Welcome back everyone!
Thanks for reading my piece last month on liquid biopsies. And, as a side note, there is a growing number of awesome quality content and posts from pandemic response, to inclusion, alongside COVID and case-studies so subscribe, share, and add this page to your bookmarks—STAT! Lablogatory has been a fantastic platform to share and learn so much in this past year, I could barely keep up!
Or super-STAT if you’re one of those people…but hey, that language belongs to all of us! Lab professionals, nurses, scientists, and doctors alike. And this month, I just want to take a quick moment to celebrate a milestone.
I’m officially a resident physician/trainee, medical post-graduate! (There was confetti falling just now on my end, not sure about yours, but work with me here.) It’s just one of those life-goals that feels great when you get there. But there’s a lot more to it than it seems…if I told you being a pathology resident means sacrificing early adulthood, amassing soul-crushing debt, and explaining to your peers and colleagues what it is exactly you do and why you also bear the moniker of “physician,” you’d delete that bookmarked webpage faster than I can make you scroll through this thing.
(oh good you’re still here!)
All that said, I’ve got to say: it’s worth every single bit of it. Times a million. But I really did mention some red flags that, were we discussing any other work environment, would make you definitely think twice before committing 5-10 years of your life. Furthermore, as a PGY-1 in pathology, I could stand next to any other patient-facing PGY-1 colleague (read: intern) and they wouldn’t have the faintest about what I actually do. Listen, the “lifestyle” specialty, generally 9-5er, no weekend, no 24hr call isn’t something I’m shy to celebrate, but it’s not the whole story. I’ve matched and started learning and working at a great institution with great faculty, mentors, and other residents/fellows. Bottom line: I’m more than a little happy about where I’m at professionally.
So, to my non-pathology friends, what is it exactly that I do during my residency training while you might be busy rounding, managing glucose levels, triaging cases, putting orders in—you know, regular intern stuff *shudders* … (pathology trainees don’t have an intern year, we jump right into the specialty and go for 3-4 straight on through). Like most of you I have a transition period where I get acclimated to the workload and patterns of my specific residency, but sans-anno-interna, I’ve got lots of work ahead to climb the steep learning curve that med school pathology merely skims.
What does non-patient-facing mean, exactly?
Well, without an intern year you jump right into what most path residents go into which is a 4-year combined anatomic and clinical pathology (AP/CP) track. You immediately begin training in all the fields in pathology. They include surgical pathology (of various sub specialties like head-and-neck, gynecologic, gastrointestinal, thoracic, neuro, etc.—think surgery, then add pathology), autopsy training, dermatopathology, cytopathology, hematopathology, transfusion medicine, clinical chemistry, microbiology, hemostasis and coagulopathy, pediatric pathology, forensic pathology, molecular, training as a laboratory director, and much, much more. Each of these services has a workload which is usually comprised of cases from biopsies and grossed specimens for histologic analysis (anatomic pathology) or the ongoing maintenance and advancement of clinical diagnostic testing through laboratory methods and management of staff/resources (clinical pathology).
When I say “non-patient facing” this means that the majority of that work is not done in 1-on-1 settings with patients in a clinic or hospital floor. It is done ancillary to their clinical experience whereby pathology attendings manage the simultaneous training of residents and processing of case sign outs for rapid and accurate diagnostic output for our patient-facing colleagues. For example, while a patient, their family, and doctor are discussing and managing symptoms related to a possible cancer diagnosis. The pathologists are examining microscopic behavior of the cancer-in-question’s cells and adding immunohistochemical testing and molecular analyses to identify, stage, and prognosticate that cancer. Returning information about what it is and what can be done back to the patient-facing clinician, who can then best-translate a tailored approach for their patient. Old-timey medical texts would often refer to the pathologist as the “doctors’ doctor,” and I’m not here to hate on that haha. My clinical friends and readers might feel forlorn now at the prospect of 4 years of medical school training to “just look into a microscope all day?” Well, for some folks in path it means a lot more than that, every slide is a patient. So we care just as much as if they were right opposite our desk. But that’s not all we do…
(More on that in a minute.)
So What Do You Do?
Okay, there are lot of words in path that might act as a barrier to understanding the common ground between me and …let’s say a colleague and friend in Family Medicine. So for the purposes of transparency here’s my friend from medical school Dr. Danash Raja and how a small part of his schedule and my schedule aren’t so different…

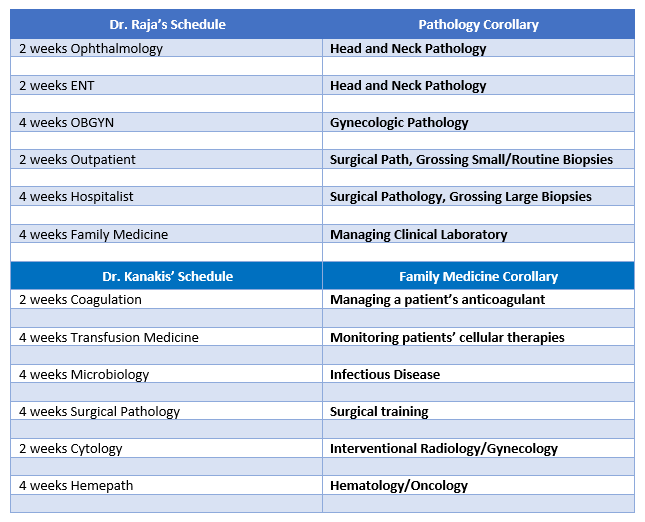
On both sides of this table are clinicians managing their patients and ensuring the best possible outcomes. Both sides are deeply vested in intensive hours of training, procedural experience, evidence-based best-practices from the literature, and ongoing continuing education.

Literally the biggest differences:
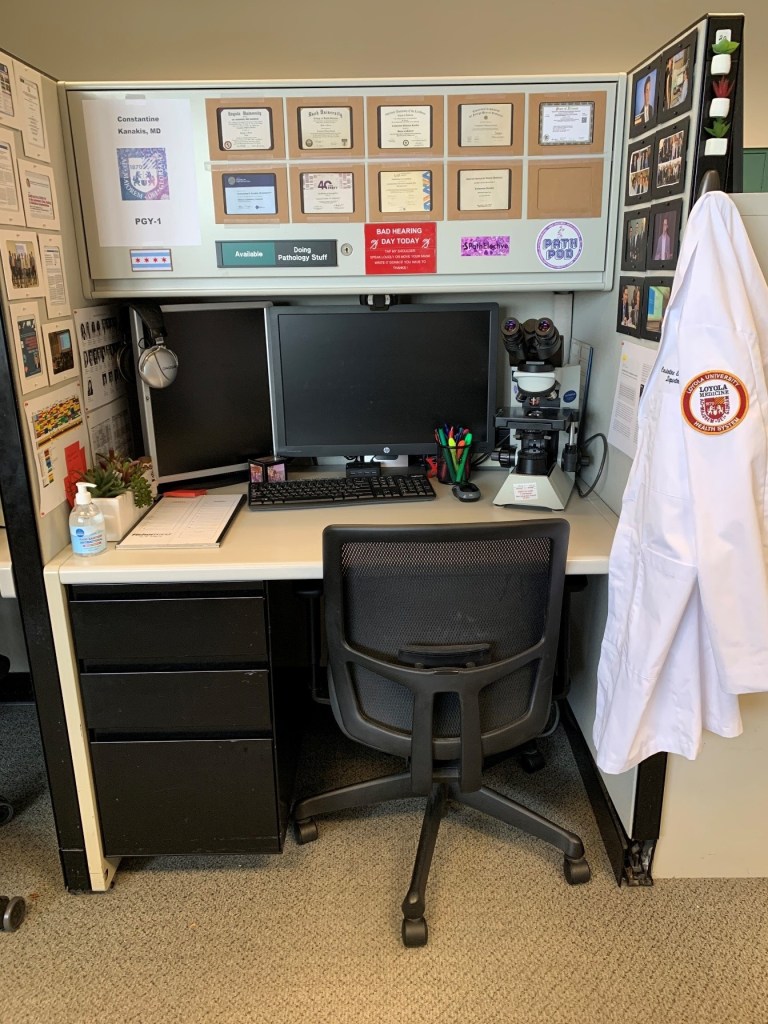
- In pathology, I get my own desk space and I need it! I’ve got to start amassing a physical and digital library to supplement the next 4-6 years of subspecialty training for the eventual day when a colleague will see me in an elevator and expect concise, thorough, and actionable material to inform their clinical management from the pathologic diagnosis.
- Pathology residents and clinical residents both take “call” except Dr. Raja has to pull grueling 24-hour+ shifts and stay in the hospital for the duration, and I answered a page about a transfusion reaction from a grocery store once.
- When a patient thinks about the person who helped them find out what kind of cancer they had and what treatment to begin, they’ll probably think of Dr. Raja or someone patient-facing in Heme/Onc—but I’m working on this, every day!
Bottom line: I’m as important as he is, and he is as important as I am. Our work is what really matters, and what really connects us as clinical colleagues. It’s all about patients, remember? But I’m more than happy to be the pathologist to his patient-facing, diabetes-managing, vaccine-giving, life-improving super hero doctor!
You Never See Patients?
We’re back on this. Remember how I said looking into microscopes isn’t all we do? Okay, well it’s not. And if you’re lucky enough to have matched to as awesome of a place as I did, then you know what I’m talking about. If you’ve read some of my pieces, you know full well my passion in pathology lies in Hematopathology and Transfusion Medicine. I like to sit right on the fence between AP and CP, and mostly look at the green grass on the CP yard. This month, I’ve been on service for Transfusion Medicine and let me tell you about the few weeks…
I, a pathologist trainee, resident physician, under the supervision of two attending physician pathologists have been seeing and following up on patients nearly every day. Gasp! No, I’m not part of some backwards resident exchange program (because OMG how dangerous haha), no I’m not lost, no I’m not being overly gunnery, that’s it, that’s the Tweet. Seriously, it’s just part of the service. Larger academic hospitals with robust clinical blood bank services often have apheresis clinics and I find myself working exactly there. Blood bank/Transfusion Medicine is one of those subspecialties where patient contact is part of the routine. At some institutions, I’ve been a part of some pathology-led teams that procure the bone marrow aspirates from their patients in Hemepath service, or conducted their own fine needle aspirations for cytology service, or dermpath services that operate in clinics alongside their dermatology colleagues—I’ve even been working on frozen sections and surgical path grossing when called into an operating room to discuss methods and approach for biopsy! There were patients at every turn, all with pathologists on the front line! Dr. Syed T. Hoda (@01sth02 on Twitter) from NYU Langone often says, “Person FIRST, doctor SECOND, specialist THIRD.” And trust him, he’s a bone and soft tissue pathologist that left the lab and went to the floors to help clinical staff when overwhelmed during the peak of the COVID crisis in NYC. So for my dual-interests, I would say I’d expect to see quite a bit of patients in my future practice.

So, would I pick pathology again? Uh, yeah! Without a single hesitation. Every day at work I am reminded that I am at the right place, with the right co-residents, the right faculty and mentorship, and the right environment to train and hone my future skills for a career that lines up exactly with what I want to do.If you’re interested about the intersections between clinical medicine and pathology, and want to learn more about “patient-facing pathology” keep an eye out during the 2020 ASCP Annual Meeting for a talk by yours truly as part of a panel discussion on communicating directly with patients! Register now! Free for members.
See you next time!


-Constantine E. Kanakis MD, MSc, MLS (ASCP)CM is a new first year resident physician in the Pathology and Laboratory Medicine Department at Loyola University Medical Center in Chicago with interests in hematopathology, transfusion medicine, bioethics, public health, and graphic medicine. His posts focus on the broader issues important to the practice of clinical laboratory medicine and their applications to global/public health, outreach/education, and advancing medical science. He is actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Watch his TEDx talk entitled “Unrecognizable Medicine” and follow him on Twitter @CEKanakisMD.
