I’ve appreciated some amazing feedback from my previous post discussing how doctors can sometimes be patients too, and the challenges one might face in different roles within our health care system. Not only a challenge of roles, but those that struggle with invisible illness have unique perspectives on patient care.
That said, this month let me take a break from all the fun content found between cases, concepts, and trends in pathology and laboratory medicine, and celebrate our amazingly successful (and virtual) Annual ASCP Meeting!
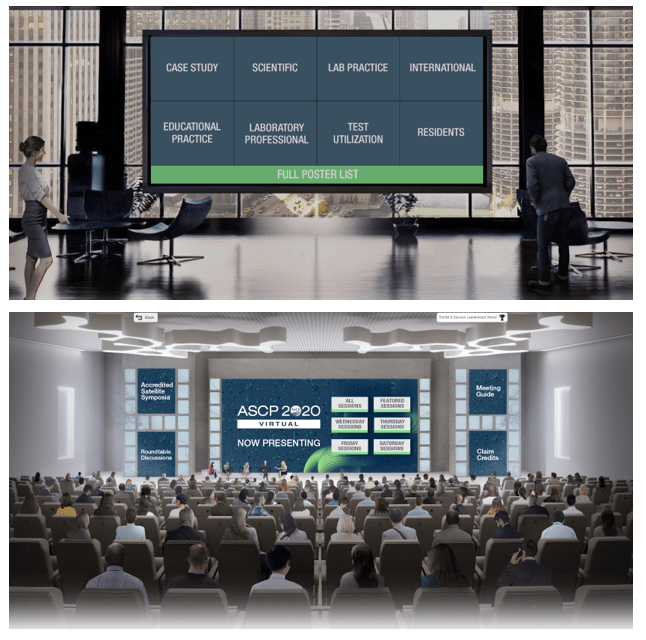
Image 1. Just look at this virtual lobby! Set aside that in-person connectivity dissapointment and just appreciate the quality put into this visually! More of my oggling to come in further images…
It was awesome. But don’t just take my word for it, we’re all people of science here, right? So let’s do it by the numbers!
133 educational sessions
3 general sessions
4 named lectures
36 round table sessions which included topics like wellness, problem-solving, collaborative solutions, and “birds of a feather” breakout discussions
9 virtual video microscopy sessions
8 session dedicated to laboratory professionals covering hematology, chemistry, microbiology, and blood banking
6 resident board review sessions
15 companion society sessions
14 sessions related to wellness
4 sessions discussing diversity and inclusion
10 COVID-focused sessions
20 grant funded sessions
4 virtual patient symposia (more on this topic below…) and
And 300+ posters!
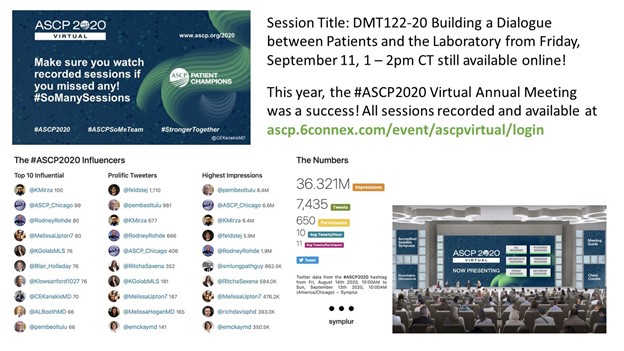
Image 2. More visual appreciation here: virtual sessions felt like you were really in a large, collective meeting of enthusiastic, like-minded laboratory professionals all learning, collaborating, and networking together!Image 3. I was fortunate enough to to speak on this amazing panel regarding direct patient-and-pathologist interactions, making laboratory medicine and the overal healthcare experience, safer, more accessible, more interdisciplinary, and better equiped at dealing with the forefront of medical diagnostics!Image 4. So, the session went well! Just look at that social media data: 36 million impressions over 3.5 days! That’s 1 million people engaging ASCP topics a day, or 12 people per second! All actively discussing and collaborating topics in pathology and laboratory medicine.Image 5. How could I (of all people) ignore the fact that #ASCP2020 featured an amazing social (media) lounge where people from all over could connect, chat, network, and relax! There were interactive, virtual sessions covering all kinds of non-lab med stuff: yoga, meditation, mixology, and cooking! I hope this is a permanent addition to future (hopefully) hybrid in-person/virtual meetings.
What more could you ask for? The folks that run the logistics and planning for the ASCP Annual Meeting outdid themselves again. Sure this content would excite anyone in the field for 3 dedicated days of immersive learning and networking, but all this and more are still available online for virtual on-demand recorded viewing! Missed a session? No worries, it’s still waiting for you for about 6 months (through March of 2021). All the buzz aside from ASCP members having free access to all of this content, the excitement started months before the meeting went live. Estimates are still coming in, but membership grew by a couple hundred in the weeks leading up to the meeting—not surprising: free access for members? That was an excellent deal, so choice.
Image 6. The start of the #ASCPSoMeTeam’s amazing trajectory culminated at #ASCP2019 in Arizona, the more we work together the more we can accomplish for our profession and our patients, #StrongerTogether.Image 7. ASCP’s Resident & Pathologist Councils are invaluable assets to promoting and advancing all of our professional development. #ASCP2020 was no different! From virtual fellowship fairs to online, interactive resident council sessions, there was a lot to take it—still available online!Image 8. I’ve talked about previous ASCP Annual Meetings here and here, and while I can’t list every single aspect of what made this meeting (virtually) amazing, members can check in for about 6 months and see for themselves the quality and attention to detail that comes directly from our collective passion to make pathology and laboratory medicine better, for everyone. Kudos to the ASCP leadership and logistics teams that made this all possible!
Great to see you all at the meeting!
Thanks for reading! See you next time!
-Constantine E. Kanakis MD, MSc, MLS (ASCP)CM is a new first year resident physician in the Pathology and Laboratory Medicine Department at Loyola University Medical Center in Chicago with interests in hematopathology, transfusion medicine, bioethics, public health, and graphic medicine. His posts focus on the broader issues important to the practice of clinical laboratory medicine and their applications to global/public health, outreach/education, and advancing medical science. He is actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Watch his TEDx talk entitled “Unrecognizable Medicine” and follow him on Twitter @CEKanakisMD.
Thanks for reading my piece last month on liquid biopsies. And, as a side note, there is a growing number of awesome quality content and posts from pandemic response, to inclusion, alongside COVID and case-studies so subscribe, share, and add this page to your bookmarks—STAT! Lablogatory has been a fantastic platform to share and learn so much in this past year, I could barely keep up!
Or super-STAT if you’re one of those people…but hey, that language belongs to all of us! Lab professionals, nurses, scientists, and doctors alike. And this month, I just want to take a quick moment to celebrate a milestone.
I’m officially a resident physician/trainee, medical post-graduate! (There was confetti falling just now on my end, not sure about yours, but work with me here.) It’s just one of those life-goals that feels great when you get there. But there’s a lot more to it than it seems…if I told you being a pathology resident means sacrificing early adulthood, amassing soul-crushing debt, and explaining to your peers and colleagues what it is exactly you do and why you also bear the moniker of “physician,” you’d delete that bookmarked webpage faster than I can make you scroll through this thing.
(oh good you’re still here!)
All that said, I’ve got to say: it’s worth every single bit of it. Times a million. But I really did mention some red flags that, were we discussing any other work environment, would make you definitely think twice before committing 5-10 years of your life. Furthermore, as a PGY-1 in pathology, I could stand next to any other patient-facing PGY-1 colleague (read: intern) and they wouldn’t have the faintest about what I actually do. Listen, the “lifestyle” specialty, generally 9-5er, no weekend, no 24hr call isn’t something I’m shy to celebrate, but it’s not the whole story. I’ve matched and started learning and working at a great institution with great faculty, mentors, and other residents/fellows. Bottom line: I’m more than a little happy about where I’m at professionally.
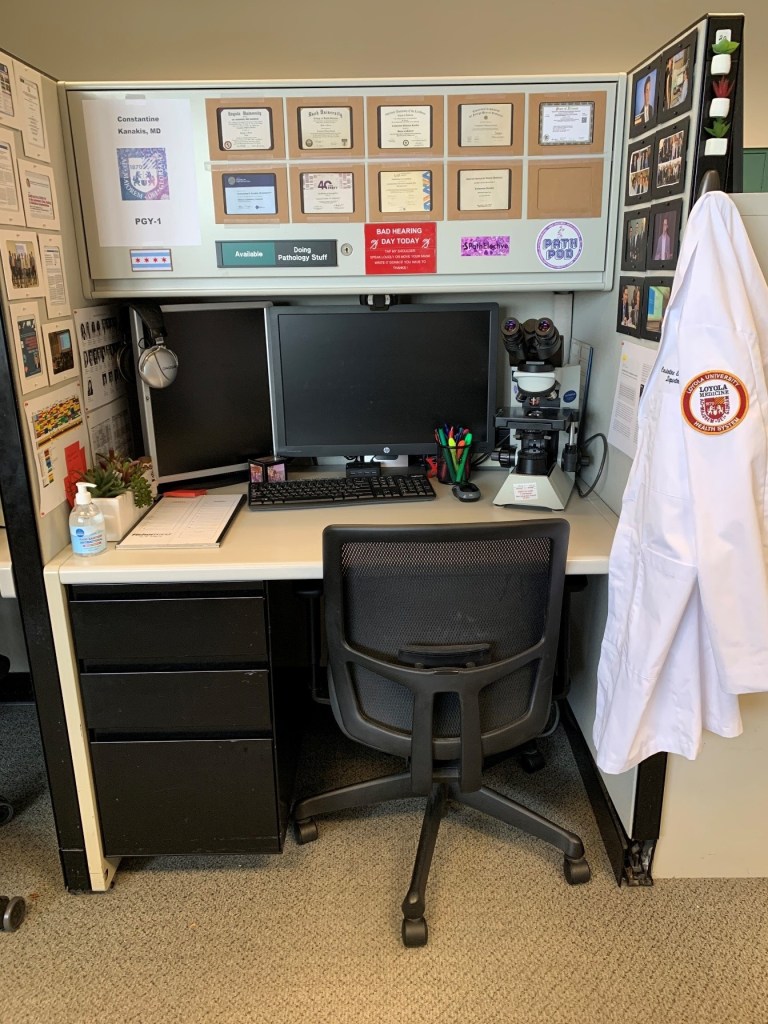
Image 1. Most path & lab med residents get cubicle-style desks to spend time reading, prepping, writing, learning, and previewing cases between responsibilities in sign-outs, tumor boards, or OR/gross room work. Most of my non-path friends don’t like this. It makes me very happy.
So, to my non-pathology friends, what is it exactly that I do during my residency training while you might be busy rounding, managing glucose levels, triaging cases, putting orders in—you know, regular intern stuff *shudders* … (pathology trainees don’t have an intern year, we jump right into the specialty and go for 3-4 straight on through). Like most of you I have a transition period where I get acclimated to the workload and patterns of my specific residency, but sans-anno-interna, I’ve got lots of work ahead to climb the steep learning curve that med school pathology merely skims.
What does non-patient-facing mean, exactly?
Well, without an intern year you jump right into what most path residents go into which is a 4-year combined anatomic and clinical pathology (AP/CP) track. You immediately begin training in all the fields in pathology. They include surgical pathology (of various sub specialties like head-and-neck, gynecologic, gastrointestinal, thoracic, neuro, etc.—think surgery, then add pathology), autopsy training, dermatopathology, cytopathology, hematopathology, transfusion medicine, clinical chemistry, microbiology, hemostasis and coagulopathy, pediatric pathology, forensic pathology, molecular, training as a laboratory director, and much, much more. Each of these services has a workload which is usually comprised of cases from biopsies and grossed specimens for histologic analysis (anatomic pathology) or the ongoing maintenance and advancement of clinical diagnostic testing through laboratory methods and management of staff/resources (clinical pathology).
Image 2. August 2019 Issue of The Pathologist magazine. Pathologists, medical students, microscopes, you get it…Specifically, that’s one of my mentors (and now faculty) Dr. Kamran Mirza and (then) medical student Austin McHenry discussing the critical role pathology plays in every circle of medical care.
When I say “non-patient facing” this means that the majority of that work is not done in 1-on-1 settings with patients in a clinic or hospital floor. It is done ancillary to their clinical experience whereby pathology attendings manage the simultaneous training of residents and processing of case sign outs for rapid and accurate diagnostic output for our patient-facing colleagues. For example, while a patient, their family, and doctor are discussing and managing symptoms related to a possible cancer diagnosis. The pathologists are examining microscopic behavior of the cancer-in-question’s cells and adding immunohistochemical testing and molecular analyses to identify, stage, and prognosticate that cancer. Returning information about what it is and what can be done back to the patient-facing clinician, who can then best-translate a tailored approach for their patient. Old-timey medical texts would often refer to the pathologist as the “doctors’ doctor,” and I’m not here to hate on that haha. My clinical friends and readers might feel forlorn now at the prospect of 4 years of medical school training to “just look into a microscope all day?” Well, for some folks in path it means a lot more than that, every slide is a patient. So we care just as much as if they were right opposite our desk. But that’s not all we do…
(More on that in a minute.)
So What Do You Do?
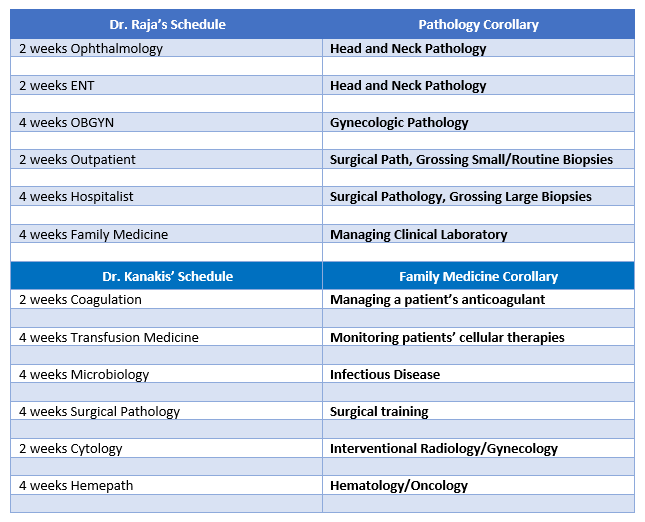
Okay, there are lot of words in path that might act as a barrier to understanding the common ground between me and …let’s say a colleague and friend in Family Medicine. So for the purposes of transparency here’s my friend from medical school Dr. Danash Raja and how a small part of his schedule and my schedule aren’t so different…
Image 3. Dr. Raja is from Alaska, and now works as a resident physician in Family Medicine in Eu Claire, Wisconsin! Alaska! Look at this graduation photo!
On both sides of this table are clinicians managing their patients and ensuring the best possible outcomes. Both sides are deeply vested in intensive hours of training, procedural experience, evidence-based best-practices from the literature, and ongoing continuing education.
Image 4. They see me grossin’, they hatin’…A lot of surgical pathology and microscopy in general revolves around understanding the gross layout of a specimen and its orientation before it becomes a thin microscope slide. As a junior pathology resident, we spend a lot of time up near the OR. Critical skill for a crucial foundation of knowledge.
Literally the biggest differences:
In pathology, I get my own desk space and I need it! I’ve got to start amassing a physical and digital library to supplement the next 4-6 years of subspecialty training for the eventual day when a colleague will see me in an elevator and expect concise, thorough, and actionable material to inform their clinical management from the pathologic diagnosis.
Pathology residents and clinical residents both take “call” except Dr. Raja has to pull grueling 24-hour+ shifts and stay in the hospital for the duration, and I answered a page about a transfusion reaction from a grocery store once.
When a patient thinks about the person who helped them find out what kind of cancer they had and what treatment to begin, they’ll probably think of Dr. Raja or someone patient-facing in Heme/Onc—but I’m working on this, every day!
Bottom line: I’m as important as he is, and he is as important as I am. Our work is what really matters, and what really connects us as clinical colleagues. It’s all about patients, remember? But I’m more than happy to be the pathologist to his patient-facing, diabetes-managing, vaccine-giving, life-improving super hero doctor!
You Never See Patients?
We’re back on this. Remember how I said looking into microscopes isn’t all we do? Okay, well it’s not. And if you’re lucky enough to have matched to as awesome of a place as I did, then you know what I’m talking about. If you’ve read some of my pieces, you know full well my passion in pathology lies in Hematopathology and Transfusion Medicine. I like to sit right on the fence between AP and CP, and mostly look at the green grass on the CP yard. This month, I’ve been on service for Transfusion Medicine and let me tell you about the few weeks…
Image 5. Dr. Kimberly Sanford, ASCP leadership and Director of Transfusion Medicine at VCU was highlighted in The Pathologist magazine for her work outside the laboratory seeing patients every day, and encouraging residents to do the same and do what pathologists do best: enrich and improve the channels of communication so patients better understand their conditions and the medical process.
I, a pathologist trainee, resident physician, under the supervision of two attending physician pathologists have been seeing and following up on patients nearly every day. Gasp! No, I’m not part of some backwards resident exchange program (because OMG how dangerous haha), no I’m not lost, no I’m not being overly gunnery, that’s it, that’s the Tweet. Seriously, it’s just part of the service. Larger academic hospitals with robust clinical blood bank services often have apheresis clinics and I find myself working exactly there. Blood bank/Transfusion Medicine is one of those subspecialties where patient contact is part of the routine. At some institutions, I’ve been a part of some pathology-led teams that procure the bone marrow aspirates from their patients in Hemepath service, or conducted their own fine needle aspirations for cytology service, or dermpath services that operate in clinics alongside their dermatology colleagues—I’ve even been working on frozen sections and surgical path grossing when called into an operating room to discuss methods and approach for biopsy! There were patients at every turn, all with pathologists on the front line! Dr. Syed T. Hoda (@01sth02 on Twitter) from NYU Langone often says, “Person FIRST, doctor SECOND, specialist THIRD.” And trust him, he’s a bone and soft tissue pathologist that left the lab and went to the floors to help clinical staff when overwhelmed during the peak of the COVID crisis in NYC. So for my dual-interests, I would say I’d expect to see quite a bit of patients in my future practice.
Image 6. My awesome co-residents! (Left-to-right): me, Dr. Elnaz Panah, Dr. Aayushma Regmi, and Dr. Sandra Haddad—you’re going to hear more about them, don’t worry.
So, would I pick pathology again? Uh, yeah! Without a single hesitation. Every day at work I am reminded that I am at the right place, with the right co-residents, the right faculty and mentorship, and the right environment to train and hone my future skills for a career that lines up exactly with what I want to do.If you’re interested about the intersections between clinical medicine and pathology, and want to learn more about “patient-facing pathology” keep an eye out during the 2020 ASCP Annual Meeting for a talk by yours truly as part of a panel discussion on communicating directly with patients! Register now! Free for members.
See you next time!
BONUS: did you notice that I referenced The Pathologist magazine a bit in this post, well it’s because they named me to their Pathology Power List for 2020! An exclusive, international list of 80 professionals in the field of pathology and laboratory medicine who contribute and advance the profession every day! I was highlighted for my active social media work and my response to the early COVID pandemic in Manhattan, NY.
-Constantine E. Kanakis MD, MSc, MLS (ASCP)CM is a new first year resident physician in the Pathology and Laboratory Medicine Department at Loyola University Medical Center in Chicago with interests in hematopathology, transfusion medicine, bioethics, public health, and graphic medicine. His posts focus on the broader issues important to the practice of clinical laboratory medicine and their applications to global/public health, outreach/education, and advancing medical science. He is actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Watch his TEDx talk entitled “Unrecognizable Medicine” and follow him on Twitter @CEKanakisMD.
I’m writing to you now back in Manhattan after visiting
sunny Phoenix, AZ for this year’s ASCP Annual Meeting. Last month
I talked about downtime, pathology emergencies, and introduced you all to our
insightful and dynamic colleague, Jalissa Hall. It was great working with her
and one of the last things we talked about was getting to go to professional
society meetings. We also talked about the upcoming meeting next year in
Austin, TX! And that’s exactly what I’d like to talk about with you this time:
why going to meetings like ASCP is not only educational, but an excellent way
to network with your laboratorian peers from around the country.
Image 1a. My wife and I made it to the Phoenix Hyatt Regency on registration day! ASCP swag on, obviously.Image 1b. Behind the Scenes – Hosting the ASCP 2019 Facebook Live broadcast with two fantastic colleagues, Dr. K. Mirza and Dr. A. Booth! Did you catch us? But more about social media later…
I couldn’t go to every single session—there’s just too
many—but I did learn so much valuable, practical information at the educational
sessions. Here are just a mere few insights from the long list of fantastic
speakers I had the chance to visit!
I participated in an interactive session on the
ASCP/CAP/ASH guidelines for lymphoma workup…
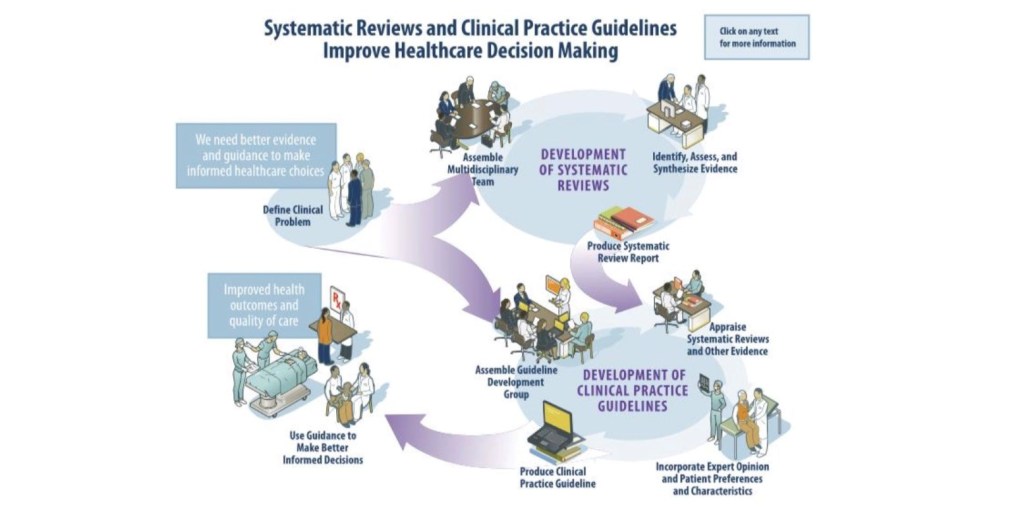
Figure 1. All the multidisciplinary expertise must go through rigorous adjustment and evaluation all the way throughout the process of seeking out and publishing proper guidelines. (Source: ASCP 2019 session 5007-19; Kroft, S., Sever, C., and Cheung, M.)
Drs. Kroft, Sever, and Cheung discussed updates from the WHO
2016 guidelines as well as relating any changes in concurrent literature to
appropriate diagnostic accuracy with evidence-based guidelines. If it sounds
familiar, it’s because I talked about these guidelines a
few months ago! In my month clerkship at The Mayo Clinic in Rochester, MN I
presented a therapy-related AML case in the setting of Li-Fraumeni disorder. In
my discussion I stressed the utility and importance of having organized and
algorithmic guidelines to diagnose patients accurately, effectively, and
timely. This time, instead of just talking about the guidelines, I got to
listen to some of the folks who actually put them together—and,
according to them, it’s no easy task!
I learned about culturally appropriate leadership
training…
Figure 2. The panelists each had something insightful and moving to contribute to this wonderful discussion on female empowerment in our profession, and ultimately how it relates to improving patient care! (Source: ASCP 2019 session 8012-19; Mulder, L., Upton, M., Vuhahula, E., Abedl AlThagafi, M., Papas, F., and Sanford, K.)
This year’s ASCP president, Dr. Melissa Upton moderated this
fantastic panel and opened with an old proverb: “If you want to go fast, go
alone. If you want to go far, go together.” This was definitely a theme for
each of the mini-sessions’ discussions. ASCP’s own Lotte Mulder discussed her
research on culturally applicable leadership training using her Leadership
Institute Initiative. She talked about countries that are culturally different
and developmentally different up and down the spectrum can all benefit from
leadership development and opportunity. Next came Dr. Edda Vuhahula, an
accomplished physician, educator, and advocate in Tanzania. She related her
experiences of women in leadership roles, and challenges on the horizon as more
women rise to these positions every day. Dr. Malak Abed AlThagafi talked about
her “hats:” as an entrepreneur, a medical director, and a researcher in her
whirlwind story of empowerment and accomplishment. Finally, medical laboratory
scientist and former Philippine Army colonel, Filipinas Papas gave her personal
perspectives on sexism, education, bias, and opportunity.
Celebrated my colleagues and my contributions to the 6thChoosing Wisely list of recommendations…
Figure 3. My totally biased favorite slide from Dr. Lee H. Hilbourne, chair of the ASCP Effective Test Utilization Steering Committee. It’s an honor to be included in this year’s list, alongside so many accomplished contributors.
The Choosing Wisely initiative, partnering with the
American Board of Internal Medicine and many other specialty organizations, is
one of my favorite programs at ASCP. To date, our lab medicine organization has
the highest number of effective test utilization recommendations. ASCP seeks
active contributions to our expanding lists of recommendations to eliminate
wasteful, unnecessary testing and to improve patient outcomes. This talk was
also a great opportunity to honor the ASCP 2019 Choosing Wisely
Champions: Dr. Gary W. Procop from the Cleveland Clinic, Dr. Lucy Nam from the
Inova Lab best practice team, and Dr. Alyssa Ziman from UCLA Health. Want to read
the most updated list of recommendations ASCP made to the Choosing Wisely initiative?
I watched some cutting-edge exchanges about cellular
therapy…
Image 2. Here I am with laboratorian S. Malakian and Dr. Gastineau with The Mayo Clinic after they discussed the future of complex cell therapies.
One really effective take-home message from this seminar was
that, if we’re going to rely on cellular therapy in the future—especially as it
relates to “individualized medicine”—then who do you think should be in charge?
Who’s got the most experience and knowledge when it comes to cell storage,
transfusion protocol, patient outcomes, and high reliability? Short answer:
it’s us. Long answer: go back and check out a piece
I wrote about high-stakes responsibility in and out of the lab!
Popped into fascinating hematologic cases at our
neighboring SHEAHP2019 meeting…
Listen, I like hematopathology, I’ll be the first to tell
you that. There were so many people giving presentations in this near
standing-room-only meeting, that I recognized from papers, abstracts, and
journals that I’ve read in the past year alone! There were so many interesting
sessions at this meeting, I wish I could have seen more…
Image 3. Here’s Dr. J. Dalland from Mayo Clinic Pathology discussing a lymphoproliferative disorder with associated eosinophilia. These talks go deep into morphology and photypic patterns, so that Hemepath colleagues have a chance to assess their workup and protocols. It’s also great learning for avoiding pitfalls—this case shows architectural changes in lymph nodes which could cause someone to misdiagnose!
Learned how to create an impactful dialogue with patients
directly…
What do you do as a pathologist when a patient wants to
speak to you? Yes, you. Not a typo! This was the last talk I went to and it was
a great way to close out this awesome conference.
Image 4. Me with (left to right) Dr. K. Sanford from VCU, Patient Champion Anthony Reed, Dr. M. Sitorius from the University of Nebraska, and M. Mitchell. All of these individuals had amazing things to say about bridging the gap between the bench and the bedside!
In their own ways these patient advocates demonstrated that
if you want to represent our lab profession as one of accuracy, answers, and
hope, we’ve got the skills and resources to do it! Dr. Sanford sees so many
patients in her transfusion services and discusses their care plans regularly.
Mr. Reed is an ASCP patient champion who, after being diagnosed with ESRD,
became a learned lab ally. Dr. Sitorius is a family medicine physician at a
pathology conference, talking about empathy and connection! Ms. Mitchell has
done fantastic work with her pathology colleagues after beating cancer and
fighting for patient education every day! These folks have taken our field of
laboratory medicine to its outer edges, touching patients’ lives directly—and I
left energized to take it further in the future.
And of course, I learned so much about the utilization of
social media as a practical tool for education, advocacy, and outreach…
I can’t list every single session, lecture, keynote,
presentation, or panel in this article. This was just a glimpse of what
meetings like this have to offer. You will learn, obviously, but you’ll also
gain access to new perspectives and meet people who reinvigorate your passion
for your profession in ways you didn’t even consider. One of the most
fulfilling experiences of this meeting was being on the ASCP Social Media Team!
Posting to Instagram, Facebook, and Twitter with the hashtags #ASCP2019,
#ASCPSoMeTeam, or the scavenger hunt #ASCPiSpy was a great way to bolster our
enthusiastic network. This was my third ASCP Annual Meeting, and I met so many
wonderful people I can’t wait for the next one! Here’s a few of my favorite
snaps from the meeting:
Image 5. Here’s part of our amazing #SocialMediaTeam: (left to right) A. Odegard from Baptist Health, myself, Dr. S. Mukhopadhyay from the Cleveland Clinic, Dr. A. Booth from the University of Texas, and Dr. K. Mirza from Loyola Chicago!Image 6. At my first ASCP meeting in California, Jeff Jacobs, ASCP’s Chief Science Officer, gave me some of the best advice for my own personal and professional growth, “Stay Humble” he told me. Nearly 5 years later, he added “Don’t Give Up” on goals, yourself, or anything in life. You can’t pick that up in a path review book. I feel lucky to know people like him.Image 7. #SoMe FTW (Social Media for the win!) At this great talk, Dr. C. Arnold, Dr. L. Shirley, and Dr. D. Gray III, all from the Ohio State University discussed how to use social media to build a reputation and expand your impact as a pathologist, educator, and advocate!Image 8: Conferences are a great time to run into old friends and colleagues whom you may have spent a month rotating with! If you read about my time at Danbury Hospital in Connecticut, Drs. O. Olayinka and G. Kuar were part of it and I’m glad to call them friends!Image 9: Presented by the ASCP Resident and Pathologist Councils, this was a great networking session to discuss fellowships, employment, and how to plan for the first 100 days of working in laboratory medicine from PGY-1 and on! I certainly learned a lot!Image 10: (left to right) Dr. K. Chaztopoulos from the Mayo Clinic, myself, and K.C. Booth, RN in front of his finalist poster in the scientific category! Another valuable professional connection and friend made through my experiences in laboratory medicine.Image 11. When one of your mentors (Dr. K. Mirza) is signing copies of The Pathologist magazine that featured him on the cover, you get in line for one …obviously.Image 12. Dr. M. Upton is an inspirational speaker and insightful individual both on stage and in person. She had words of encouragement for my upcoming residency interview season and made sure I felt I could rely on ASCP for whatever I needed professionally. Thank you, Dr. Upton!Image 13. Some more colleagues from Mayo Clinic Pathology (left to right): Dr. A. Ravindran, Dr. D. Larson, Dr. J. Dalland, and myself. These folks were very busy with all the great hematology sessions at the SHEAHP2019 meeting.Image 14: No ASCP Annual Meeting would be complete without the leadership, passion, and vision of our CEO Dr. Blair Holladay. He, his leadership team, and this organization have been integral in my path to pathology and I can’t wait to see what’s in store for the future!
Social media has become so valuable in our field. Not just
for networking, but sharing cases, impressions, publications, and more! It’s so
easy to rally behind a hashtag and support a cause in so many instances—why not
in our profession? Get involved, be an active voice for your own practice as
well as your colleagues.
If you want to learn more about the sessions you may have
missed, download the ASCP2019 app from the Apple App Store or Google App Store!
Thanks for reading! See you on social media, because when we
communicate and collaborate, we are #StrongerTogether! I’m on twitter at
@CKanakis, until next time!
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola
University Chicago with a BS in Molecular Biology and Bioethics and then
Rush University with an MS in Medical Laboratory Science. He is
currently a medical student actively involved in public health and
laboratory medicine, conducting clinicals at Bronx-Care Hospital Center
in New York City.
In the previous 2 blog posts we discussed how to prepare for your inspection, and what to expect during the inspection itself. In the last of our 3 part series on regulatory inspection preparedness, today we’ll be covering what to do after the inspection ends.
Throughout the inspection itself, the inspectors should be communicating any issues or citations they uncover; ensure that your management staff is taking notes on any of these potential findings. Based on these notes, you should start working to address and correct any issues right away. Formal documentation regarding the nature of any official citations can take several weeks to receive back, depending upon the regulatory agency performing the inspection. Waiting for the formal report to begin making corrections will reduce the time you have to form a plan of correction, and can further impact patient care depending upon the citation received.
Have a Plan. Draft a spreadsheet to record: 1) each issue identified, 2) laboratory department(s) it was found in, 3) associated risk factor (patient care or safety issues = 1, regulatory requirements = 2, recommendations = 3), 4) staff member assigned to investigate and correct the issue, 5) due date for investigation response, and 6) status of the investigation (in progress, on hold, completed). Share this spreadsheet with your management team, and review at weekly/monthly staff meetings for updates on progress completion.
Risk 1 Issues. The safety of your patients and staff, along with ensuring accuracy in testing results is the number one priority of a laboratory. If the inspectors identified any weaknesses in these areas, they should be addressed first. This would include items such as staff not adhering to required safety precautions, not following manufacturer requirements for quality control testing or instrument maintenance/calibration, lack of follow-up for QC or proficiency testing failures, along with any other finding which questions the integrity and accuracy of the testing being performed.
Risk 2 Issues. Double check the regulatory standard to ensure you fully understand the requirements, and that you have appropriate evidence of compliance. As the testing activity menu and complexity of testing increases, the amount of documentation requirements can increase as well. Even with a paperless system, it is easy to overlook a signature of review or checkmark on a log. “If it’s not documented, it wasn’t done.” For simple administrative oversights, review your current processes to identify any gaps or areas that can be improved upon to ensure all documentation is properly filled out each month. If the inspectors noted a discrepancy between your current policy and how staff are actually performing a test, review the testing process to see where the true discrepancy is – is the policy outdated and needs to be revised, or do staff need to be retrained on the current policy with competency assessed for compliance?
Risk 3 Issues. Inspections are a great opportunity for further education for all those involved, both the inspector and staff being inspected as well. For some regulations, there is no one set way that must be followed in order to demonstrate compliance with a requirement. Hearing how someone else is meeting the requirements may spark an innovative idea from your own staff on how your current processes can be improved. Be open to hearing new ideas, and find ways to implement those which you feel would be successful at your institution.
Evaluate All Sections of the Lab. When investigating a finding in one laboratory department, ensure that any process improvements are shared across all areas of the lab. Just because microbiology didn’t get caught with expired reagents like hematology did this inspection, doesn’t mean that they aren’t at risk for future inspections.
Focus on the Positives. Congratulate and recognize your staff on their successes in the areas you performed exceptionally well in. It’s a joint effort to ensure the lab is inspection ready; be sure to pass along any compliments received throughout the inspection process to all levels of staffing. Focus on what you’re doing well and how you can continue to maintain those processes and implement them in additional areas.
A little bit of preparation ahead of time will make the inspection process smoother and less stressful for all involved. When viewed as a learning experience and opportunity for improvement rather than a visit from the “lab police”, laboratory inspections can be a useful tool to confirm the quality of your overall laboratory program.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s 2018 Top 5 in the 40 Under Forty recognition program. She has worked in the medical laboratory profession for over 18 years. In her current position, she transitions between performing laboratory audits across the entire Northwell Health System on Long Island, NY, consulting for at-risk laboratories outside of Northwell Health, bringing laboratories up to regulatory standards, and acting as supervisor and mentor in labs with management gaps.
Over the last few blog posts I have spoken about my involvement in the laboratory and hospital to find other people interested in clinical pathology. While this has helped fuel my passion for laboratory medicine, one of the issues that made me feel the loneliest was the responsibility I felt as a new pathologist and not having someone to help share that burden.
As a pathology trainee I saw several new pathologists start their positions in microbiology, hematology, and even anatomic pathology. They always seemed to be cool, calm, and collected (unless they were running around trying to get their research published). What I did not focus on was that they also had a built-in mentor (the experienced pathologist) who was there to discuss a tough case or help them make a difficult decision.
When I took a community practice based job I was immediately entrenched in a decision making role. The sense of responsibility I felt to our patients, and making sure those decisions affected care in a positive way, was more overwhelming than I expected. The decisions included items such as which instruments to bring into the lab, when to report certain isolates, and even how to handle irate clinicians about the way we report our results. Every time I encountered a new situation I had not experienced first-hand in residency, I wanted to run my approach by someone to make sure it was the right way of doing things. I had one mentor I am pretty sure I texted every day the first two weeks of my job (thanks Dr. Lars Westblade!) for every single technical question that came up in microbiology. While it may seem excessive, it was the only thing that gave my decision making confidence at that time.
As the year went on, other mentors from training were also there for me, but I realized I needed a mentor on site that I could run major decisions by, as they understood the environment I was in more than my training mentors could. I was hesitant to seek advice from my bosses, as I was hired for my clinical pathology expertise, but as I reached out for guidance, I came to find the senior pathologist could guide me in the politics of my current situation while I could make decisions on the technical background. I can now see that having a senior pathologist with a wealth of information on how to handle situations and clinicians has been invaluable to the start of my career. The wisdom imparted has given me direction and experience in making decisions that residency could not fully prepare me for, such as handling physicians not happy with aspects of the lab or employees who did not want to perform tasks I asked of them.
Beyond individual mentors, another area that helped me with technical aspects of my job has been belonging to clinical pathology societies. American Society for Microbiology has several different list-serves you can post questions and get answers back from experts all over the country and world. The American Association for Clinical Chemistry has a board called “The Artery” that you can also post questions to and experts will answer. These formats have been priceless when seeking advice on certain topics literature does not seem to cover and are examples of why belonging to professional societies really bolsters your career.
As the year has progressed and I have made one decision after the next, my confidence has been built up so that I don’t have to discuss every decision with my mentors; that being said, I still have them on speed dial. While I think that responsibility is one area that residency was not able to fully prepare me for, I can see that it is a work in progress and one aspect of my job that will continue to motivate me to be the best I can be and make the best decisions for our patients.
Now to hear from you: did responsibility overwhelm you your first year of practice? How do you utilize mentors and professional societies to help approach unique and new situations?
-Lori Racsa, DO, is the director of microbiology, immunology, and chemistry at Unity Point Health Methodist, and a Clinical Assistant Professor at the University Of Illinois College Of Medicine at Peoria. While microbiology is her passion, has a keen interest in getting the laboratory involved as a key component of an interdisciplinary patient care team.
As I mentioned last month, a big part of my job has been to do daily rounds through the lab to seek out areas that need troubleshooting. One point I noticed was technologists don’t always see the impact of their work on patient care. I wanted to make sure they knew the importance of their work so I decided to incorporate education as a tool to highlight how their work directly affects patient care. Each section of the laboratory has their own ways of communicating so I have done something a little different in both labs.
In the microbiology section, I started a weekly “formal” microbiology rounds with the infectious disease doctors, the pharmacists, and the technologists. While I saw this rounding at both of my training institutions, there were held in different styles. In one, the infectious disease team rounded through the lab and asked the techs questions about their patients; in the other, the team discussed interesting case around a microscope. I decided to take a combined approach: we meet in the lab at the microscope so the techs can work if needed yet still be a part of the discussion. The techs save interesting cases that have come up over the last week or so and we show the rest of the team. It usually involves discussing organism identification methods as well as the disease process associated with the organism. This has given the techs the chance to ask the physicians and pharmacists questions about the patient isolates they have worked on directly. In addition, it has given them the opportunity to ask why physicians order certain tests. The pharmacists have added so much to these rounds and it has been nice to see a collaborative effort between multiple areas of the patient care team come together and talk about why things are done and the outcome of the patient based on laboratory results. It demonstrates to everyone that each member of team is passionate about patient care. In order to bring some of this knowledge to the second shift staff that performs microbiology processing, I save one or two interesting cases from rounds and present a quick rundown of what the bug is and how it is identified in the lab so they can see how their work is completed the next day.
For chemistry and immunology, the laboratory team has a monthly meeting. At each of these meetings, I run through a formal case presentation based off interesting cases the techs have come across or have had questions on specific disease processes related to the laboratory work they are performing. The topics have ranged from beer potamania (that got a lot of discussion!) to what polymerase chain reaction is. It has been another approach to show the technologists how their work directly impacts patient care and they have really enjoyed it. The goal is to bring clinicians into these discussions, as well, but that has not been as easy for these meetings. We have been able to bring a pharmacist in to discuss vancomycin trough levels and why draw times are so specific. It really helps having other departments reach out to the laboratory staff to let them see why policies are structured the way they are.
I really enjoy being in the lab and interacting with the technologists, however, one of the principal lessons I have learned this year is how important it is to get out of the laboratory as a clinical pathologist. The next couple of months I will talk about how I have gotten involved in other areas of the hospital. But for now, let’s hear from you, do you have any formal rounding or education that you offer your techs? What ideas have had the best responses from the technologists? I am looking forward to hearing more ideas on how to integrate education and interdisciplinary teamwork for our laboratory staff.
-Lori Racsa, DO, is the director of microbiology, immunology, and chemistry at Unity Point Health Methodist, and a Clinical Assistant Professor at the University Of Illinois College Of Medicine at Peoria. While microbiology is her passion, she has a keen interest in getting the laboratory involved as a key component of an interdisciplinary patient care team.
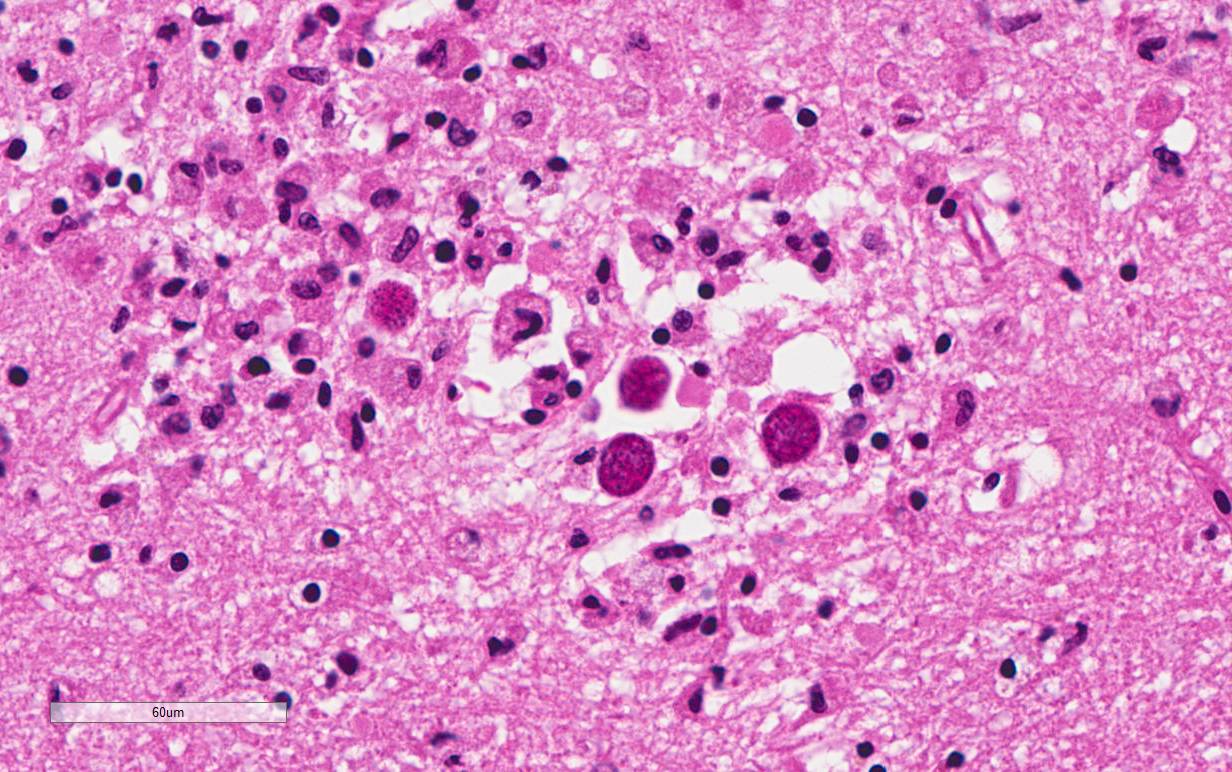
A 47-year old woman with a past medical history of Systemic Lupus Erythematosus (SLE) and liver cirrhosis of unknown etiology was admitted to the hospital for back pain and new onset neurological symptoms. She soon developed pancytopenia and study of her peripheral blood smear showed evidence of thrombotic microangiopathy. ADAMTS-13 inhibitor was negative ruling out thrombotic thrombocytopenic purpura (TTP). She then developed multiple thrombi, including a nonocclusive thrombus in the superior mesenteric vein with extension to the splenic vein as well as a femoral deep vein thrombosis. Her hospital course then became complicated by lupus cerebritis, a small ischemic focus in the left corona radiata and the left medial midbrain, and decompensated liver failure with hepatic encephalopathy. Despite intensive medical treatment, she became hypoxic and hypotensive requiring pressors, and expired in the ICU after several months of hospitalization. The autopsy was performed based on the relative’s request to better understand pathological processes that lead to patient’s demise. The flowing images were obtained from the brain at autopsy (Image 1).
Light microscopy of H&E-stained sections of the hippocampus reveal encysted Toxoplasma bradyzoites as well as extracellular Toxoplasma tachyzoites in the CA1 region, suggestive of a subacute focal infection.
Discussion
Toxoplasmosis is considered to be a leading cause of death attributed to foodborne illness in the United States. More than 60 million men, women, and children in the U.S. carry the Toxoplasma parasite, but very few have symptoms because the immune system usually keeps the parasite from causing illness.
People typically become infected with Toxoplasma by contaminated food or animal-to human routes of transmission. Toxoplasmosis is not passed from person-to-person, except in instances of mother-to-child (congenital) transmission and blood transfusion or organ transplantation.
Persons with compromised immune systems may experience severe symptoms if they are infected with Toxoplasma while immune suppressed. Persons who acquire HIV infection and were not infected previously with Toxoplasma are more likely to develop a severe primary infection. The diagnosis of toxoplasmosis is typically made by serologic testing. A test that measures immunoglobulin G (IgG) is used to determine if a person has been infected. If it is necessary to try to estimate the time of infection, which is of particular importance for pregnant women, a test which measures immunoglobulin M (IgM) is also used along with other tests such as an avidity test. Due to the high rate of falsely positive Toxoplasma IgM testing, the FDA advises physicians testing pregnant women not to rely on the results of any one positive IgM test as the sole determinant for diagnosis of acute Toxoplasma infection.
Diagnosis can be made by direct observation of the parasite in stained tissue sections, cerebrospinal fluid (CSF), or other biopsy material. These techniques are used less frequently because of the difficulty of obtaining these specimens. Molecular techniques that can detect the parasite’s DNA in the amniotic fluid can be useful in cases of possible congenital transmission.
Clinical correlation
The case patient was at risk for developing toxoplasmosis due to SLE disease, and chronic immunosuppressive therapy that she was receiving for the aggressive course of her illness. However, most likely Toxoplasma gondii organisms seen in the brain parenchyma were in a dormant state due to lack of associated inflammation or architectural distortion. Her neurological decline is most likely related to thrombotic microangiopathy. Opportunistic infection is common in patients with SLE. In some patients, it is difficult to distinguish between the effect of infection and exacerbation of SLE because both can produce similar symptoms. There have been many reports of toxoplasmosis in SLE patients, with conditions such as cerebritis and pericarditis mimicking SLE manifestations.
2) Seta N, Shimizu T, Nawata M et al. A possible novel mechanism of opportunistic infection in systemic lupus erythematosus, based on a case of toxoplasmic encephalopathy. Rheumatology (Oxford). 2002;41(9):1072-3.
3) Zamir D, Amar M et al. Toxoplasma infection in systemic lupus erythematosus mimicking lupus cerebritis. Mayo Clin Proc. 1999; 74(6):575-8.
Contributors
Written by Anastasia Drobysheva, MD, 2nd year Anatomic and Clinical Pathology resident, UT Southwestern Medical Center
Image provided by Bret Evers, MD, PhD, Neuropathology fellow,UT Southwestern Medical Center
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
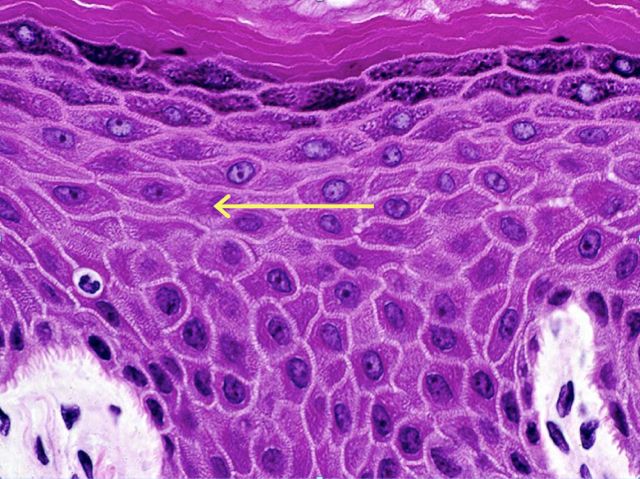
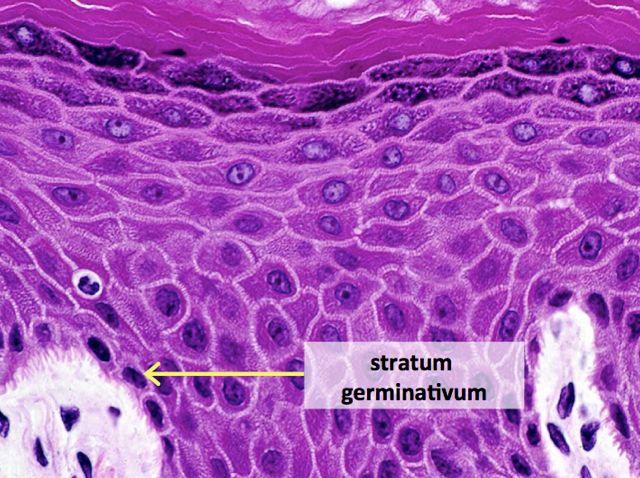
The answer is E, stratum spinosum. The stratum spinosum, also known as the prickle cell layer of the skin, is often several cell layers deep, and is located immediately above the stratum germinativum. Cells in this layer are polygonal, and are connected to each other by numerous desmosomes. During fixation, the cell membrane retracts around desmosomal contact points, giving the cells a prickly appearance. The cells contain many bundles of intermediate filaments as well as keratinosomes, which are membrane-bound granules thought to deposit a “toughening” layer on the surface of the cell membrane.
The stratum germinativum (also known as the basal layer) is composed of a single layer of cells adjacent of the basal lamina. The cells are tall cuboidal or columnar, and are connected to the basement membrane by hemidesmosomes, and to other cells by desmosomes. Cells in the basal layer are mitotically active, and contain numerous polyribosomes and intermediate filaments.
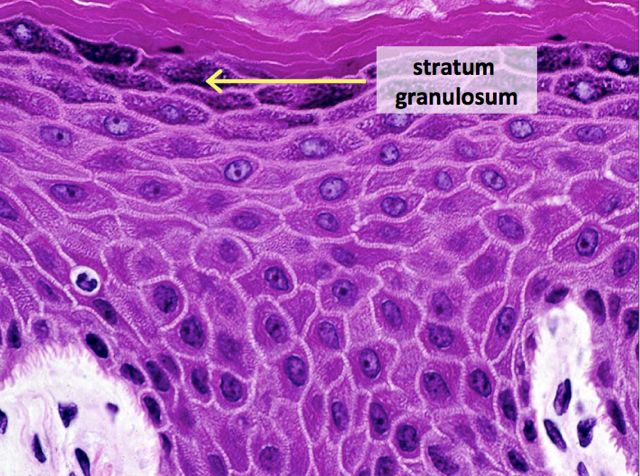
The stratum granulosum is 3 to 5 cell layers thick, and is composed of flattened, polygonal cells arranged with the long axis parallel to the basement membrane. The cytoplasm of these cells contains numerous basophilic granules, called keratohyalin granules, which are thought to be keratin precursors.
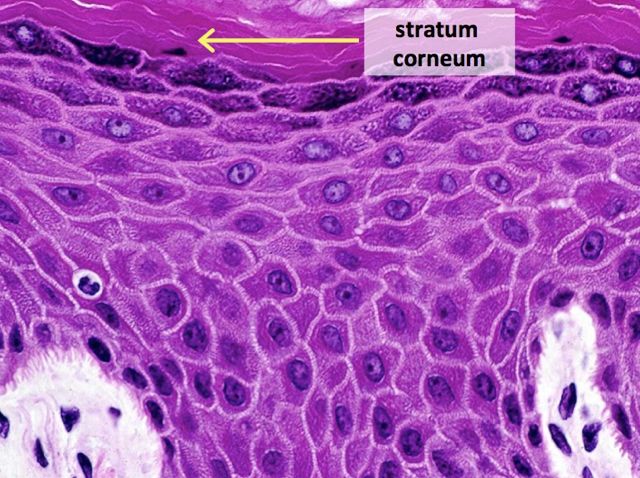
The stratum lucidum is not truly a distinct layer of skin, but rather a staining artifact. It is visible in some sections of thick skin as a glassy-appearing, eosinophilic artifact at the bottom of the stratum corneum. It is not present in this particular image of epidermis.
The stratum corneum is the outermost layer of skin. The thickness of this layer varies considerably from region to region in the body. The cells of this layer are dead, flattened, and fused together, with completely keratinized cytoplasm.
-Kristine Krafts, MD, is an Assistant Professor of Pathology at the University of Minnesota School of Medicine and School of Dentistry and the founder of the educational website Pathology Student.
I haven’t been able to blog as much of late. It’s been a busy year with more than its fair share above the usual crises that a chief resident is expected to handle – an “August year” for me as my program director put it. But I’ve learned a lot and have been lucky to have the support of my attendings, program coordinator, and program director to help. Even when we’ve not always agreed on what is best for our residents, I’ve always been allowed to speak up for our residents and felt as if our concerns were heard and acknowledged even if policies didn’t go our way. I think that’s the biggest strength of a smaller program–the ability to form strong relationships with mutual respect, whether it is with one’s mentors, peers, or hopefully, both–and I know we will cheer each other on when we hear of each other’s accomplishments in the future even if we won’t see each other daily as we do now because of those bonds we built during these past couple of years. The lessons I’ve learned regarding “soft skills” have been equally as important as the knowledge I’ve gained about my favorite lymphomas or molecular mutations. And four years is really shorter than one might think to fit in all we need to as AP/CP pathology residents, so see it for the gift it is–protected time to grow into the physician you want to be. I see the fruits of these lessons more clearly now as I prepare to graduate. Much of it was obtained through mentorship, formal and informal, from those more experienced and with my best interests at heart.
So here are some pearls I’d like to hand down:
Know thyself as early as possible: Be honest with yourself about your strengths and weaknesses so that you can build on the one while working on the other. As we have now signed on to be life-long learners, identify what works for you early or adjust those learning habits which might have worked before but are no longer working. Designate a couple of hours on a weekend day every week to do learning above and beyond what is expected for your current rotation and consistently stick to it. If you can, designating an hour everyday would be even better and it doesn’t have to be hard core studying like our med school days—you can leisurely read a review article, watch TedMed videos, casually look over boards materials or qbanks from day 1, and so forth as long as you do set aside time consistently. Take advantage of experiential opportunities to help decide early where you see yourself as a physician (academics, private practice, commercial lab, subspecialty, etc) in the future so that you can plan as early as possible your rotations, electives, opportunities, and networking with that goal in mind. But most importantly, knowing who you are, what you believe in, how you work best, and what you want and knowing early, will help you plan and see opportunities earlier. But always, be true to yourself.
Time management is key: Learning to plan early and efficiently is a skill and it takes time to learn. Honestly, I’m not the best on a daily basis unless I take time ahead of time to plan my day, which I don’t always do, but plan to be better about during fellowship. But I do know how to plan effectively to juggle multiple long-term projects with deadlines at a time. You will constantly hear about time management – whether on rotation evaluations or during fellowship interviews. I find that those who are very good at time management, all have checklists and planners (whether hard copy or digital) so maybe they’re on to something there. Whatever works for you, being a deliberate planner ahead of time will serve you well.
Be proactive: In some way, we’ve all be conditioned in a passive learning style where those who are more experienced hand down information to us which we are expected to regurgitate or ruminate on and respond. During residency, we don’t have the strict structure we are used to from medical school as we may be only given loose guidelines but are expected to figure out how best to manage our time on our own. We no longer have every hour planned out for us and so the quicker you learn to plan ahead and effectively use your time while at work, the more time you’ll have for personal activities. Don’t just do the minimum but use gaps in your time during the day to study, to build relationships with mentors with whom to work on book chapters, abstract submissions (for posters/platform presentations at conferences), and publications, to attend conferences/tumor boards outside your rotation even in non-pathology departments, to work with others outside of pathology on interdisciplinary projects. In some ways, these activities are networking without our even realizing it. For the rest of our lives, we will constantly be judged and compared to others by our character and work ethic and that often will include tangible items on our CV whether this is fair or not. Challenge yourself on every rotation by trying to do as much as a junior attending would within the limits of what you are allowed to do and not just the minimum.
Get involved in advocacy: Participate in leadership positions at an organized level–within our professional organizations, with interdisciplinary teams within your hospital, or with volunteer organizations in your community. Bringing about change takes time but if done with a positive goal in mind, can have such a rewarding impact on those we wish to serve as well as yourself. You might discover a previously unknown passion or skill you possess that you can share. Before residency, I was heavily involved with on-the-ground, upstream-minded health equity efforts in immigrant and minority communities. And while I took a hiatus from my work due to residency training, I know that as a future public health pathologist-scientist with both public health and research training, I will return to working to change those systemic and institutionalized societal structures that maintain health inequity within those communities. So it’s now your time to find your passion and to give back. Pay it forward for every good gesture someone has shown you.
Build relationships with mentors: Since I’ve been involved with organized medicine, I’ve always heard the word “networking”. Too me, it always seemed somewhat a Machiavellian “ends justify the means” insincere word but I guess that’s all up to interpretation. What I prefer to say is focus on finding colleagues with whom you share values and passions, who you respect and would like to emulate, and with whom in the future, you might want to collaborate. If your premise is sincere, opportunities always unexpectedly follow has been my experience.
Step outside your comfort zone: As busy physicians-in-training who are used to structure and consistency, it’s good every once in a while to try something new. You never know what you may find–it may even turn out to be a new passion for you. Life is too short and you want to live it without regrets. You want to say when your time comes that you lived life to the fullest and maybe even tried some things that scared but surprisingly made you happy.
Recharge with some “me” time: All work and no play can make any of us dull and cranky. Set aside time to spend with friends (especially non-physician friends) and family and do non-work related activities. Especially when life is getting you down, some time away from thinking about work may be the recharge you need.
-Betty Chung, DO, MPH, MAis a fourth year resident physician at Rutgers – Robert Wood Johnson University Hospital in New Brunswick, NJ.
ASCP’s 40 under Forty program recognizes forty pathologists, lab professionals, and residents under the age of 40 who are making significant contributions to the fields of Pathology and Laboratory Science. If that sounds like someone you know (or maybe it’s you!) head over the nomination page and start the process. Good luck!