Case history
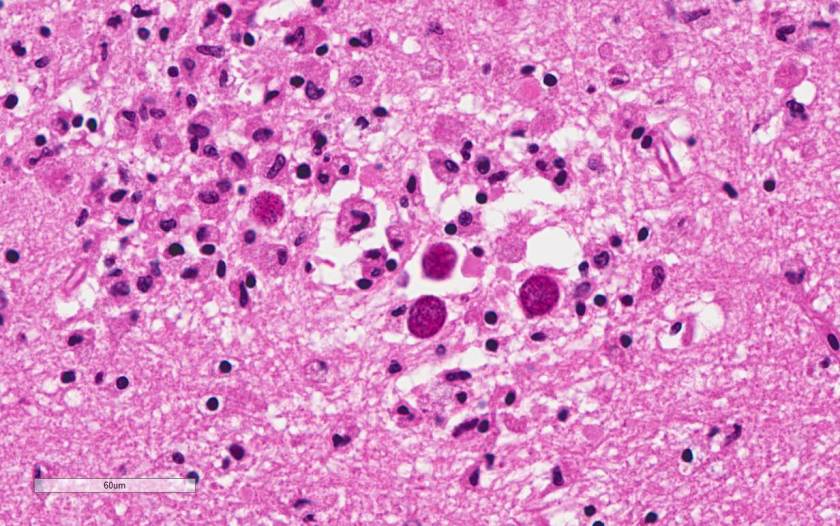
A 47-year old woman with a past medical history of Systemic Lupus Erythematosus (SLE) and liver cirrhosis of unknown etiology was admitted to the hospital for back pain and new onset neurological symptoms. She soon developed pancytopenia and study of her peripheral blood smear showed evidence of thrombotic microangiopathy. ADAMTS-13 inhibitor was negative ruling out thrombotic thrombocytopenic purpura (TTP). She then developed multiple thrombi, including a nonocclusive thrombus in the superior mesenteric vein with extension to the splenic vein as well as a femoral deep vein thrombosis. Her hospital course then became complicated by lupus cerebritis, a small ischemic focus in the left corona radiata and the left medial midbrain, and decompensated liver failure with hepatic encephalopathy. Despite intensive medical treatment, she became hypoxic and hypotensive requiring pressors, and expired in the ICU after several months of hospitalization. The autopsy was performed based on the relative’s request to better understand pathological processes that lead to patient’s demise. The flowing images were obtained from the brain at autopsy (Image 1).
Discussion
Toxoplasmosis is considered to be a leading cause of death attributed to foodborne illness in the United States. More than 60 million men, women, and children in the U.S. carry the Toxoplasma parasite, but very few have symptoms because the immune system usually keeps the parasite from causing illness.
People typically become infected with Toxoplasma by contaminated food or animal-to human routes of transmission. Toxoplasmosis is not passed from person-to-person, except in instances of mother-to-child (congenital) transmission and blood transfusion or organ transplantation.
Persons with compromised immune systems may experience severe symptoms if they are infected with Toxoplasma while immune suppressed. Persons who acquire HIV infection and were not infected previously with Toxoplasma are more likely to develop a severe primary infection. The diagnosis of toxoplasmosis is typically made by serologic testing. A test that measures immunoglobulin G (IgG) is used to determine if a person has been infected. If it is necessary to try to estimate the time of infection, which is of particular importance for pregnant women, a test which measures immunoglobulin M (IgM) is also used along with other tests such as an avidity test. Due to the high rate of falsely positive Toxoplasma IgM testing, the FDA advises physicians testing pregnant women not to rely on the results of any one positive IgM test as the sole determinant for diagnosis of acute Toxoplasma infection.
Diagnosis can be made by direct observation of the parasite in stained tissue sections, cerebrospinal fluid (CSF), or other biopsy material. These techniques are used less frequently because of the difficulty of obtaining these specimens. Molecular techniques that can detect the parasite’s DNA in the amniotic fluid can be useful in cases of possible congenital transmission.
Clinical correlation
The case patient was at risk for developing toxoplasmosis due to SLE disease, and chronic immunosuppressive therapy that she was receiving for the aggressive course of her illness. However, most likely Toxoplasma gondii organisms seen in the brain parenchyma were in a dormant state due to lack of associated inflammation or architectural distortion. Her neurological decline is most likely related to thrombotic microangiopathy. Opportunistic infection is common in patients with SLE. In some patients, it is difficult to distinguish between the effect of infection and exacerbation of SLE because both can produce similar symptoms. There have been many reports of toxoplasmosis in SLE patients, with conditions such as cerebritis and pericarditis mimicking SLE manifestations.
References
1) http://www.cdc.gov/parasites/toxoplasmosis/
2) Seta N, Shimizu T, Nawata M et al. A possible novel mechanism of opportunistic infection in systemic lupus erythematosus, based on a case of toxoplasmic encephalopathy. Rheumatology (Oxford). 2002;41(9):1072-3.
3) Zamir D, Amar M et al. Toxoplasma infection in systemic lupus erythematosus mimicking lupus cerebritis. Mayo Clin Proc. 1999; 74(6):575-8.
Contributors
Written by Anastasia Drobysheva, MD, 2nd year Anatomic and Clinical Pathology resident, UT Southwestern Medical Center
Image provided by Bret Evers, MD, PhD, Neuropathology fellow, UT Southwestern Medical Center

-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
