe these systems, we often find that they lack electronic tools for running the laboratory internally which inhibits tools for reporting externally. Thus, the major needed solution now is that any histology laboratory anywhere in the world should be using an anatomic pathology laboratory information system as it creates internal and external tools for standardized reporting, communication, and management. Furthermore, it creates better opportunities to integrate synoptic (templated) reporting, interdisciplinary team activities, and standardization of requisitions (i.e., upon receipt of samples). Greatly increased value for patients in LMICs can be achieved with electronic APLIS.
Lastly, there are incredible examples of pathologists who make time in their day to meet with patients to discuss their pathology reports. These discussions can only focus on what the reports says and what the words in the report mean, as defined not in context of that patient. Such exchanges can provide patients with helpful questions to ask their clinicians and prepare them to better understand what the clinicians suggests as next steps for treatment. Clearly valuable to the patient, these exchanges are also valued by the pathologists who enjoy the face-to-face interactions with patients that humanize the process. In rare cases (possibly a for-profit situation), these services may generate revenue but under current medical billing rules there is no standard mechanism for the pathologist to be reimbursed. If we have identified this as adding value to the patient in the pathology value chain, should we not try to find ways to build these services into the care model financially? With the ubiquitous use of video conferencing in the COVID-19 era, can this task be of minimal effort to pathologists but still add value for patients?
In our last installment, we will discuss marketing & sales and service, both of which are particularly flawed and fascinating to consider.
References
Porter, M. (1985). The value chain and competitive advantage, Chapter 2 in Competitive Advantage: Creating and Sustaining Superior Performance. Free Press, New York, 33-61.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
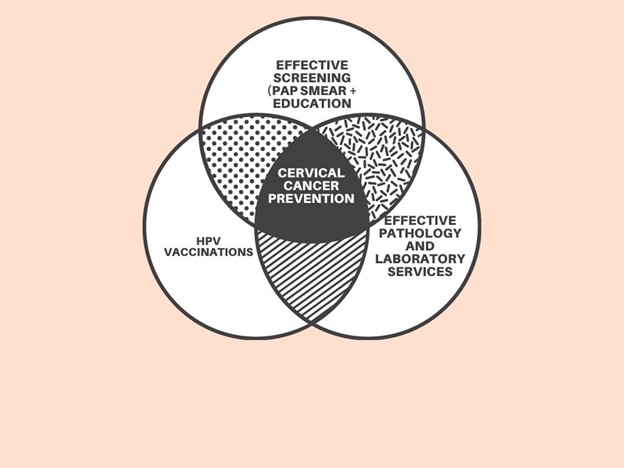
One of the most effective public health strategies to date is the development of the pap smear test and its use as a screening tool in cervical cancer prevention. Before the emergence of the pap test, cervical cancer used to be the leading cause of cancer-related deaths for women in the United States.1 However, with effective pap tests screening programs and the availability of the HPV vaccine against high-risk serotypes known to be a major cause of cervical cancer, many developed countries have been able to address this disease with its attendant catastrophic consequences including loss of lives, income and long-term disabilities.
Now, cervical cancer doesn’t even make it as one of the top 10 causes of cancer-related deaths for women in the United States.2 Unfortunately, the progress that has been made with this disease is not a universal one. While many developed countries have made giant strides in addressing this disease burden, most developing countries still grapple with significant morbidities and mortalities attributable to cervical cancer. Recent statistics show that cervical cancer is the second most commonly diagnosed cancer after breast cancer and the third leading cause of cancer death after breast and lung cancers in developing countries.3 In fact, almost 90% of cervical deaths in the world occur in developing countries, with India alone accounting for 25% of the total cases.3 Cervical cancer incidence and mortality rates are highest in sub-Saharan Africa, Central and South America, South-eastern Asia, and Central and Eastern Europe.3 A combination of factors may be responsible for these discrepant findings in developing countries.
First is the lack of effective screening programs that detect precancerous lesions before they become invasive diseases. Unfortunately, this factor is linked to lack of awareness through education and sub-optimal laboratory services that still exists in many of these countries. Laboratory services are scarce and there has been a gradual decline in laboratory professionals. Even if the supplies and equipment needed to run a lab were available, where are the laboratory professionals and pathologists that are needed to provide this critical healthcare service? In addition, a lack of regulatory oversight in some of these countries makes the replication and standardization of results increasingly challenging.
Secondly, is the role of HPV vaccinations in preventing cervical cancer. Many of these developing countries are yet to incorporate routine HPV vaccinations into their vaccination programs and access to these services are still very low. In contrast, many developed countries have made HPV vaccinations available and accessible, which is a major defense against cervical cancer.
Thirdly, is the impact of government policies on laboratory medicine. Pathology and laboratory medicine continue to face cuts in services and compensations, even in developed countries including the United States. These practices impact the ability of laboratory services to deliver optimal results, a scenario that could be even more problematic in developing nations.
As January marks cervical cancer awareness month, public health and policy professionals need to take steps to address the root causes of this problem, in order to proffer sustainable solutions, especially in developing countries. In addition to prioritizing health education and public health campaigns on cervical cancer prevention, the role of effective laboratory services in addressing these challenges also need to be emphasized.
A successful healthcare initiative requires a strong and functioning laboratory system, especially in the 21st century. Any health policy program or public health campaign that fails to recognize this fact is most likely headed for failure before it even starts off.
Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer. Available from: http://globocan.iarc.fr, 2013.
-Evi Abada, MD, MS is a Resident Physician in anatomic and clinical pathology at the Wayne State University School of Medicine/Detroit Medical Center in Michigan. She earned her Masters of Science in International Health Policy and Management from Brandeis University in Massachusetts, and is a global health advocate. Dr. Abada has been appointed to serve on the ASCP’s Resident’s Council and was named one of ASCP’S 40 under Forty honorees for the year 2020. You can follow her on twitter @EviAbadaMD.