In the world of clinical laboratories, we often focus on metrics, SOPs, and compliance checklists to reduce errors. But as any seasoned laboratorian or quality professional knows, mistakes still happen—sometimes even when all the systems are in place. Why? Because at the center of every lab process is a human being. And humans, for all their training and dedication, are not robots. (Even though it seems admin sometimes thinks we are.)
As a regulatory affairs manager and laboratorian with a background in psychology, I’ve spent years navigating the intersection between compliance and cognition. Understanding how people think, react, and sometimes err has helped me see lab operations through a different lens. In this post, I want to explore the concept of human factors and how they play a role in lab errors—not to assign blame but to foster a culture of safety, empathy, and improvement.
The Cognitive Load We Carry
Laboratorians are tasked with high-stakes responsibilities: matching blood types, identifying critical values, and interpreting complex diagnostic results. Add in interruptions, multitasking, and staffing shortages, and the mental bandwidth gets stretched thin.
Cognitive overload can lead to slips and lapses. A mislabeled specimen, for example, might result not from negligence but from working memory overload.1 When we acknowledge this, we can begin to design systems that support mental function instead of taxing it.
The Role of Confirmation Bias
Confirmation bias—the tendency to favor information confirming our beliefs—can creep into lab work. If a pathologist or a technologist “expects” to see a result or a specific pattern, they may inadvertently interpret ambiguous data to match their expectation.2,3 This is not a character flaw but a function of how our brains process information. Peer review, second reads, and built-in verification steps can guard against this type of error.
Fatigue, Stress, and Emotional Load
We often underestimate the impact of emotional and physical fatigue on performance. Long shifts, personal stressors, or the emotional toll of working in healthcare environments can impair judgment and focus.4,5
Labs prioritizing wellness—through break policies, mental health support, or manageable scheduling—not only show compassion but can contribute to improved performance and fewer mistakes.
Designing with Humans in Mind
So, how can labs address human factors without compromising accountability? Start by shifting the narrative. Instead of asking, “Who made the mistake?” ask, “What in the system allowed this to happen?” 6 (As a side note, this is the true purpose of a root cause analysis.)
Incorporate human factors thinking into root cause analysis. Provide human-centric training that acknowledges common cognitive pitfalls. And most importantly, build a culture where speaking up about near misses is welcomed, not punished.
Last Thought
Human error isn’t a moral failing; it’s a predictable part of being human. When labs take a psychologically informed approach to error prevention, they open the door to safer practices, stronger teams, and more resilient systems.
Understanding human factors doesn’t weaken quality systems—it strengthens them. And perhaps more importantly, it reminds us that the people behind the results matter just as much as the results themselves.
References:
Reason, J. (1990). Human Error. Cambridge University Press.
Nickerson, R. S. (1998). Confirmation bias: A ubiquitous phenomenon in many guises. Review of General Psychology, 2(2), 175-220.
Lockley, S. W., et al. (2007). Effects of health care provider work hours and sleep deprivation on safety and performance. The Joint Commission Journal on Quality and Patient Safety, 33(11 Suppl), 7-18.
West, C. P., et al. (2009). Association of resident fatigue and distress with perceived medical errors. JAMA, 302(12), 1294-1300.
Dekker, S. (2014). The Field Guide to Understanding ‘Human Error’. Ashgate Publishing.
-Darryl Elzie, PsyD, MHA, MLS(ASCP)CM, CQA(ASQ), is the Regulatory Affairs Manager Inova Blood Donor Services. He has been an ASCP Medical Laboratory Scientist for over 25 years, performing CAP inspections for two decades. He has held the roles of laboratory generalist, chemistry senior technologist, and quality consultant. He has a Master’s in Healthcare Administration from Ashford University, a Doctorate of Psychology from The University of the Rockies, and is a Certified Quality Auditor (ASQ). Inova Blood Donor Services is the largest hospital-based blood center in the nation. Dr. Elzie is also a Counselor and Life Coach at issueslifecoaching.com.
When you think of the “glass ceiling,” you typically think of your career, right? I know I thought purely of professional development when I heard that term thrown around. I’m a huge proponent of breaking said glass ceiling in yourself, your team, your organization, your specialty, and the entire field of laboratory medicine. There’s continuing education through our professional societies and ideally through our institutions, and there are advanced degrees, certificates, and on-the-job training. So many tools and resources we can add to our professional toolbox to exceed all expectations, including those we hold over ourselves. But what about the personal glass ceiling? In order to excel in our careers, we have to first excel in ourselves. Let that sink in. I hear other lab professionals say, “I want to be a leader, too, someday.” I promise you, especially as I’ve learned over the past 3 years in an official leadership role, a leader is not shaped without ongoing personal development and the constant challenging of your personal glass ceiling.
New people-leaders in my health system are required to undergo extensive training through our Leadership and Organizational Development (LOD) team. To be quite frank, I silently scoffed at the idea of having to attend “so many virtual and in-person trainings that interfere with my workday. I mean, my dissertation focused on laboratory leadership and change management, come on!” I’ll be the first to admit that I was so wrong. It also helped that there were three other laboratory leaders present with me, so we were able to role play and come up with solutions to issues in real-time. There were DEI trainings, such as civil treatment and inclusive workforce; communication models, including coaching, delegation, and two of my personal favorites – Management Foundations and Emotional Intelligence (EQ).
In the first day of Management Foundations (and yes, after my thinking, “How can I get out of this and prepare for our upcoming lab inspection instead?”), we were given tools to explore ourselves. Initially, I thought we would be completing the Myers-Briggs Type Indicator and explore our personalities. I’m in my seat waiting to share how I’m an INFJ, the Advocate, and how I have (sometimes) unrealistic high expectations for myself and others. This wasn’t a personality test though. What we were about to embark on was a behavior test, also known as the DiSC Assessment. We were told to choose 4 color-coded cards with adjectives that we thought described ourselves. I chose “high standards,” “diplomatic,” “analytical,” and “enthusiastic.” I chuckled when I saw a fellow lab supervisor also grab “high standards” to describe herself as I know how Type A we both are. After going through the formal assessment, I learned that my dominant behavior was “Conscientiousness” with a secondary behavior of “Influence.” As a “C” behavior type, I’m described as enjoying working with people who are organized and have high standards, carefully weighing pros and cons, and preferring environments with clearly defined expectations. Nailed it! This assessment teaches you how to communicate and work with different behaviors and how those other behaviors react to pressure. It is also important to take note of your secondary behavior as sometimes that can become the dominant behavior under stress. This activity was so enlightening that I returned to the lab the following day and asked my team complete the assessment as well. Not only has this given me an insight into my own behavior, but now I’m better prepared to help the individuals on my team thrive and communicate under different levels of pressure on a personalized level. Take note that your behavior preference also impacts how you receive feedback and communicate upward as well and giving this assessment to those either lateral to or above you in the organizational hierarchy can also yield incredibly useful results. Insight gained from this tool crosses so many boundaries, and if others are open to it, they can actually use the results to improve their awareness and regulation.
Speaking of, during our EQ training, we dove into 4 components of EQ – self-awareness, self-regulation, social awareness, and relationship management. For self-awareness, we’re encouraged to be curious and name our emotions (name it to tame it), dig for reasons behind that reaction, search for patterns or triggers to this emotion, and then lean into the discomfort of that to experience growth. In self-regulation, we were asked to breathe using the 4-7-8 method and practice grounding exercises. Essentially, you want to catch yourself when your brain is going offline and not react until you can engage the prefrontal cortex in a healthy and productive (professional) way. You also have to commit to the practice of self-awareness and self-regulation, making it a habit so that you can hold yourself accountable and build trust both within yourself and across your team.
When it comes to social awareness, take time to read the room. Look at body language and recognize if others have the time or space for the information or energy you are bringing, and put yourself in the other person’s shoes. For relationship management, it’s important be open and listen without judgement or assumptions. Build trust by being consistent and constructive with feedback, and most importantly, develop others by being conscious of needs and encouraging buy-in. Whether you are in-tune with yourself or you’re still navigating the self-section of EQ, one of my biggest takeaways from these sessions is to take time and observe how others manage their emotions. Are they bringing stress from home to work with them, or are they bringing their stress from work home? Notice their nonverbal communication or body language, their timing, how they deliver messages, and how they respond to feedback. How do their reactions impact the rest of the team? How does it compare to how you manage your own emotions? Are you self-aware and actively practicing self-regulation in your everyday life, and are you setting an example for them even if they are dysregulating?
I began thinking about how the LOD tools I received in this program can help anyone who is willing to learn navigate difficult situations in daily life, well beyond the workday. It prompted me to reflect on how my behaviors and reactions in both my professional and personal lives are not only interrelated, but consistent. I reached a point a few years ago where emotions and behaviors aligned just right, and while I am human and burnout can manifest in many ways, the regulation has helped me surpass the glass ceilings I had at that time. In an ideal world, leaders should be able to coach others to recognize and regulate so they can exceed all expectations they’ve set for themselves. If you say you want to be a leader and shatter your professional glass ceiling, keep in mind that it will never be handed to you. Simply excelling at the laboratory skills associated with your job is not enough to be a leader as low EQ will unveil itself immediately. As a leader, you need to be able to regulate your emotions and practice social awareness and relationship management. I encourage you to self-reflect and assess your emotions and behavior both at home and at work, in your family life, and in your social circles, under stress and when you find peace. As for relationship management, understanding your reactions and the behaviors of your team members provides insight to the overall team’s wellbeing and how it shapes the culture of the organization. While these trainings are required for new leaders in our health system, I can’t help but feel that most should also be required for all employees. Things like behavior exploration, EQ, feedback, and communication – these are critical soft skills that all employees could benefit from professionally. But it’s more than that – these tools can help you succeed in your personal relationships and overall well-being. With ongoing self-regulation and relationship management, you can break every glass ceiling you hold over yourself. It’s okay if you’re a work in progress; think of it as personal continuous improvement.
-Taryn Waraksa-Deutsch, DHSc, SCT(ASCP)CM, CMIAC, LSSGB, is the Cytopathology Supervisor at Fox Chase Cancer Center, in Philadelphia, Pennsylvania. She earned her master’s degree from Thomas Jefferson University in 2014 and completed her Doctorate of Health Science from Bay Path University in 2023. Her research interests include change management and continuous improvement methodologies in laboratory medicine. She is an ASCP board-certified Specialist in Cytology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree. Outside of her work, Taryn is a certified Divemaster. Scuba diving in freshwater caverns is her favorite way to rest her eyes from the microscope.
Jamie, the manager of a large metropolitan hospital lab, has many responsibilities. She must spend most of her time in the office, on the phone, or in meetings. She does find time to come out to speak with the employees, but only for a second to check on things or maybe make a request. During a recent safety audit, Jamie received feedback that several employees were seen working in the lab without using the proper PPE. One tech was working the bench without gloves, one individual had their lab coat on but not buttoned, and one auditor noticed that no one in the lab was wearing face or eye protection. This came as a shock to Jamie, she had never noticed this before. This doesn’t necessarily mean that Jamie is a bad manager, it could be that she was so focused on daily operation issues and she failed to notice other problems.
We have all heard the term “nose blind.” It’s when a person is around a bad smell so frequently that they become oblivious to its presence, and this can actually happen with vision as well. Have you ever heard the phrase, “you can’t see the forest for the trees,” or maybe the term “snow blind?” This phenomenon occurs when someone is concentrating so hard on one problem they may miss a more serious safety issue directly in front of them. Lucky for us, we have a tool to help those safety issues stand out. We have our “Safety Eyes!”
Ok, so what exactly are Safety Eyes? Are they some kind of new eye protection device that fit directly on your eyes? Are they indestructible eyes? Not exactly. Safety Eyes is a term used to describe the ability to spot current or potential safety issues more easily. It is the ability to walk into a room and immediately scan the environment for safety issues. This ability doesn’t just magically develop, it takes time and effort to master, and once you have it, you will begin to notice issues without even trying.
There are methods you can use to develop your safety eyes. Like any other sense, it is important to practice using it frequently so that its use becomes second nature to you. Think about this in terms of a wine sommelier. A sommelier may train for several years to acclimate their nose and palate in order to detect various nuances in different types of wine. It is through experience and exposure to many different types of wine that they are able to pick up on the slightest hint of a flavor or scent. This same repeated exposure works for sharpening your Safety Eyes as well. It is probably unlikely that you have a Safety Unicorn in your lab who can pick up on potential safety issues on their first day on the job. To become better at seeing safety issues, perform periodic rounding in the department and look for specific safety issues. Start by covering one specific safety area such as PPE use, waste management or fire safety. Your ability to quickly notice issues in these areas will sharpen, and you will be able to expand your newly honed power to other areas.
By developing your Safety Eyes, you will become more aware of various types of safety issues and where they are most likely to be encountered. It is easy to become “nose blind” to safety issues in a lab where you work every day. Start by simply using a checklist to focus specifically on one new safety area and soon the issues that may have been there all along will be more easily detected. Now that you can see the forest, you can make those important changes which will improve your overall lab safety culture!
-Jason P. Nagy, PhD, MLS(ASCP)CM is a Lab Safety Coordinator for Sentara Healthcare, a hospital system with laboratories throughout Virginia and North Carolina. He is an experienced Technical Specialist with a background in biotechnology, molecular biology, clinical labs, and most recently, a focus in laboratory safety.
Even though I readily share and celebrate my accolades with family and friends, I have generally been quiet with my coworkers regarding career moves. When I passed the ASCP Specialist in Cytotechnology BOC exam three years into my career as a cytotechnologist, I only shared the news with my supervisor, cytopathology director, and a few other pathologists. After dabbling in budget and supply purchasing and compiling monthly and annual QA statistics, I completed ASCP’s certificate program from Lab Management University in 2018. The following year, I traveled to Puerto Rico for the American Society for Cytotechnology (ASCT) conference and sat for the International Academy of Cytology (IAC) Comprehensive Examination. Six weeks after the exam, I received word that I passed, and again, I immediately shared the exciting news with my supervisor and cytopathology director. No one else at work had a clue until a year later when they noticed extra initials behind my sign-out signature. Then, the ASCP 40 Under Forty application and eight weeks of waiting came and went this past summer and once again, I elatedly celebrated with my superiors. I have always moved in silence amongst my peers to maintain an inclusive and docile/same-level environment. While some might be supportive, not everyone actively encourages growth. Furthermore, not everyone wants an all-you-can-eat buffet on their work plate, and many lab professionals are happy with a less stressful, entry-level competency kind of routine. And that is perfectly A-OK too! Regardless, I am who I am, and for the lab professional who loves continuing education and learning new techniques and advancements across the field of health care, I wondered what career moves I would make in 2021. What goals should I set out to achieve? What is my next step?
There it is. A doctoral program. 100% Online and meant for the full-time working professional. I have officially embarked on my eight-semester-long journey to earning a Doctorate of Health Science (DHSc) with a concentration of Organizational Excellence in Healthcare. Rather than a traditional PhD which prepares scholars for research-based careers in a very focused area, the DHSc is an applied doctorate focusing on healthcare leadership in various disciplines. Now that I am halfway through my first semester, I can honestly say this is one of the best decisions I have ever made. Learning about applied leadership theory in healthcare and how to effectively, efficiently, and efficaciously lead in a complex healthcare landscape has been so intellectually stimulating thus far. Most recently, my classmates and I engaged in a discussion emphasizing how today’s leaders must stay relevant in their dynamic fields, and we shared our required competencies (i.e., the knowledge, skills, and abilities) for leading people and managing resources for both today and tomorrow (Ledlow & Stephens, 2018). A recurrent theme we uncovered is the necessity for continuing education – whether it be formal or informal. Staying relevant requires healthcare leaders to read, research, and teach. As cytotechnologists, we have existing continuing education programs in place, such as ASCP’s Credential Maintenance Program, recommending certificants to participate in and record credits to renew their certifications. We have Interlaboratory Comparison Programs through the College of American Pathologists (CAP) that feature ancillary studies as a diagnostic companion to cytology slides. We watch cytoteleconferences provided by the American Society of Cytopathology (ASC). We are encouraged to attend our affiliated societies’ national conferences to collaborate interprofessionally. With all that is available, however, we still need to do more than just claim continuing education credits.
We need to stay abreast on how our field of laboratory medicine is changing and how we can accommodate those changes and adapt to those changes. We need inspiration and motivation throughout the organizational hierarchy. We need passion and commitment from all levels and all disciplines. We need transformational, flexible, and culturally competent leaders to serve as mentors for the next generation of leaders. We need leaders who continuously self-reflect and improve as they build diverse, yet cohesive teams that thrive on generating positive outcomes for the organization. To the current leaders, leaders-in-training, and the followers with potential – we must get better, we must take more initiative, we must aspire to learn more than just the “what” or the “how,” but most importantly the “why.” For the upcoming year and beyond, I challenge you to continuously learn more about your field of laboratory medicine and its impact on society. Ask why the pap guidelines have changed. Ask about the advantages of robotic bronchoscopy. Ask what molecular tests are available and which are currently in development. Ask what we can do to reduce the burden of disease in our community! Refrain from saying, “I don’t know” and respond with, “I’ll find out.” Become an expert in your field by understanding the interdependency of laboratory disciplines and beyond, and strive to actively network with each other. For those who want more, please do more! Pursue more! There is no ceiling on your potential, and there are no limits to your growth.
So sayonara to 2020, and hello to 2021! New year, new me? No. New year, improved me. And hopefully an improved you!
1. Ledlow, G.R. & Stephens, J.H. (2018). Leadership for health professionals: Theory, skills, and applications (3rd ed.) Jones & Bartlett Learning.
-Taryn Waraksa, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
“Where do we go from here…chaos or community?” is the question Dr. Martin Luther King, Jr. asked in 1967 before the civil rights riots in the hot summer of 1968. The query was directed to the nation as it sought to address the racism and pain deeply felt in the daily lives of its African-American citizens. Over 50 years later, that very same question is asked again as the nation is roiled with civil demonstrations, daily videos of racist behavior, and the seemingly senseless killings of African-American men and women.
As American culture and the nation evolves, uncomfortable conversations are beginning to occur in healthcare and across the country. Laboratory administrators and managers may want to reflect on the culture of their laboratory to ensure all voices are heard and that they are creating and supporting an inclusive work environment.
Diversity, inclusivity, and equity are goals healthcare organizations seek to incorporate into their culture to foster a healthy workplace environment and be reflective of the communities they serve. As with most industries, the laboratory has found itself challenged to improve cross-cultural intelligence and eliminate implicit and unconscious bias. The scientific community would like to believe it operates and makes decisions based solely on objectivity and facts. However, everyone is human and prone to perceptions influenced by preconceived beliefs and life experiences.
In the laboratory, questions involving race relations are pondered and discussed by workers of all creeds and colors. Historically, laboratorians have viewed themselves as scientists focused strictly on the pursuit of facts, hard data, and helping patients. However, one would err in thinking the lives of minority lab workers were encased in impenetrable bubbles of logic and reason. Instead, early on in their career (correction—their lives), many minority workers learned to compartmentalize and hide feelings of unfairness and helplessness in their effort to “fit in” and not make others feel uncomfortable.
Laboratory administrators should let employees know that their office is a “safe place” if an employee feels he or she needs to discuss issues affecting how they feel about their work environment. Many employees of color working in predominately white environments may avoid conversations involving race out of fear as being labeled as “one of those.” However, avoiding difficult conversations does not make the problems go away; in fact, the lack of addressing an issue often creates a more significant problem later on, or the employee simply quits. One thing managers should be prepared to hear if they are successful in creating a safe space and the employee chooses to talk, harsh truths.
Lab managers can be proactive and ask if the employee has encountered any barriers or obstacles to their success in the healthcare organization. Minority employees frequently experience microaggressions, favoritism, and racial discrimination. Discussing feelings may provide a release for the employee, allow the manager to begin to understand, and offer the opportunity for the manager to reflect on their behavior.
The diversity of today’s protest marchers provides evidence of the progress America has made toward vanquishing the problems of racism and discrimination. All colors, creeds, and ethnicities are together expressing their desire to defeat the scourge of racial injustice. Laboratories are a part of the social community, and minority employees are often reluctant to share anxiety and experiences they feel are race-based. Lab managers should be reflective and reach out to their employees to let them know their office is a “safe place” to discuss issues openly, including those with racial overtones. It is only through open and honest dialogue that we can avoid chaos and become the community we seek.
Darryl Elzie, PsyD, MHA, MT(ASCP), CQA(ASQ), has been an ASCP Medical Technologist for over 30 years and has been performing CAP inspections for 15+ years. Dr. Elzie provides laboratory quality oversight for four hospitals, one ambulatory care center, and supports laboratory quality initiatives throughout the Sentara Healthcare system.
Many years ago a woman purchased a cup of coffee in a restaurant drive-through. Not having a cup holder available in her car, she placed the cup between her legs to hold the coffee while she reached for money to pay for it. She burned her legs, sued the restaurant, and actually won her court case. Now such restaurants are required to warn customers with signs stating the obvious; “coffee served hot.” Before this regulation came to be, however, many people were aware of the possible danger of placing a hot cup near their skin. Does having a posted sign make customers safer? What about the lab environment? There isn’t an explicit safety regulation written for every action that could create an unsafe situation. So what are a few of the hidden and maybe no-so-obvious things might your staff need to know in order to keep safe?
You can’t chew gum in the laboratory. It’s true, but sadly, it’s not written down anywhere as a regulation. OSHA’s Bloodborne Pathogen standard says that “eating, drinking, smoking, applying cosmetics or lip balm, and handling contact lenses are prohibited (in the lab).” It says nothing abut gum, throat lozenges, hard candy, or even chewing tobacco. The unwritten rule is that OSHA is trying to prevent hand-to-face contact while working in an area where infections can be acquired easily this way. There are multiple routes of entry via mucous membranes- a major source of pathogen exposure- your mouth, nose, and eyes. Laboratorians should always keep their hands away from their face when working in the department. These activities are just another opportunity for hand- to-mouth contact. While you might be able to show the safety officer you are putting these things in your mouth outside of the lab, you would not be able to prove that to an inspector, and they will rightly cite you for it. If you need help enforcing this, be on the lookout- by the end of the year there will most likely be a regulatory body that addresses gum chewing directly.
How long should staff wear PPE? During the COVID-19 pandemic, many have asked about the effectiveness of various PPE and have looked for written guidance discussing how long it should be worn. In general, studies show that gloves lose barrier effectiveness in about two hours. Wear them that long if they are not visibly soiled while in use in the lab. Lab coats- disposable or reusable- can be worn for one week in the general lab setting unless something is spilled on them. Once a new coat is worn, the outside is considered contaminated, but that does not mean it cannot be re-used. It is wasteful to change coats every day unless there is a reason to do that (i.e. in a specialty lab where cross-contamination will be an issue). Face shields worn by staff can be reused as well, and they can be cleaned with alcohol-based products for disinfection. Rarely should a wearable face shield or goggles be used only once before disposal.
Mesh shoes are not allowed to be worn by lab personnel. Again, other than in CLSI guidelines, it will be difficult to find that written clearly in lab safety regulations. Laboratory footwear should “be comfortable and cover the entire foot, including the instep and the heel. Because canvas shoes will absorb chemicals or infectious fluids, they are not recommended. Leather or a synthetic, fluid-impermeable material is suggested. OSHA’s PPE standard does insist that employers take measures to protect the feet of employees. In the lab and specimen collection setting, that means footwear needs to protect from biohazard materials, chemicals, and even sharps. Mesh or canvas shoes do not fit the bill, and neither do clog-style shoes (even if they have a heel strap). If you need to, set your lab’s footwear policy through the dress code or maybe the Chemical Hygiene Plan. If staff tells you they can’t find this type of footwear, tell them to look harder. All across this country, hundreds of laboratory employees are wearing the appropriate shoes, and they are available at several different stores.
Often, because these safety rules are “unwritten,” staff will challenge you on them. It can be difficult to try to enforce these important safety measures if you can’t properly educate the staff about why they exist. Be sure to know your regulatory resources, and don’t be afraid to dig deeply into the references to find the answers you seek. Lab leaders can write their own policy, and it can go above and beyond what the regulations state if needed. The safety standard may not be clear and direct, but it these are still important measures to take. Just like that lady may have needed a sign to prevent her from putting hot coffee in her lap, your staff needs clear safety guidance to keep them safe from a lab-acquired injury or exposure. Provide the tools they need to remain happy and healthy members of your lab team.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Hello again everyone and welcome back to Lablogatory!
If you read my post last time, I talked about preserving integrity and delivery of our professional duty as laboratorians in the face of both overwhelming pandemic demands as well as working to advocate for our field as more people realize each day what goes into every single lab result around the world. A run on sentence and a heavy discussion—and it was just in time to celebrate Lab Week 2020!
This time let’s expand on the second topic a bit. Advocacy in our profession and spotlighting our critical roles as pathologists and medical laboratory scientists. As much as you or I might agree that this is proof positive, just from looking at the regular old news media this year, it’s not so easy. But something that’s been quietly creeping higher and higher on the Lab-Med radar this past year or so is now growing faster than it ever has before: Social Media.
The medium you disseminate information on also translates a message about the author/speaker. For me, I was not only staying the course about data-driven testing science regarding COVID, but I took every ad-lib and opportunity to praise the medical laboratory profession. I praised laboratorians for their hard work, and took a minute to say clearly and plainly, that they are indisputably healthcare heroes in this season of notability. In doing so, I found myself addressing a more pressing pandemic: The Path and MLS pipeline problem. We have a serious issue with finding new medical laboratory scientists and medical students to go into our field. The main cause and culprit? Our essential clinical invisibility. As we are much less patient facing than our other colleagues, it’s difficult to expose younger students considering various careers in healthcare to our specialty. Cue Twitter, Facebook, Instagram, LinkedIn, and even TikTok.
Image 1. Throwback to the 2019 ASCP Annual Meeting in Phoenix, AZ. Dr. Kamran Mirza (left), myself, and Dr. Adam Booth (right) are all part of the growing community of pathologists/trainees plugged into the social network to advocate, collaborate, and spotlight our profession. Follow them both on twitter at: @KMirza and @ALBoothMD, they are champions of using social media as an educational connection.
I’ve talked about this before. And, of course, I’m biased: I’m on the official ASCP Social Media Communications Committee and was highly active in previous iterations including the #SoMeTeam as well as ASCP Social Media Ambassadors programs. Anyone who reads my pieces here knows I’m not social media shy—heck, I weaponized my online presence for residency interview season, networking around the clock to get my name and my work out there for programs to notice. Spoilers: it worked really, really well.
(If you’re one of those senior medical students who is preparing to practice the age-old tradition of wiping the internet clean of your presence, consider a 180 turnaround from that plan—at least if you’re applying to pathology…)
So what worked so well for me? Well, first some background. You know I’m on two ASCP committees, CCPD and Social Media. I’ve already told you I’ve been working the social media angles for a while now, at ASCP meetings, sharing content, etc. And I had a super busy, and super rewarding, residency interview season. With rotations and interviews at some amazing places, I was able to both learn a lot about what it is I really want to do and meet folks to talk about it with. All that being said, sometimes things just fall into place. Specifically, a global pandemic happened. …too soon?
I’m not going to rehash the early days of the pandemic for you, or talk about how I became involved on the ground floor of a lot of outreach and education efforts: that was sooo last month, I did that already (read it all here). But what I will talk about is the butterfly effect that each media engagement set into place for me.
Image 2. When everyone’s talking, the loudest microphone gets the audience. When no one’s making sense, the best content wins. Many of the talks and interviews since the very first ones with my friend and colleague Dr. Ajufo set up a cascade of content to answer some serious concerns during these strange times.
In effect, the order of events for me these last few months looked like this:
Writing pieces for Lablogatory¸ some based in scientific analysis of testing, some to address public health concerns and education.
Making small viral online tid-bits aimed at educating lay people about overall health, avoiding exposure, and what testing means.
Social media connection to join the #PathCast lecture series, of which my video has garnered approximately 20,000 individual views and was seen in almost 50 countries.
Invitations from CDC-funded training agencies to explain testing considerations, virology details in translational science, and discuss how those most vulnerable to social determinants of health are most inequitably affected by pandemic conditions.
Informal features where I was invited to discuss those intersectional tenets of medicine, public health, and socioeconomics with lay persons in a virtual group setting.
An interview with Lifehacker magazine’s Vitals section, to answer reddit-style ask-me-anything questions regarding COVID testing online live with open to the public availability.
Inclusion in Lifehacker magazine’s online podcast, where I was featured alongside other experts to discuss the effect of the pandemic on many aspects of life from health to finances.
An interview with The Endless Files Podcast¸ where I was invited as a content expert to discuss the connections between laboratory data, public health, public policy, and discuss the political climate surrounding coronavirus concerns all over the sociopolitical spectrum.
An interview with People of Pathology Podcast which gave me the chance to talk about my individual career path and transition from education about testing to advocacy and representation for our amazing profession.
The nomination and selection by my medical school faculty and peers to deliver the student charge at my formal, virtual, medical graduation.
…more are on the way!
Why am I listing these things? Is it my misplaced Greek hubris? Maybe. But before I fly too close to the sun, I’m trying to prove a point. That what started out as creating content on social media for health and wellness during a pandemic essentially became a snowball by summer. I was addressing pressingly relevant information during the obvious opportunity to step up and educate. But something else was happening; something I didn’t realize until recently. And whatever it was, I wasn’t getting there alone.
**All of this was made possible by social media recommendations and connections from friends and colleagues!**
PathCast? I was recommended by a pathologist friend on ASCP’s CCPD committee with me. The CDC-funded training? A former grad student friend of mine when I studied at Rush. Lifehacker? Made possible in a public call for content by our favorite medical lab scientist and Lablogatory editor, Kelly Swails. The Endless Files? Reached out to an old political science professor and friend at Loyola. People of Pathology? Social media connections with friends and CLS colleagues in Canada—you want to make things happen? Don’t go at it alone!
Don’t know how to get started in all this social media frenzy? Don’t fret. Basically, here’s a four-step process: make accounts on one or all of your favorite platforms, follow everyone you want to learn more from, share other’s content or your own frequently, and (most importantly) promote others before yourself! There are countless webinars and talks on how to use social media to leverage advocacy and education, just look at some of the greatest pathology teachers on Twitter: @KMirza, @CArnold_GI, @MArnold_PedPath, @RodneyRhode, @HermelinMD, @KreuterMD, @JMGardnerMD, and many, many more. But there’s more than just twitter! Many super talented folks team up to produce lectures, webinars, and even podcasts (check out the brand-spankin’-new PathPod here!)
Just dive in!
Image 3. Virtual graduation, social media outreach. 2-for-1 sale. In my on-screen graduation quote during the conferment of degrees, part of it read “don’t let me be the last pathologist you were friends with…” and during my student address, I implored my classmates and anyone else watching to consider creative, new ways to solve clinical problems. Maybe with new tools, new skills, and a new understanding of interdisciplinary collaboration. I also reminded people that our digital presence can indicate our professional message, as champions of truth in science.
In conclusion, social media is the new (old) heavy hitter in the medical world. Younger med students are getting access to more specialty information than they ever have before, informing and guiding their career choices. Specialists of all kinds share and reshare excellent diamonds of content that galvanize medical discourse everywhere from Twitter to TikTok. What does this do? It closes the gap between professionals across disciplines, shines new spotlights on fields that traditionally got stamped with basement autopsy stereotypes, and creates digestible and understandable bridges for lay people to access our jargon-filled discourse. It only goes up from here.
Post-script: if you haven’t noticed the racially charged, horrible situations adding to the tumultuousness of 2020, there’s another lesson in this. Social media again proves a most-valuable and all-powerful tool to mobilize, demonstrate, collaborate, and unify thoughts, ideas, and causes. I doubt we will ever be free of tragic moments in history, but when we come together as one collective we can use our various platforms to honor heroes, shame wrong doers, celebrate positive change, and highlight systemic failings that might hold us back from true progress, justice, and peace. That includes the medical world, as all things cross at the intersections of human life and human rights.
Thank you for reading! Stay safe, stay well, and continue to practice safe, compassion-informed social distancing. The pandemic isn’t over, and neither is our work.
Until next time!
-Constantine E. Kanakis MD, MSc, MLS (ASCP)CM is a new first year resident physician in the Pathology and Laboratory Medicine Department at Loyola University Medical Center in Chicago with interests in hematopathology, transfusion medicine, bioethics, public health, and graphic medicine. His posts focus on the broader issues important to the practice of clinical laboratory medicine and their applications to global/public health, outreach/education, and advancing medical science. He is actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Watch his TEDx talk entitled “Unrecognizable Medicine” and follow him on Twitter @CEKanakisMD.
“Never, ever underestimate the importance of having fun,”
said Randy Pausch, a professor of computer science at Carnegie Mellon
University. Indeed, having fun is an important component of life, and that
includes your professional life. However, having fun in the workplace can seem
like an impossible task sometimes. There is, after all, lots of work to be
accomplished, performance to be measured, and projects to complete. This can
make it challenging to find of time and ways to have fun appropriately and
constructively.
The benefits of having fun in the workplace are plentiful. Because
most fun activities require people to work in groups or teams, the shared
experience can increase collaboration, engagement, and foster communication. Having
fun fosters motivation and commitment to an organization as people associate
the positive feelings and experiences with the workplace. This also increases
morale and comradery among the participants, which increases their performance.
All these aspects, in turn, foster creativity, innovative thinking, and
problem-solving skills. The more creative employees are, the more comradery
they feel among themselves, and the better they perform the more turnover is
reduced. Having fun in the workplace is incredibly beneficial to both the
employees and the organization overall.
In today’s workplace culture, people are generally more
aware and considerate of what is appropriate behavior. This also applies to
having fun, because if activities are only fun and enjoyable if they are
appropriate for everyone involved. It is, therefore, important to establish
clear boundaries: what is considered part of this activity and what is not. It
is also important to consider different levels of physical, mental, and
emotional ability. Having fun is inclusive and collaborative, so it is critical
to design activities that everyone can partake in. The activity should also
always be optional. Making participation mandatory is not actually fun for people,
so make sure that there is an opt-in and opt-out option. Finally, every
activity should have some element of learning and education. If you are asking
people to participate in a fun activity, ensure that they are learning
something about one another or about a specific topic.
There are many different ways in which you can incorporate
fun in the workplace. Last year at ASCP, our social committee hosted an ‘Oscar
Party” in which we could vote for our colleagues in categories such as “Outside
the Box Thinker/Innovator,”, “Outstanding Philanthropist,” and “Rookie of the
Year.” Then all staff gathered in the kitchen area of our office that was
decorated with a red carpet and we all received a glass of sparkling cider. The
winners were announced and cheered on as they walked the red carpet. They gave
a short speech after receiving their little Oscar award. It was a simple way to
have some collective fun and it felt so great cheering everyone on and
recognizing certain employees for their outstanding contribution to the society.
On average, babies laugh about 400 times a day. Adults, on the other hand, only laugh about 35 times a day and significantly less often on weekdays than on weekend (Beard, 2014). Laughter is incredibly important to our overall well-being and performance. In fact, “laughter relieves stress and boredom, boosts engagement and well-being, and spurs not only creativity and collaboration but also analytic precision and productivity”(Heggie, 2018). So, let’s try to incorporate more fun and more laughter in both our personal and our professional lives. Let’s find ways to cheer each other up and create a collaborative, warm, and productive environment that fosters engagement, retention, and analytic precision. After all, laughter is the best medicine.
-Lotte Mulder, EdM, is the Senior Manager of Organizational Leadership and Patient Engagement at ASCP. She earned her Masters of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. After she graduated, Lotte started her own consulting company focused on establishing leadership practices in organizations, creating effective organizational structures, and interpersonal coaching. She has worked in Africa, Latin America, Asia, and the U.S. on increasing leadership skills in young adults through cultural immersion, service learning and refugee issues, and cross-cultural interpretation. She is currently working toward a PhD in Organizational Leadership.
During the 2019 ASCP Annual Meeting in Phoenix, I noticed a
morning workshop session entitled “The Impact of Fun.” The title intrigued me,
so decided to take a break from the science and clinical medicine workshops
that I would normally attend, and take advantage of the opportunity to listen
in.
I have been working as a pathologist and lab director for 30
years, and while I hate to admit it, I had never thought seriously about taking
time during the day for playing games with my co-workers. I was always consumed
with meetings, deadlines, and getting the clinical work completed.
At the beginning of the course, I was a little unsure what I
had gotten myself into. However by the time the workshop concluded, the reality
of what I had been missing had set in.
When I returned to work following the meeting, I began to
search for fun activities that our lab team could do over a lunch hour. I set a
date and promised food to entice the wary into attending the event in the
conference room. Once they had assembled, I divided the group into two teams by
drawing an imaginary line down the middle of the room. We then played team trivia
using a book of questions I had acquired. By the end of the hour, everyone was
laughing and having fun. The lab continued to buzz with talk and occasional
laughter all afternoon.
We have continued setting aside one noon hour each month
where we gather for different types of games. Charades, and Pictionary have
been hits. Mostly everyone brings their own lunch, but food or deserts are
provided on occasion to keep these events special. There are a few who choose
not to participate, but even they occasionally show up to watch and laugh along
with the rest. As is pointed out above, you cannot make having fun a mandatory
or it ceases to be fun.
Our lab staff really seem to enjoy these events and so does
this old pathologist. During our most recent event, one of my young colleagues
remarked how much fun these lunches have been, and that they hoped we would
continue these going forward. I intend to keep these going as long as I
continue working. It has provided me with an opportunity to get to know each of
my co-workers much better. I only wish I had learned about the importance of
having fun with your co-workers and teammates earlier in my career. I encourage
other pathologists, lab directors and section supervisors to learn from my
experience and begin finding ways to bring the fun back into the workplace if
you have not already done so.
-Dr. Wisecarver is currently Professor Emeritus in the Department of Pathology/Microbiology at the University of Nebraska Medical Center in Omaha, Nebraska. He served as Medical Director of the Clinical Laboratories for Nebraska Medicine, their clinical affiliate from 1996 until 2017. He currently serves as the Director of the Histocompatibility Laboratory for Nebraska Medicine.
After a lot
of positive responses and sharing on social media, my article last month got lots of people talking about
annual meetings and how great they are for networking, learning, and advancing
our profession. Not too long after the ASCP Annual Meeting in Phoenix, I was
back in my Manhattan apartment working on my speech and graphics for a real
life TEDx session hosted at my medical school.
Let’s pause
here: if you either haven’t heard of the TED/TEDx brand or if you binge watch
their 18 minute videos and want more links to watch now, now, now!
TED
is a non-profit organization whose mission is to share “ideas worth spreading.”
They’re about 35 years old and based in NYC stateside, and Vancouver in Canada.
Basically, over the last few decades they hold conferences at those flagship
sites called “TED talks” where selected speakers present on a myriad of topics.
TEDx conferences are officially licensed but off-site events which operate
under TED protocol and guidelines. There have even been spin-off conferences
like TED MED, which focus solely on healthcare.
Image 1. What’s a TEDx talk? Basically, an off-site, officially sanctioned, “idea sharing” conference.
Some of the students at AUC School of Medicine, organized such a conference with official TED licensing and recruited me to join their list of speakers to deliver talks on their chosen theme: resilience. Officially called TEDxAUCMed, this conference included community members, students, artists, activists, and more discussing the human capacity for resilience in ways not commonly discussed. “Weathering the Storm” was the official event title, as the school located in the island nation of St. Maarten displays daily resilience especially since being hit by Hurricane Irma in 2016. Among their list of incredible speakers, I was humbled to be included! I titled my talk “Unrecognizable Medicine” and wanted to deliver a talk to students, clinicians, and those of us in medicine witnessing first-hand a tidal wave of new technologies and paradigms that redefine the way we discuss health. Oh, and since I’m a huge fan of #GraphicMedicine more and more each day, I hit that hashtag hard and decided to illustrate my whole talk!
Image 2. Title Card from my TEDx talk.
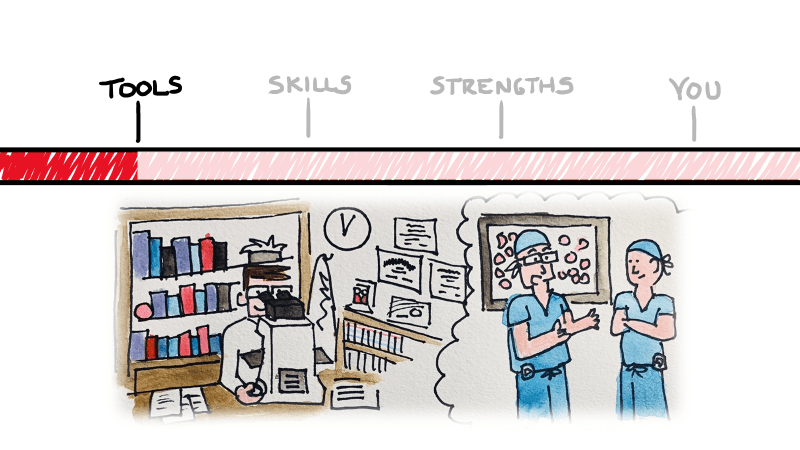
So what did I talk about, exactly…and what’s the big deal? I’m not going to re-hash my presentation for you in text—that’d be boring, and I’m obviously going to put a link at the bottom for you to watch it yourself. I got you, lab fam! But essentially, what I set up was a three-tiered template to assess and navigate that tidal wave of tech. Tools, skills, and strengths—three things inherent to the practice of medicine in any specialty.
Image 3. Red back-ligting. So intense. Thanks for coming to my TEDx Talk, literally!
There are
untapped topics in medicine which are looming over the horizon. As medicine
continues to evolve and change, the problems we face and the needs we must meet
will become moving targets. New specialties will emerge, and new technologies
will replace centuries old tools we cling to today. A shift in thinking is both
proactive and healthy in a profession that mandates our commitment to
preserving health and quality of life. I have spent years battling stereotypes
in medicine and hope to challenge the fabric that places individuals in
professional or academic boxes. Fresh first-years at some schools are already using
point-of-care ultrasounds (POCUSes) instead of stethoscopes—which
student sounds like they have better info on morning rounds, a student who
maybe kinda-sorta heard some non-descript murmur, or a mini-pocket
echocardiogram with an ejection fraction of 45%? Stereotypes have too long
shaped the way students choose specialties, equating some areas to colloquial
high school cliques! No offense to orthopedics or dermatology. Troponins used to be something you
could hang your white coat on, but not anymore. What do you do with a new 5th
generation Trop of 39 with a delta of 18? ACS or acute MI? Cancer therapy is
exploding with personalized treatments being added every day! Any student right
now would impress their heme/onc attending on rounds if they suggested PDL-1
and other immunotherapy testing for patients with newly diagnosed lung cancers.
*Deep breath*
Ok. My point
is, tomorrow’s medicine is going to have a lot of different therapies, tools,
and even vocabulary that schools may never catch up with. How do you prepare
for this explosion of knowledge? You look to yourself to take an inventory of
your strengths and use those to guide your clinical sails. Addressing
stereotypes head-on, learning on the spot, dealing with complex identities in
your patients, and always practicing with compassion will lend itself to
staying ahead and staying fulfilled.
Image 4. If you’re drawing cartoons of pathologists for an educational series, you probably make them look like you. Or in this case me, I guess. Keep an eye out for my #PathDoodles on social media!
Pretty heavy stuff right? But there’s something else that caught my attention in reflection on the TEDx talk… I’ve searched the TED library of videos, and while there are plenty of doctors, scientists, and pioneers in research discussing medical ideas, I haven’t seen any medical laboratory scientists. If you find any, please correct me. But, as I understand it, it’s just me. And that’s something special.
Image 5. My wife and I check-in for rehearsal at the TEDxAUCMed conference in sunny St. Maarten.
There’s a
culture shift in our profession, and a lot of us are talking about it.
Pathology and laboratory medicine are stepping out from behind the healthcare
curtain and asserting itself as a champion for patients, truth, and the
importance of data-driven medicine. Not only do I talk to groups of folks every
time I get a stage, but I use social media to reach clinicians and patients!
Yes, I’m one of few medical students-turned-residency applicants who didn’t
change their name to hide their online presence for the winter. But instead of
a secret twitter hibernation, I’ve used social media as a tool to network,
engage, and connect.
One of my
favorite new projects is something I call #PathDoodles where I break down the
aspects of pathology and some specialty topics for those outside of medicine
(and sometimes just outside our profession). I’ve already covered things like
“what is pathology?” and the importance of autopsies, the role of medical
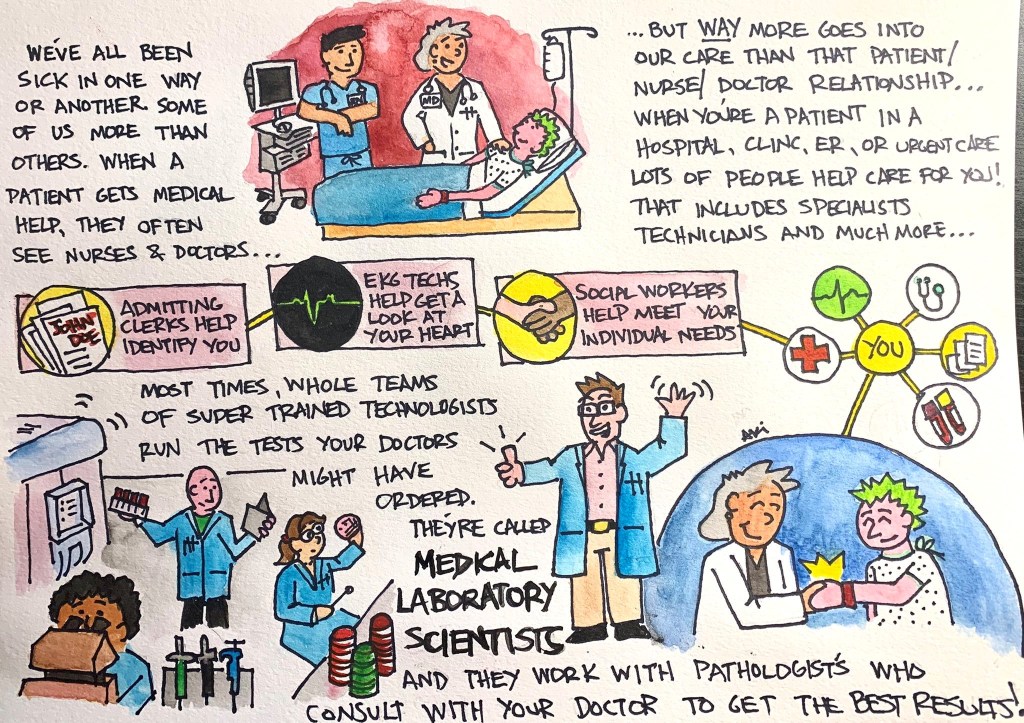
laboratory scientists, and I continue to add more regularly!
Image 6. One of a growing list of #PathDoodles.
There’s a
culture shift in our profession, and a lot of us are talking about it.
Pathology and laboratory medicine are stepping out from behind the healthcare
curtain and asserting itself as a champion for patients, truth, and the
importance of data-driven medicine. Not only do I talk to groups of folks every
time I get a stage, but I use social media to reach clinicians and patients!
Yes, I’m one of few medical students-turned-residency applicants who didn’t
change their name to hide their online presence for the winter. But instead of
a secret twitter hibernation, I’ve used social media as a tool to network,
engage, and connect.
One of my
favorite new projects is something I call #PathDoodles where I break down the
aspects of pathology and some specialty topics for those outside of medicine
(and sometimes just outside our profession). I’ve already covered things like
“what is pathology?” and the importance of autopsies, the role of medical
laboratory scientists, and I continue to add more regularly!
Follow me on Twitter (@CEKanakisMD) and check out my TEDx talk:
My talk begins at 5:00:00. Enjoy!
–Constantine E. Kanakis MD, MSc, MLS (ASCP)CM completed his BS at Loyola University Chicago and his MS at Rush University. He writes about experiences through medical school through the lens of a medical lab scientist with interests in hematopathology, molecular, bioethics, transfusion medicine, and graphic medicine. He is currently a 2020 AP/CP Residency Applicant and actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Follow him on Twitter @CEKanakisMD
So far
we have reviewed the different federal regulatory agencies responsible for
establishing laboratory testing guidelines, a brief overview of the different
roles each department plays, as well as a discussion on testing complexity. In
today’s post we’ll cover the optional accreditations available to labs, and how
accreditation differs from certification.
In the
simplest of terms, certification is a mandatory requirement, whereas accreditation
is optional. Certification is required in order for laboratories to receive
payments from Medicare or Medicaid. Laboratories must meet the minimum
requirements set forth by CLIA to earn and maintain their certification status.
Accreditation
is an extra additional step that laboratories can take to set themselves apart
from neighboring labs by holding themselves to a higher standard. Accredited
laboratories must still adhere to the minimum CLIA requirements, but there are
additional rules and requirements to be satisfied depending upon the different
accreditation agencies.
More
rules and paperwork, why would anyone volunteer to take that on? Depending on
the size, complexity, and client population that your lab serves, the benefits
to obtaining accreditation can greatly outweigh the challenges of maintaining
that accreditation status.
One of
the requirements to maintaining your CLIA certification is routine inspections
to confirm compliance with the rules. Accreditation agencies require
inspections as well, but thankfully in most cases your CLIA inspection can be
satisfied by your accrediting agency; meaning your lab will receive a single
inspection to satisfy both groups. Results will vary for each lab, but
generally speaking the accreditation inspections are perceived to be easier to
get through than those conducted by the federal inspectors. For example, agencies
like The CAP and COLA tend to be more focused on sharing of ideas and good
laboratory practices, rather than coming in as the “lab police” and looking
only for problems. The explanation of their regulatory requirements tends to be
more user friendly and easier to interpret as well, rather than the formal CLIA
laws which are legal documents and read as such.
Recognition
by an accrediting agency confirms that the laboratory is qualified and
competent to perform testing for which it has received the accreditation for.
This stamp of approval can help patients and clients feel comfortable in
choosing your laboratory for their testing needs. For laboratories that perform
testing as part of clinical trial evaluations, this can help reduce the number
of requested on-site audits by the client themselves, as the client may choose
to rely on the third-party accreditation assessment due to their high
standards. It may also help encourage new clients to choose you for their
testing needs, as the accreditation confirms your commitment to higher quality
standards.
Another
possible benefit of having accreditation status is the impact on your laboratory
staff. Continually striving to raise the bar on your standards and going above
the bare minimum instills a sense of professionalism in your employees. By
continually reviewing the regulations and preparing for or responding to
inspections, staff are more likely to be committed to complying with your
organization’s quality management system and standards of performance. Staff
who are familiar with the requirements and the reasoning behind why a certain
task is performed or documented, are more likely to comply with those policies
and procedures.
There
are currently 7 CLIA approved accreditation agencies: https://www.cms.gov/Regulations-and-Guidance/Legislation/CLIA/Downloads/AOList.pdf. Some agencies are focused on a
specific discipline, such as AABB for transfusion medicine, and others are more
encompassing for all of the laboratory departments. Organizations looking to become accredited
should research each option in order to determine which ones would be best to
meet their specific needs. It is also common for labs to maintain more than one
accreditation at a time, for example AABB and CAP. As always, the regulatory
agency with the most stringent rules would be the ones the lab is expected to
adhere to. In cases of joint accreditation, multiple inspectors may be needed
to complete the biennial inspection; however the agencies will try to
coordinate efforts and work together so that the inspections occur
simultaneously. Sticking with our AABB & CAP example, CAP will work with
AABB to locate an AABB approved inspector for the transfusion medicine
checklist, while the remainder of the CAP inspection will be carried out by CAP
inspectors. The AABB inspector would then inspect the transfusion medicine
department for compliance with both CAP and AABB requirements at the same time.
The accreditation process may be challenging, but once you have obtained that esteemed status, the opportunities for continual education and improvement of your laboratory will be endless.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s
2018 Top 5 in the 40 Under Forty recognition program. She has worked in
the medical laboratory profession for over 18 years. In her current
position, she transitions between performing laboratory audits across
the entire Northwell Health System on Long Island, NY, consulting for
at-risk laboratories outside of Northwell Health, bringing laboratories
up to regulatory standards, and acting as supervisor and mentor in labs
with management gaps.