Hello again everyone, and welcome back!
Last time we talked a bit about what exactly pathology and laboratory medicine training looks like—a much-needed peek behind the curtain, if you ask me. This time, I’d like to discuss something that’s been challenging me way before I started working as a resident: something that’s made both clinical medicine and academic collaboration difficult (to say the least). I talk a lot about how medicine works best when we all come together and contribute our expertise from disciplines across the board for the sake of improving patient care; I even talk about how, too often, people don’t hear the messages coming through from their colleagues and that negatively impacts our field. We’re all guilty of it, some more than others. And in the last few weeks, I’ve been nearly deaf to my colleagues.
No literally, this article is about my Meniere’s disease and how those of us with invisible illness(es) can really impact the collaborative spirit of medical science. Trigger warning: frustration, anxiety, and pathology (mine, specifically). So here’s a reminder that everyone you meet and work alongside has issues they’re dealing or struggling with. And, to those outside of medicine, remember doctors are people too. Dr. Jena Martin, a dermatopathologist I admire and follow on social media recently promoted the topic #DoctorsArePatientsToo—she writes, shares, and promotes fantastic topics on social media and I suggest you check her content out at @jenamartinmd.
So, I’ve got a couple things to explain here. Come with me on a journey through the inner ear and out into the reaches of global pandemics!
An MD with MD
So what is Meniere’s disease (MD) and why does it deserve its own article? Well, first of all, it doesn’t deserve anything, it’s a garbage disorder with dumb symptoms and I’m only using it/myself as an example to highlight the struggle for other people working in medicine who also deal with invisible problems. But, since you asked…
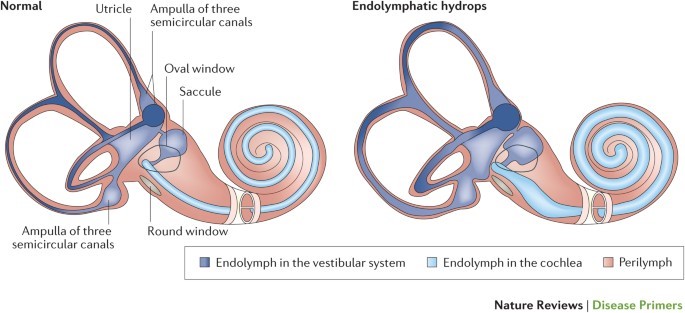
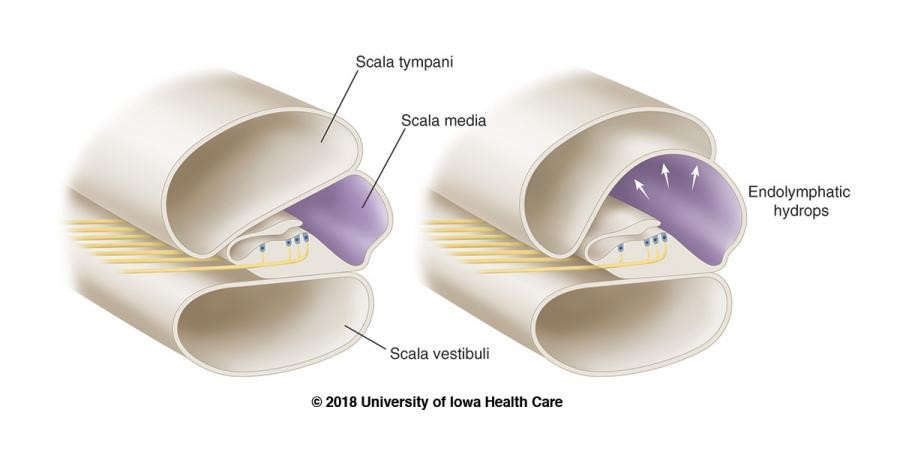
Without belaboring any detail, Meniere’s is a somewhat understood inner ear disorder in which the potassium-rich, sound-signal inducing endolymphatic fluid builds up in the inner ear. This causes the organ of Corti (Image 2b) to swell up, along with the rest of the cochlea, the vestibule, and the fluid containing parts of the inner ear (Image 2a). The super pressurized vestibular-cochlear balloon is in a confined bone-space so what happens often is that small fistulas form, mixing the endo and perilymphatic fluids causing all sorts of problems not limited to but including: aural fullness, deafness, ridiculous multi-tonal/pulsatile tinnitus, distorted hearing, frequency loss, imbalance, severe peripheral/rotational vertigo lasting for hours, occasional tachycardia, anxiety, and more! There is no cure; therapy is symptom-dependent and purely aimed at management and mitigation of fulminant hearing loss. Did I mention that most times it’s one-sided, but mine is bilateral? Fun. I’ll be donating my ears to science and/or the garbage in some odd decades from now…
Let me put it this way: Over time, I will lose a stark majority of my natural hearing. I will continue to get occasional vertigo attacks, and related symptoms, until the disease (eventually…hopefully?) “burns out” and has no more capacity to damage any more already-damaged inner ear hair cells. I’ll probably get hearing aids or cochlear implants. (Whatever, I’ve always wanted to be half bionic…) I’ll probably keep a cane with me most times. (Dr. House anyone? Right? Or I could keep a sword in there? Legal issues?) But it’s not the long term that bothers me most. It’s the flare-ups. This disorder has periods of acute attacks, periods of mixed-symptom flare ups, and periods of remission. I can handle the remissions, hah. I can even handle the acute episodes—I’ve had great ENT colleagues and discovered great medication plans to manage the attacks. So that leaves the flares, which inspire writings like this one obviously. I wear my hearing aid, but it’s minimally helpful, and I practice patience until my hearing returns. But that isn’t as easy as it sounds, especially when you’re a working resident MD!
The Sound of Silence
Technically, I haven’t experienced true silence since 2015. And, during flare-ups, most of my hearing is almost entirely replaced by the only sound my ears can accommodate and attenuate for which is their own local vasculature. If Edgar Allan Poe could see me know…telltale ears, anyone? Let me paint a picture of what I’m hearing right now on a pretty rough flare-up day, at work, at my desk in the resident room. I’m drinking tea, I can’t hear myself swallowing. I monitor my heartrate on my watch and it’s about 80-90 beats per minute, in my ear, all day, whoosh-whoosh. The pot of tea the robots have been making, whistles non-stop, 24/7. The mosquitoes I’ve been writing about for years now on Lablogatory never leave my cochlea. Cool, on top of that I’ve got hearing loss and aural fullness that makes me not able to hear low-volume pages/phone rings (vibrate mode FTW) and most talking—especially behind masks. (I’ll get to that in a second.) If I turn my hearing aid too high, there’s a squeaky feedback explosion, not to mention the occasional adjustments for quiet and/or super loud talkers, yikes. Just overall, me no hear too good right now. Basically if hearing was reading text, the printer is out of toner and the paper is provolone cheese. And the cheese is on fire. Opa!

Global Pandemic? Sounds Pretty Bad…
The SARS-CoV-2 pandemic has created very interesting situations at work and elsewhere, all over the globe. People are utilizing the most effective measure against spreading the illness: which up to this point is the non-pharmaceutical intervention of social distancing. Nearly every single person working today, in any field, doing anything, reading this blog, has been a part of email chains, and conference calls, and …. sigh… Zoom meetings. I know, I know… there are pro’s and con’s to this but consider these three points for those with #InvisibleIlnesses:
- Working from home has liberated chronically ill folks
Okay so I have an intermittent vestibular/cochlear disorder. What about folks with chronic pain, or Lyme-sequelae, or brain fog, or any other host of hurdles before they can jump onto a video call. Pretend you’re sick at home with a (non-COVID) viral bug. Can you imagine how nice it would feel to have hot tea, your medications, your cat, your spouse, and (most importantly) your couch/bed/TV nearby? Within reason, you’ve just given people who would have needed to excuse themselves a way to participate productively!
2. Imagine having a supplementary PowerPoint or chat box during conversations IRL
One of my specific challenges is missing a word here, a sentence there, and not being able to catch up in a conversation. Usually it ends up with my smile-nodding through to the next topic or checkpoint, but in the current age of virtual meetings I can un-obtrusively ask “What was that last bit?” without seeming like I tuned out. And bonus: I can often get a text translation of a point or two I might have missed from keen colleagues aware of my AV troubles. I can only imagine what it would be like for those more permanently affected.
3. The explosion of inclusivity and accessibility is remarkable
Speaking of which, the number of videos and presentations I am now seeing with closed captions/text supplements are astounding. Usually when I’m in the midst of a flare, I have to check out from audiovisual stimuli and stick to reading only. This can be quite the challenge for work sometimes. But with chat boxes and videos with captions, I feel like I can catch right up. Now, I said I’m only like this part of the time, so for those that have felt excluded and marginalized I’m happy to say that inclusivity and accessibility are growing. I’ve often thought that the importance of a news story or press conference could be measured by the presence or absence of a sign-language interpreter. Over 100 press conferences by Governor Andrew Cuomo in NY, or in Chicago, Illinois with Governor JB Pritzker and Mayor Lori Lightfoot, and each of them was accompanied by ASL accessibility. Fantastic! Just look at one of many efforts online, like @ProjectHearing on Instagram, which promotes the advancement of these topics every day!

Your Lips Move but I Can’t Hear What You’re Saying
So why, when the world is literally aflame with a viral pandemic, am I drudging you through my rant against my inner ears? And why did I just commit the travesty of endorsing zoom calls and captions (I know some people hate captions—you came for a movie not a book, I get it).
Well this whole topic illustrates to big things about working both as a physician and as a person with an invisible condition. First, like most things in medicine, to achieve success you have to adapt, improvise, and overcome. Solving patients’ problems and advocating for their best outcomes takes a little finessing of the system sometimes, you’ve got to do the same thing for yourself. Second, since doctors are patients too, its okay to ask for help. I matched with some of the best residents I’ve ever met, and they’ve offered whatever they can in helping manage my flares during work. This includes anything from extra emails/group text notification chains, forwarding pages, translating video call jumbled audio, etc. They are the best!
Meniere’s has been a challenge to me for a couple of years now, and it’s something I deal with. We’ll call it a character-building attribute. But I genuinely did worry about how this was going to affect me during residency—I had my fair share of hard days in med school basic sciences, and plenty of attending wave-offs when I simply couldn’t hear on 4:00am rounds (yeah I’m looking at you OBGYN and Surgery…). But, it’s been good.

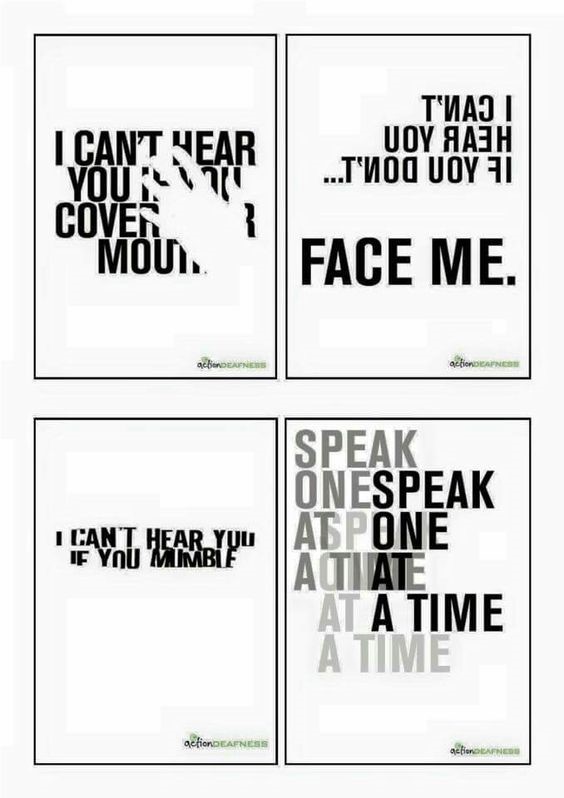
And more than just good, another resident actually has a more permanent hearing impairment and two desks over from mine are the embedded hearing interpreters provided by the department. They’ve been so friendly and provided my with so many resources that I couldn’t be more appreciative. Not only do I have another resident to confide hearing-related rants to, but I also have a department that cares enough to create a supportive and accessible environment. One of the best things they’ve provided: MASKS WITH WINDOWS! Because since this damn pandemic started, I can’t read lips anymore! I didn’t realize how much I depended on visual lip-reads to confirm my hearing that it’s been a learning curve to say the least. Imagine being mostly deaf, your hearing aid not helping much, and looking into a multi-headed scope while your attending lectures on what you’re looking at. An otherwise impossible situation, but my friends and colleagues find ways to make it work because when one person excels, we all do. I’ve been able to continue working, learning, and collaborating thanks to considerations for invisible illnesses like mine.
Consider your colleagues, what can you do to make sure they feel that their needs are met since #DoctorsArePatientsToo? See you next time!

-Constantine E. Kanakis MD, MSc, MLS (ASCP)CM is a new first year resident physician in the Pathology and Laboratory Medicine Department at Loyola University Medical Center in Chicago with interests in hematopathology, transfusion medicine, bioethics, public health, and graphic medicine. His posts focus on the broader issues important to the practice of clinical laboratory medicine and their applications to global/public health, outreach/education, and advancing medical science. He is actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Watch his TEDx talk entitled “Unrecognizable Medicine” and follow him on Twitter @CEKanakisMD.

You’re amazing…
THANK YOU SO MUCH FOR THIS ARTICLE! I am a general practitioner and recently (one month) been diagnosed with Menniere’s. My biggest problem at this stage is the unpredictable nature of the vertigo attacks! I have a waiting room full of patients and -suddenly- I’m “man down”!! You get behind with your appointments, people start to grumble… but you cannot get up from … well whatever is closest to you: the floor, examination bed … and sometimes the toilet (the nausea and vomiting… ugg) I also struggle to use my stethoscope with my hearing aids. I can’t find a good support group/organisation in South Africa so I am grateful for your post! I’m looking all over for practical ways medical doctors handle this syndrome. Thank you! Don’t feel so isolated anymore! 🙂