I’ve appreciated some amazing feedback from my previous post discussing how doctors can sometimes be patients too, and the challenges one might face in different roles within our health care system. Not only a challenge of roles, but those that struggle with invisible illness have unique perspectives on patient care.
That said, this month let me take a break from all the fun content found between cases, concepts, and trends in pathology and laboratory medicine, and celebrate our amazingly successful (and virtual) Annual ASCP Meeting!
Image 1. Just look at this virtual lobby! Set aside that in-person connectivity dissapointment and just appreciate the quality put into this visually! More of my oggling to come in further images…
It was awesome. But don’t just take my word for it, we’re all people of science here, right? So let’s do it by the numbers!
133 educational sessions
3 general sessions
4 named lectures
36 round table sessions which included topics like wellness, problem-solving, collaborative solutions, and “birds of a feather” breakout discussions
9 virtual video microscopy sessions
8 session dedicated to laboratory professionals covering hematology, chemistry, microbiology, and blood banking
6 resident board review sessions
15 companion society sessions
14 sessions related to wellness
4 sessions discussing diversity and inclusion
10 COVID-focused sessions
20 grant funded sessions
4 virtual patient symposia (more on this topic below…) and
And 300+ posters!
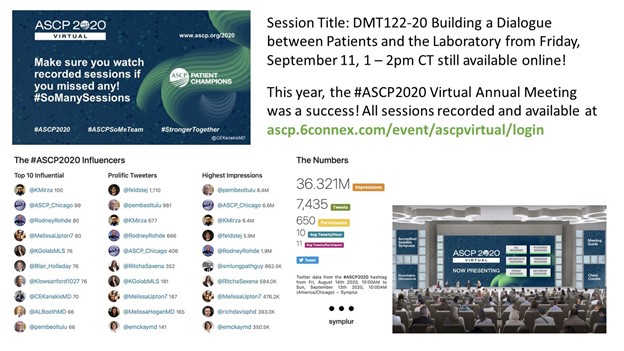
Image 2. More visual appreciation here: virtual sessions felt like you were really in a large, collective meeting of enthusiastic, like-minded laboratory professionals all learning, collaborating, and networking together!Image 3. I was fortunate enough to to speak on this amazing panel regarding direct patient-and-pathologist interactions, making laboratory medicine and the overal healthcare experience, safer, more accessible, more interdisciplinary, and better equiped at dealing with the forefront of medical diagnostics!Image 4. So, the session went well! Just look at that social media data: 36 million impressions over 3.5 days! That’s 1 million people engaging ASCP topics a day, or 12 people per second! All actively discussing and collaborating topics in pathology and laboratory medicine.Image 5. How could I (of all people) ignore the fact that #ASCP2020 featured an amazing social (media) lounge where people from all over could connect, chat, network, and relax! There were interactive, virtual sessions covering all kinds of non-lab med stuff: yoga, meditation, mixology, and cooking! I hope this is a permanent addition to future (hopefully) hybrid in-person/virtual meetings.
What more could you ask for? The folks that run the logistics and planning for the ASCP Annual Meeting outdid themselves again. Sure this content would excite anyone in the field for 3 dedicated days of immersive learning and networking, but all this and more are still available online for virtual on-demand recorded viewing! Missed a session? No worries, it’s still waiting for you for about 6 months (through March of 2021). All the buzz aside from ASCP members having free access to all of this content, the excitement started months before the meeting went live. Estimates are still coming in, but membership grew by a couple hundred in the weeks leading up to the meeting—not surprising: free access for members? That was an excellent deal, so choice.
Image 6. The start of the #ASCPSoMeTeam’s amazing trajectory culminated at #ASCP2019 in Arizona, the more we work together the more we can accomplish for our profession and our patients, #StrongerTogether.Image 7. ASCP’s Resident & Pathologist Councils are invaluable assets to promoting and advancing all of our professional development. #ASCP2020 was no different! From virtual fellowship fairs to online, interactive resident council sessions, there was a lot to take it—still available online!Image 8. I’ve talked about previous ASCP Annual Meetings here and here, and while I can’t list every single aspect of what made this meeting (virtually) amazing, members can check in for about 6 months and see for themselves the quality and attention to detail that comes directly from our collective passion to make pathology and laboratory medicine better, for everyone. Kudos to the ASCP leadership and logistics teams that made this all possible!
Great to see you all at the meeting!
Thanks for reading! See you next time!
-Constantine E. Kanakis MD, MSc, MLS (ASCP)CM is a new first year resident physician in the Pathology and Laboratory Medicine Department at Loyola University Medical Center in Chicago with interests in hematopathology, transfusion medicine, bioethics, public health, and graphic medicine. His posts focus on the broader issues important to the practice of clinical laboratory medicine and their applications to global/public health, outreach/education, and advancing medical science. He is actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Watch his TEDx talk entitled “Unrecognizable Medicine” and follow him on Twitter @CEKanakisMD.
Are you interested in presenting an education course at ASCP’s 2016 Annual Meeting? If so, the call for proposals is now out. You can find it at the direct link below.
ASCP’s 2016 Annual Meeting will be held at the Mandalay Bay Hotel & Casino in Las Vegas, NV on September 14-16, 2016.
ASCP and ASC have put together a program to enable cytotechnologists to grow their skills and advance their careers. During this workshop, attendees will learn how to engage as a part of the clinical team and broaden their skill set to include fluorescent in-situ hybridization and interpretation of applied molecular tests.
The Clinical and Laboratory Standards Institute (CLSI) and the Association of Public Health Laboratories (APHL) will co-host the 12th annual educational update webinars for antimicrobial susceptibility testing (AST).
Each January, CLSI updates standards for AST. It is important for clinical laboratories to incorporate the new recommendations into routine practice to optimize detection and reporting of antimicrobial resistance. In January 2015, the annual update of the M100 AST tables (CLSI document M100-S25) was published. In addition, the standards that describe performance of disk diffusion and minimal inhibitory concentration tests in versions M02-A12 and M07-A10, respectively, were updated. Some highlights for 2015 include introduction of the Carba NP test for carbapenemases and expanded recommendations for quality control testing.
These changes and several other new recommendations found in M100-S25, M02-A12, and M07-A10 will be discussed during the webinar. In addition to the webinar, an optional postprogram self-assessment will be provided that will allow individuals to assess their knowledge regarding the most important AST and reporting issues for 2015. Laboratories can use this feature to augment competency assessment requirements for their staff.
The webinar will be led by Janet A. Hindler, MCLS, MT(ASCP), Senior Specialist, Clinical Microbiology, at the UCLA Health System in Los Angeles, California, USA.
Webinar information is as follows:
CLSI 2015 AST Update
February 4, 2015 • 1:00–2:30 PM Eastern (US) Time
February 5, 2015 • 3:00–4:30 PM Eastern (US) Time (repeat session)
Learner Level: This intermediate-level program is appropriate for laboratory professionals working in clinical and academic settings.
At the conclusion of this program, participants will be able to:
Identify the major changes found in the new CLSI document M100-S25.
Design a strategy for implementing the new practice guidelines into their laboratory practices.
Develop a communication strategy for informing clinical staff of significant AST and reporting changes.
ASCP 2014 at Tampa provided the perfect getaway for a New Yorker forced to wear fleece early October. The same attire seemed to be mocking me the moment I stepped out of the Tampa International Airport on Wednesday night. It was a pleasant surprise and I gleefully tucked it right into my suitcase.
At the hotel, I took a quick glance at the lecture schedule. Having already missed the first day, I was eager to extract the best out of the next two days. I was thrilled to see an array of topics specially aimed at residents. Also, many lectures focusing on novel or state-of-the-art techniques, including molecular methods, virtual microscopy, digital pathology, informatics, etc. It seemed to me like “The future beckons!!” Being a hard-core morphologist, it was a tough call for me, as I would have to forego a host of other good lectures. But I decided to focus on the resident review courses and ancillary techniques.
Keeping with my agenda, I set the ball rolling on day two by attending the lecture on “Automating Anatomic Pathology.” It was an eye opener for me, dealing with the scope and future of automation in anatomic pathology lab. “Anatomic Pathologist’s Role in Patient Safety” was the next. Dr. Silverman cited studies revealing that soft tissue lesions, with an error rate of 20-30%, led the list of organ specific error rates. He deliberated on the importance of second opinions in error reduction. He aptly concluded his lecture with the remark, “the pathologist is the Final Quality Assurance Officer or ‘the buck stops here.’” It was a huge wake up call for me.
I moved on to my first lecture on Molecular Pathology, “Welcome to the Beginning: Molecular Pathology for the General Pathologist and Molecular Pathologist.” It was just the right one for me and helped me firm up basic concepts. In the evening I attended “Molecular Diagnostic Methods in Oncology: an update on practical aspects.” Dr. Larissa Furtado and Dr. Yue Wang from University of Chicago were simply brilliant in elucidating the role of molecular techniques in oncologic practice. The prior morning session, helped me understand the deliberations in this talk much better.
I made it a point to attend most of the Resident Review courses. Though my Board Exams are two years away, I took it as a perfect platform to acquaint myself with the “hot” topics. I spent almost the entirety of day three attending the courses. A packed audience was testimony to these sessions’ popularity. Most of the speakers were brilliant. The case based presentations followed by an interactive voting format helped keep us all fully involved. However, the lab administration and last day hematology section could have been better.
In between, I found some time to listen to one of my all time favorites: Dr. Goldblum’s trademark lecture on soft tissue pathology. He quipped in his inimitable style “Don’t hunt for lipoblasts to diagnose a liposarcoma” and warned us of the vast plethora of “pseudolipoblasts” lurking around. Rather, he stressed the importance of analyzing the entire histology in the correct clinical context.
Let’s wander into the poster sessions! We had a total of twelve posters from our program itself, probably the largest representation from a single center. I had four posters and one of them was selected as a finalist in the Best Resident Poster section. It was an entirely new experience for me. However, I did some homework to prepare myself for the judging session. The judges on both the days were very pleasant and spent a significant amount of time discussing the work with me. It was disappointing not to get the award, though I knew the competition was tough.
The evening Mixology Lab was the perfect concluding session in the backdrop of the setting sun across the scenic Hillsborough river. There was delicious food and wine as Dr. Baloch announced the various poster award winners. It was special for me for another reason, as my very good friend Shree Sharma was one of the “top 5 under 40” award winners.
Mixology Lab attendees soaking up the sun
It would be so improper if there were all work and no play. Friday evening provided the perfect opportunity to explore the city. I went out with friends to the Ybor City, taking the streetcars, which surprisingly provided 50% discount to conference attendees. Ybor City was such a happening place, full of fun. While strolling along the 7th avenue, we took pictures with people celebrating Gasparilla festival, dressed as pirates. A glass of sangria at the historic Columbia Restaurant provided the perfect toast to end the day.
My trip was not to end here as I had already registered for the TRIG Genomic Pathology Workshop for Saturday. This was my first exposure to such a session in molecular technology. We were divided into small groups. In a case based approach, the workshop deliberated on teaching principles related to the development of genomic assays and result interpretation. There were four cases pertaining to single gene testing, prognostic gene panel testing, how to design a cancer gene panel and whole genome sequencing, respectively. Both Richard Haspel and Andrew Beck were simply brilliant and they took special care to approach each group separately and clarify their doubts. It was a highly stimulating experience for me and I learned a whole new facet of pathology. The utilization of online genomic pathology tools for result interpretation appealed to me. It also gave me the opportunity to work with fellow residents from other programs in a very close and interactive manner. Though the warm sun outside beckoned, I believe this was the perfect finale for three full days of extensive learning activities.
A trip to Tampa would be incomplete without a visit to the Florida Aquarium. I took a relaxed tour of the aquarium after the workshop, visiting the lovely marine friends. When I boarded the flight back to New York on Sunday afternoon, I felt very content. It was also reassuring to see that ASCP indeed cares about resident education and needs. The meeting opened my eyes towards the new horizons in pathology and how many options lie before us for shaping our careers.
-Rifat Mannan, MD is a second year Pathology resident at Mt Sinai St.-Luke’s Roosevelt Hospital Center, New York.
Instead of having to deal with the sub-zero cold weather in Chicago (where my car doors froze earlier in the week and I had to tug on them for over half an hour to get into the backseat of my car to turn on the heat), I was fortunate last weekend to be in the sunny and warm wine countryof Temecula (near San Diego). I was there for a CAP Council on Education meeting where I served as their junior (resident) member. Due to confidentiality agreements, I can’t divulge specific details, but it did get me to thinking about what “true competency” means and what we need to do to obtain and maintain it after we graduate.
Residency is a transition for many (especially if you didn’t take time off to work before continuing your higher education) between two different mentalities: that of school versus employment. Ideally, there shouldn’t be a large difference between how we approach school and our job but that’s not always how it goes. In medical school, if we didn’t continually study, it was just our grade that would suffer and we could study harder for the next test to average out to a decent grade. But with residency, which is now my job, when I don’t apply myself to learn everyday (and I can’t say that I’ve perfected this yet but I keep trying), it’s really my patients, and possibly future patients, who suffer the consequences.
Pathology is the “end game.” We are the regulator of most diagnostics (both on the CP and AP sides) that other physicians use to make treatment and prognostic decisions.And so, we need to train now and develop a trainee culture that nurtures life-long learning (and truly mean more than just lip-service). We need to allow residents to participate in true “practice-based” learning (not just passive learning) and to feel the punitive consequences if we ignore our responsibilities or are incompetent. I believe in second, and even third, chances. I believe that our residency programs should remediate residents who are not where they should be in a non-threatening manner. But I do also believe that there is a minimum bar that we all need to meet within a specified time frame.
I believe that we need to be good representatives of our respective programs as graduates, and more importantly, “competent” pathologists who do not hurt our patients due to lack of important knowledge that we should possess – and of course, it’d be nice not to have to worry about malpractice issues as well. Developing this mentality starts during residency – where we should study a little everyday in order to perform as much as we can– and where we can take feedback from our attendings and work to improve our areas of deficiency while we have them around to guide us.
Some pathologists on forums that I’ve visited decry maintenance of certification (MOC) and the continuing medical education (CME) and/or self-assessment modules (SAM) as money-making measures for the organizations who put together CME/SAM material. This weekend, I learned what these and many other acronyms mean. I can see their point since it often costs money to obtain CME/SAM; also, physicians do not want to think of having to take tests once they graduate med school. However, I do think that in a rapidly changing field such as pathology, not being up-to-date may have detrimental effects on patient care, so CME/SAM are necessary. We can’t always expect that everyone in our profession will be motivated to be up-to-date without some sort of “carrot stick.” It’s sad but true. So my main point, fellow residents, is that we should develop good habits now that encourage life-long learning and an attitude that shows that we put our patients first…and we’ll probably find that without even realizing it, we have worked toward gaining competency in our profession. So what do you think about the need for CME/SAM and MOC every 10 years? There’s no “grandfathering in” for any of us, so we will have to deal with this. But do you think that this is the way to go to help our maintain competency once we’ve achieved it?
–Betty Chung, DO, MPH, MAis a second year resident physician at the University of Illinois Hospital and Health Sciences System in Chicago, IL.
I wanted to devote this blog to my experience at the recent Training Residents in Genomics (TRIG) one-day workshop at the ASCP Annual Meeting in Chicago. I admit that I am biased since I had ten years molecular and cell biology and transgenics research experience prior to medical school and enjoy all things molecular. But I really I do think that TRIG is an idea whose time has come.
TRIG is a group of molecular pathologists, medical educators, and geneticists who came together in 2010 with the goal to create a standardized, high quality genomics curriculum and to promote adoption at >90% of pathology residency programs by the end of their 5-year grant period. A 2010 survey of 42 pathology residency program directors found that only 93% confirmed molecular pathology as a part of their training and only 31% had established curricula on relevant topics. So, TRIG plans to provide online resources, lectures and workshops, and to assess the efficacy of genomic medicine curricula at residency programs through RISE performance. From speaking to other residents I’ve met over the past year, I know that the teaching of molecular pathology at each program can vary significantly.
The TRIG workshop had four sessions that followed the case of a woman with newly diagnosed breast cancer while applying specific hands-on skills related to the genomic related elements of her case. I missed the first session so I can’t say too much except that they discussed single gene testing and assessment of BRCA mutations of unknown clinical significance. Session two covered the assessment of prognostic gene panels (Oncotype DX) and compared them versus the standard breast IHC panel. We also learned to plot Kaplan-Meier survival curves based on a patient’s genomic profile on a publicly available website.
After lunch, session three dealt with the selection of genes to design a breast cancer multi-gene assay for this patient. Questions considered were the availability of targeted drug therapy for specific somatic mutations, the strength of association of selected genes with breast cancer, frequency of these variants, reimbursement, and choice of PCR based genotyping versus next-gen sequencing. The final session focused on the creation of a genomic pathology report for this patient after analyzing the clinical significance of each result from multi-gene mutational analysis using free web-based tools.
This workshop was a great introduction for the genomics neophyte (especially if one’s residency is weak in this subject or doesn’t have a molecular pathology rotation) and even someone with some experience like myself, learned how to use some new tools and applications even though the concepts were not new to me. As I mentioned in previous blogs, I learn more from having to tackle issues hands-on and being able to participate in a bidirectional discussion about a topic versus reading textbooks or attending lectures. The workshop was a good intro albeit too short to learn to apply these skills comfortably and effectively…but it is definitely a step in the right direction and I expect to see more great things coming out of the TRIG Working Group. More info about TRIG is at www.ascp.org/trig.