“The world is moving so fast, that we have few true experts on tomorrow. All we have are experts on yesterday.” –GYAN NAGPAL, The Future Ready Organization
One of my ingrained memories from my time at Harvard was the set of criteria needed to be promoted up the academic ranks within the medical school. At the “last” level—associate to full professor—one of the criteria was that you have an established international reputation and expertise in a particular area which is clearly demonstrated by your body of written work as well as the external opinions of 20+ people (in formal letters) who have never directly worked with you. Although that may sound like a tall order in words, it is something that musicians, actors, and influencers can easily demonstrate, although their “particular area” is not necessarily something tangible but certainly entertaining. In academia overall, achieving such documented prowess may appear easier for some fields than others. For example, behavioral psychology has spawned an entire industry of self-help books across every possible genre which all are based on the same principles; yet, no one really cares about the reproductive processes of Chytridiomycota. There are many people who call themselves experts in behavioral psychology and so many conventions, book signings, and meetings about the topic that those experts are probably never lonely. But our buddy who studies Chytridiomycota probably doesn’t have lunch with someone every day that includes a spicy discussion about mycelial separation. In certain areas of academia—for example, astronomy and physics—the inclusivity of publications and sharing of credit for collective work is so common that the above criterion really makes no sense but, at the same time, they are an integrated, harmonious community who all know each other and likely have raging keggers where nothing less than all of the known universe is discussed. Unfortunately, in the medical field, there are a plethora of expert cliques (Oncology, Dermatology, Surgery, Pathology, etc.) and then there are many individuals who are experts in their narrow area that the “cool kids” don’t really care about. COVID demonstrated that the cool kids do care when their house is on fire and those dejected experts are the only ones with a fire extinguisher—but I refuse to write any more about COVID. I am declaring it officially dead to me (but still staying on top of it). To quote a friend, I’ll just call it, “our recent unpleasantness.”
The take home is that expertise is excellent for society but for the individual who is burdened with a particular expertise that is uncommon (or unsavory), daily life can be lonely. Of course, there are people around that one can talk to, but they want to talk about mundane things like work, taxes, politics, Instagram, television shows, or actors. No one wants to get down and dirty into Chytridiomycota!! And we all know those folks—and love them—for their enthusiasm and their quirks. But this loneliness is much more common that we’d like to assume. When I was at Harvard, there were a cadre of people—all of different backgrounds and in different specialties—that were “global health” people. I have waxed on in previous blogs about the complex and expansive definition of “global health”, but the point is that anyone who identifies that way speaks a common enough language and has read the same books to have an engaging conversation about the topic. When I moved from Harvard to my current role at ASCP, the pool of immediate colleagues dwindled but my day-to-day job kept me in touch with so many global health people that I was even more engaged. Then the recent unpleasantness struck, and I relocated for remote working. I love my neighbors dearly but none of them have heard of global health. Moreover, because my day involves a computer terminal, innumerable meetings and emails, cross-coverage of activities, and evolving roles to meet the rapidly evolving world, the virtual global health quotient of my week has dwindled further. And sure, I could join a Facebook group or a WhatsApp thread or follow a Twitter thread about global health (and I do all of those things) but it still a little lonely most of the time.
Eureka! I was invited to give a talk—in person, ya’ll! With live people! —in Seattle in late April/early May at the behest of the Binaytara Foundation on Cancer Health Disparities. Most of the people who were invited to this summit were people I already knew but hadn’t seen in 2 years. I was happy to join but under the presumption that, “I’ve heard all this” but thought it would be great to see everyone. I was so wrong!!
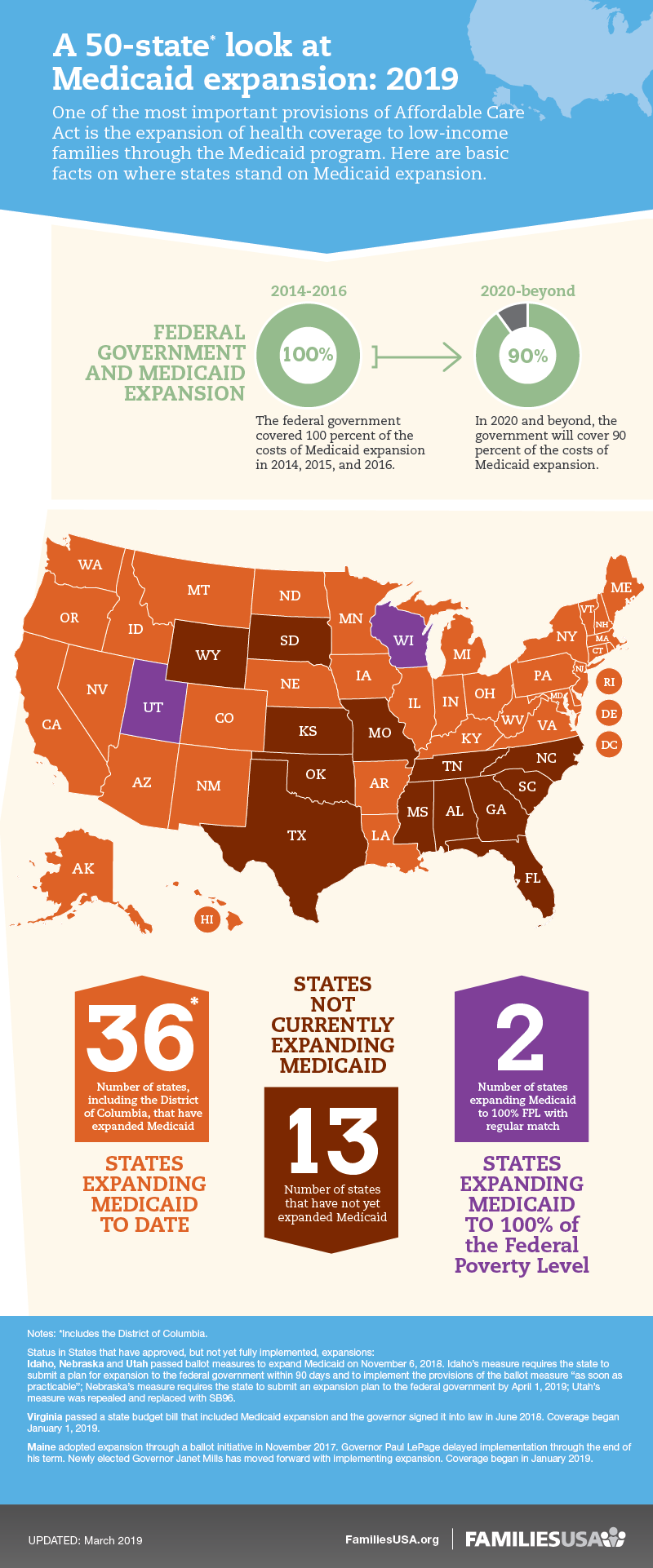
The initial session was about health insurance coverage disparities in general and for cancer, and I savored every word. Many of you will read this and likely be highly informed in this area and others may know nothing about it. For me, I’ve been busy with global health disparities (primarily in Africa) and hadn’t paid enough attention to the continued disparities in my own back yard. I was humbled, a little ashamed, but delighted to learn. There were multiple specific projects and programs, presented by the leads, demonstrating how access to insurance programs and other payment programs massively reduced and resolved disparities in particular communities—minorities, inner city, homeless, etc. There were multiple data sets demonstrating how the Affordable Care Act had drastically increased access to care and reduced self-pay (a major barrier to proper cancer care outcomes). But it was not all “rainbows and butterflies”. There was a very upsetting presentation on the Medicaid expansion for cancer coverage which was allowed by the ACA that included descriptions of early expanding, slowly expanding, and nonexpanding states. It is important to note that this Medicaid expansion was money from the federal government to states to allow them to complete this coverage for more people with cancer including screening and early diagnosis. When the ACA became law, the federal government paid 100 percent of the cost of expansion coverage (from 2014 to 2016). After that, the federal share decreased, and now it pays 90 percent (as of 2020). Although the percentage has dropped from 100 to 90, the non-expansion states did have the opportunity to opt-in when there was 100% coverage. From Barnes et al (2021), “Early Medicaid expansion was associated with reduced cancer mortality rates, especially for pancreatic cancer, a cancer with short median survival where changes in prognosis would be most visible with limited follow-up.”1 What was also demonstrated was that, where expansion occurred, many health disparities were reduced. From Han et al (2018), “Disparities in the percentage of uninsured patients by race/ethnicity, census tract-level poverty, and rurality were diminished or eliminated in Medicaid expansion states but remained high in no expansion states, highlighting the promising role of Medicaid expansion in reducing disparities among sociodemographic subpopulations.”2 Medicaid expansion was free money from the federal government so why wouldn’t states take it if it can decrease cancer mortality and eliminate obvious disparities? According to familiesusa.org, Medicaid expansion has benefitted state economies, boosted job growth, and helped working but uninsured individuals improve their health and economic situations.3 The infographic shows the expanded, expanding, and nonexpanding states. Moreover, the decrease in the uninsured rates provided by the Medicaid expansion has provided offsetting savings (less uncompensated care provided by hospitals, more tax revenue on healthcare plans, etc.) that has more than covered state costs for the expansion. I will let you draw your own conclusions about why some states wouldn’t take free money from the government to care for minority groups and the impoverished. But all of that was just a taste of the conversations. And, for some of you, perhaps it sounds like the mating habits of Chytridiomycota. But these were my people and engaging with them for 3 days was an excellent cure for the mental loneliness of the past two years.
So, what did I learn from this event—other than a lot about health insurance, training people in disparities research, LGBTQ+ health access program, etc.? Convening is a very important part of the academic and professional and human process. Convening in person with other people in the same room creates safe dialog, allows for preposterous questions and new ideas, field tests opinions, and introduces people for more collaboration. Prior to our recent unpleasantness, with my global health team at ASCP and in my global health volunteer work at Harvard, we had been using video conferencing tools for years. I was a beta tester for Zoom before it was Zoom. I had been on 5 different meetings in one day using 5 different platforms. Videoconferencing was just a tool that we had to use to talk quickly and constantly with people all over the world. But we still had coffee in the break room, weekly in person meetings, and curbsides with other staff, etc. When the switch to complete videoconferencing occurred for all day work and, along with it, the inevitable virtual conference to replace a live meeting, the loneliness of expertise grew to an almost insufferable level. The cure, however, exists and it is in the live, in person meeting.
Note: Thanks to Matthew Schultz, Jeff Jacobs, and Suzanne Ziemnik of ASCP for their insightful ideas about this topic and input on this blog post.
- Barnes JM, Johnson KJ, Boakye EA, Schapira L, Akinyemiju T, Park EM, Graboyes EM, Osazuwa-Peters N. Early Medicaid Expansion and Cancer Mortality. J Natl Cancer Inst. 2021 Jul 14;113(12):1714–22. doi: 10.1093/jnci/djab135. Epub ahead of print. PMID: 34259321; PMCID: PMC8634305.
- Han X, Yabroff KR, Ward E, Brawley OW, Jemal A. Comparison of Insurance Status and Diagnosis Stage Among Patients With Newly Diagnosed Cancer Before vs After Implementation of the Patient Protection and Affordable Care Act. JAMA Oncol. 2018 Dec 1;4(12):1713-1720. doi: 10.1001/jamaoncol.2018.3467. PMID: 30422152; PMCID: PMC6440711.
- https://familiesusa.org/resources/momentum-on-medicaid-expansion/

-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
