Hi everybody—welcome back!
Although you better not have gone too far since last time, self-isolation and social distancing are still critical for us to get through this. Wash those hands, and dust off books and board games. #StrongerTogether (apart), am I right?
Yes, it’s going to be another piece on the current pandemic. It probably will continue to be so until conditions change. So, as your contributor to virology and testing these last two months, I’d like to take a minute to “zoom out” a bit and look at this pandemic in a different way.
It’s highlighting lots of things in healthcare from supply chain, to political regulatory red tape, to the mechanism of deliverables in the United States. And despite the title, I have no romantic epilogues about anything happening in Columbia at the turn of the 20th century. However, very much like the original book’s protagonist, I’d say there are a lot of us in Pathology and Laboratory Medicine alike who are champions of the scientific cause for advancement, education, and positive outcomes. And what better, more fitting of a time to celebrate this cause, than Laboratory Professionals Week 2020!
*** Never forget how vital you all are at every level. Technicians, technologists, medical laboratory scientists, administrators, directors, managers, residents, fellows, faculty, and staff all fit together in a magnificent (but often too unseen) tapestry that makes every patients’ tests results mean something so much more than numbers on a printed report. You’re all lab heroes, we’re all lab heroes. Go make sure you thank some of them this week (or anytime) and a heartfelt thank you to all of you from me as well! ***
In the mere month since I last wrote a piece for Lablogatory, so much has changed with the pandemic as well as my role in local and academic public health efforts. To name a few, I trained with the New York City Medical Reserve Corps as a public health educator early during the pandemic, I was invited to give a lecture on SARS-CoV-2 and COVID-19 testing considerations for lab professionals by the excellent pathologists who run the PathCast series, and I just recently finished a two-day series with an organization called Proceed who are sponsored by the National Center for Training, Support, and Technical Assistance (NCTSTA)—a CDC grant-funded education web series. I’ll mention a little bit about all these things (and of course link you to the material) and talk about how it all fits into what has quickly become a complicated social pandemic response.
NYC-MRC
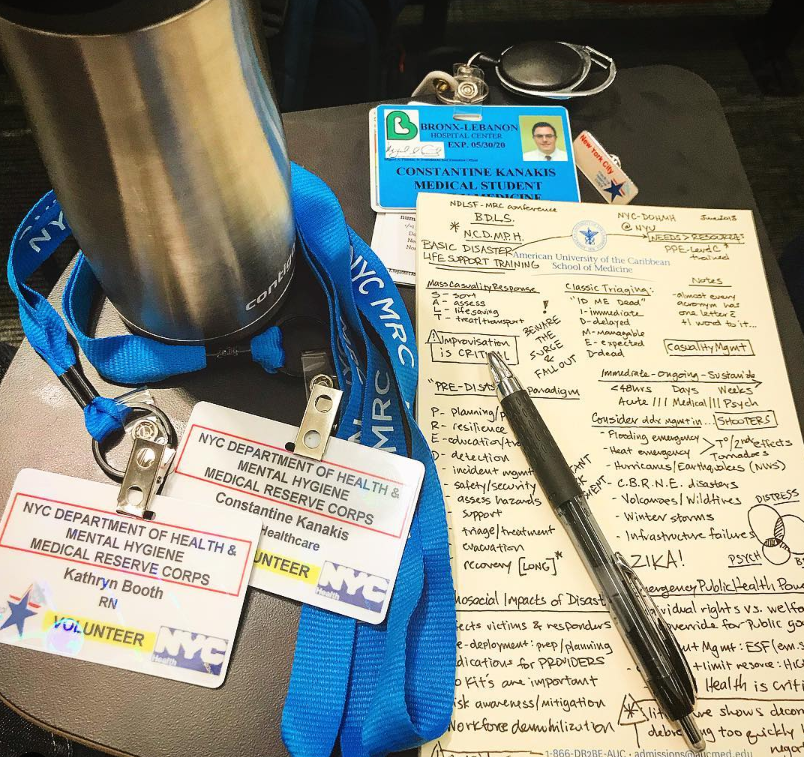
Almost as soon as I set up shop to start my medical school clerkships and clinical training in New York City, I joined the New York City Medical Reserve Corps—a collection of volunteer healthcare first responders in the event that the city at large ever needed to mobilize every available healthcare personnel during a disaster or health emergency. *Spoilers: turn on the news* At the same time I was prepping some pre-clinical research in infectious disease healthcare and contributing to ASCP’s Choosing Wisely initiatives addressing Hepatitis C testing in vulnerable communities with some of the nation’s highest rates of infection (read the flashback primers I wrote here and here), I was attending NYC-MRC seminars and becoming a nationally certified disaster responder. There have been drills, seminars, and lectures since joining in 2018 but nothing to really contribute to while I moved through clinicals. Welp, clinicals ended, I had a few weeks off for residency interviews, then Kung Pow! Enter the defining viral pandemic of 2020! Smooth sailing lectures became phone network scrambles to see if I obtained my medical license yet since New York’s hospitals were slammed! The last meeting I remember going to was a training on disseminating appropriate information to various levels of practice/professions. I didn’t know it yet, but this became paramount knowledge for me.
What Information Matters Most?
So what exactly did I learn? Essentially, it’s nothing groundbreaking or new, but the way you address certain topics matters more than you might realize. I once found myself in a room of mixed level healthcare providers, homeless shelter staff, local public health officials, hospital nurses, and lay people—that’s a broad range of knowledge and practice exposure. If you talk about upregulated ACE-2 receptor expression in intra-viral inflammatory response before full blown ARDS and DAD visible in lung biopsies you’ve lost half the crowd; and if you talk about epidemiology basics like reproductive number (R0), first cases found (FFX), and trace tracking, your provider audience is suddenly looking at their phones. But almost none of them know enough about laboratory testing, regulations, or quality assurance measures—so that became my target, and my bridge to connect everyone. I began collaborating with a friend and colleague Dr. Emeka Ajufo, who matched into his top-choice pain management and rehabilitation (PM&R) residency, and started creating content that connected topics like wellness, one health, and prevention while at the same time understanding deliverables and quality behind lab testing.

PathCast
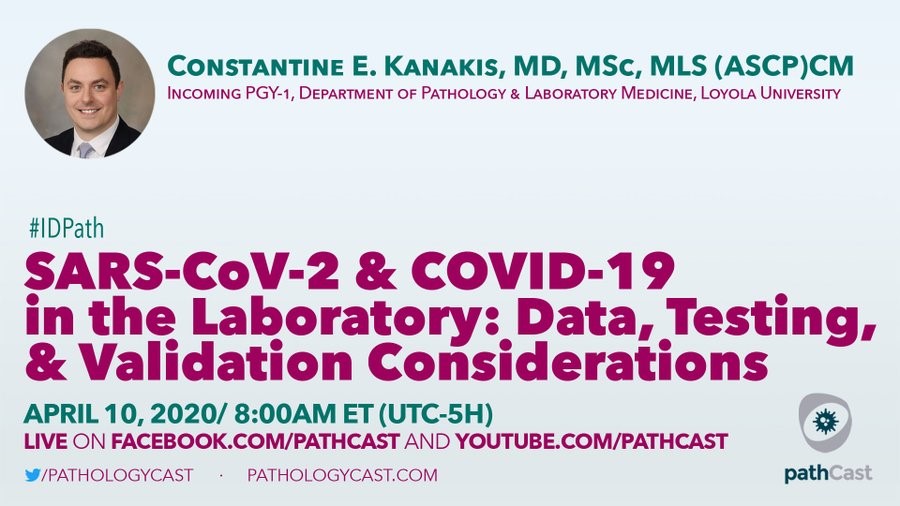
So this partnership content got noticed on Twitter (@CEKanakisMD) by the folks that run the PathCast simulcast series on Facebook and YouTube. Dr. Rifat Mannan (@mannanrifat03 on Twitter) from the University of Pennsylvania Hospital and Dr. Emilio Madrigal (@EMadrigalDO on Twitter) from Massachusetts General Hospital have been hosting and promoting a mountain of impressive faculty lectures for all kinds of topics in pathology since 2016. They host them live for viewing across an international audience, take questions, and save each video for future viewers. Their wide and comprehensive hour-a-piece lecture series is enjoyed my many and offers a free, no-hassle viewing experience. I was honored enough to be considered to give a talk on their channel, and after discussing more details with them, it appeared that there was a unique opportunity for some high-value topical information on laboratory and quality testing during this COVID-19 pandemic. If you haven’t heard of this series, you’re missing out. Please go like and subscribe to both their Facebook and YouTube platforms ASAP—you won’t be disappointed!
What’s a Good Test in a Pandemic?
Excellent question! You’ve probably already heard me talk about this before… This specific question came from discussions on social media with friend, colleague, and fellow ASCP Social Media Committee member Dr. Rodney Rhode (@RodneyRohde on Twitter). If I make it sound like I’ve been busy these last months, Dr. Rhode operates at another level: he’s publishing articles on the pandemic, running laboratory operations, is a research dean and department chair at Texas State, and is disseminating clinical information faster than I could even process it—he’s one of many pathology rockstars in our field! When we spoke before the PathCast series, we talked a bit about the problems in FDA fast-track clearance of all these new tests that would barely make the cut during non-pandemic “peace time.” The Emergency Use Authorization program allows the FDA to push forth tests available for commercial distribution with around 30 or so specimen validations that often don’t break the 60-70% sensitivity/specificity ceiling—yeah, I know. But it’s the best we’ve got and hospitals all over the country are working as hard as they can to bolster their validation studies with more specimens, better controls, modified protocols, and enhanced LDTs (laboratory developed tests) just to meet demand.

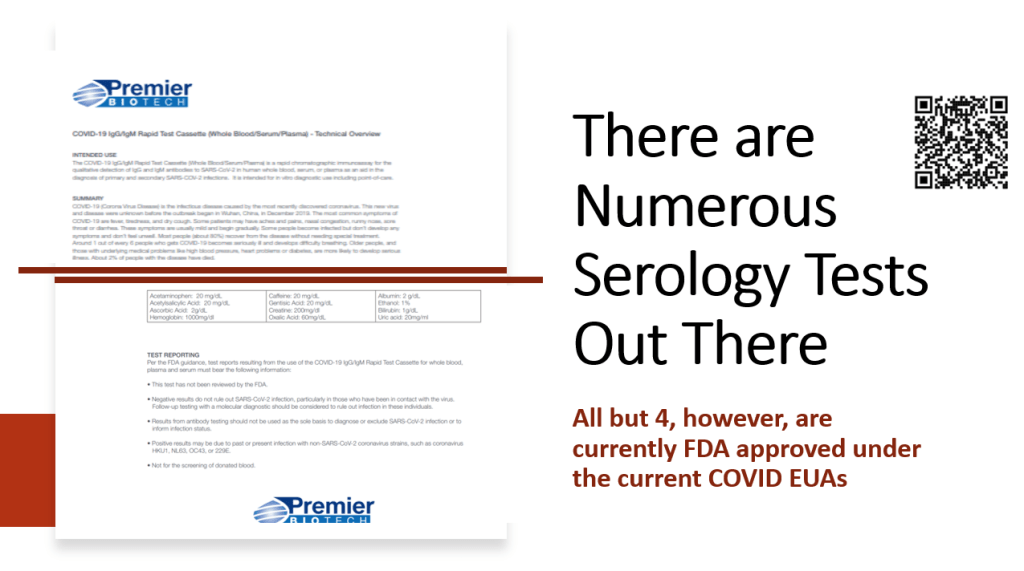
There are not enough tests, but there are also too many tests. Just before that PathCast lecture went live, I got an email from our awesome Lablogatory manager and editor, Kelly Swails (@kellyswails on Twitter) about some generic antibody testing kit that people were going nuts over. The problem was on page 6 of the manufacturers’ insert: “this test has not been reviewed or cleared by the FDA.” Well, there’s a problem—and they’re a dime a dozen. Since then, friends, colleagues, and all kinds of inquiries have come my way to ask, “is this a good test?” as people find kits available for purchase… it’s been a mess to say the least. But we laboratorians know: one of our core principles isn’t to let quantity overrule quality, especially when it comes to patient testing. That’s a non-starter.
NCTSTA
Shortly after the PathCast buzz started to settle, one of my MLS grad school classmates who now works with a local public health education and training organization in New Jersey, reached out to see if I could expand the discussion on testing to include problems with access and issues with vulnerable populations. Check and check. Go back and look at some of my posts on Zika and arbovirus work in the Caribbean and you just know I was excited to help! Proceed, Inc. has been a supportive community leader in addressing health and accessibility concerns in their local region and reaching out to form partnerships under the banner of the National Center for Training, Support, and Technical Assistance program (supported by the Centers for Disease Control and Prevention (CDC), Office of Minority Health (OMH), Administration for Children & Families (ACF), and other local entities.)
Who’s Vulnerable?
If you watch the news it’s individuals over 65 years of age and/or anyone with a significant related underlying condition: asthma, COPD, hypertension, etc. And, while that’s true, that’s just the tip of the vulnerability iceberg. Let’s remind ourselves for a minute about the inward and outward concepts of “social determinants of health.” When we want to label a population as vulnerable, or better put, increasingly susceptible to the negative effects of their living conditions in the setting of health care access, we have to think about all the things that contribute to a person’s health: their relationships, their stable/unstable living conditions, level of education, their income/expense ratio, possible language barriers, race/creed/color, disability, addiction, those experiencing homelessness, and concerns for their individual safety to name just a few! Inwardly, should we choose to engage these vulnerable communities we must do so with proper inclusion and a foundation of trust, communication, clarity of purpose, partnership, support, and—arguably most importantly—cultural humility. I also offered the attendees two resources as handouts which are available to you if you attend the recorded webinar as well: one COVID-19 safety factsheet directly from the CDC, and an adaptation of social determinants inventory I designed when my arbovirus team worked on Zika education in Sint Maarten. In truth, we’re all vulnerable in different ways, but when we work together to address gaps in delivery and access we end up #StrongerTogether—and that’s something our laboratory community knows a thing or two about!


The Tipping Point
The $64,000 two-part question: are things getting better or worse, and when will things go back to normal? My 64¢ answer: we don’t really know yet because there’s not enough active current data. The best estimates have case-peaks in places like Manhattan reaching a sort-of plateau as non-emergent hospitalizations, intubations, and COVID-19 cases slow down—but don’t mistake that for a full-on stop. Social distancing and quarantine initiatives in places like New York, Chicago, and other cities are the most effective NPI (non-pharmaceutical intervention) we’ve got. And that’s saying a lot. We have data that suggests previous pandemics had second waves as soldiers came back from war during the 1918 Flu pandemic in the states, so we’ve got to be careful and mindful of what we’re up against. But it’s getting easier and easier to become listless and bored of Netflix and stress-baking. People are getting legitimate cabin fever, although I’d rather we all had that than another, more topical viral illness these days. We’ve got a ways to go with all our frontline work, our NPI distancing, and stratified testing/tracking measures and we have to keep at it, otherwise we’ll undo all the progress we’ve made. And, that “new” vulnerable population, with motivations most certainly rooted in fear and stress, demanding to “reopen” the country since COVID is, after all, a hoax: don’t underestimate their power to tip the scales and send us back. The marriage of policy and politics is a patchy one at best, but efforts from professional advocacy societies like the ASCP are making strides, pushing both at the local and federal levels to demand active and appropriate responses to address proper COVID testing. But things don’t have to be so contentious.


Fear and Loathing vs. Love in the Time of COVID?
So where does this leave us now? You’ve listened to my litany of testing complexities and considerations for preserving quality of healthcare delivery to all types of patients and you know where I stand on having a passion for preserving the importance and integrity of our professional role as leaders in this field. Do we give in to frustration or keep fighting this pandemic in more, creative ways? The answer, to me, is obvious. We move forward, as always. But most especially, this lab week should be something different because it not only highlights our work as traditionally “behind the scene,” but underscores our critical importance to the delicate house of cards balanced between clinical healthcare, decision making, public health, and public opinion. It’s not only our job to make sure the tests are good (even during pandemics) but that we represent a consistent and reliable message of evidence-based truth for patients and clinicians to rely on—like we always do.
Happy Lab Week 2020. Stay safe, wash your hands, and remember social distancing doesn’t just mean staying at home. It also means integrating compassion into a new routine, and caring for neighbors, colleagues, and friends in new profound ways.
See you all next time!


-Constantine E. Kanakis MD, MSc, MLS (ASCP)CM is a new first year resident physician in the Pathology and Laboratory Medicine Department at Loyola University Medical Center in Chicago with interests in hematopathology, transfusion medicine, bioethics, public health, and graphic medicine. His posts focus on the broader issues important to the practice of clinical laboratory medicine and their applications to global/public health, outreach/education, and advancing medical science. He is actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Watch his TEDx talk entitled “Unrecognizable Medicine” and follow him on Twitter @CEKanakisMD.
