Hello again everyone! Last time on Lablogatory, I discussed the importance of patient advocacy and how it was especially poignant around the recent holiday season. We all have families, and sometimes those families and our medical professions intersect. Since then, I hope you’re all having a good start to the new year!
For me, the new year means a new start in medical school with clinical clerkships in New York City. Building off the theme I started last year, I hope to continue a message of patient advocacy through a laboratorian’s lens as I learn and navigate the clinical side of our field. My first such rotation is in a clinic serving a population with very significant statistics, both from the standpoint of laboratory data and epidemiology: HIV, hepatitis, and chronic infectious disease. As such, let me use this as a primer and explore what that really means for the patients in that community.
Now it’s no surprise that laboratory professionals like ourselves are deeply involved with public health efforts aimed at mitigating chronic/infectious diseases through screening, collaborating, and advancing technology. Last year I was fortunate enough to be part of the 2017 ASCP Annual Meeting in Chicago. Participating in sessions, and roundtable discussions, I was also able to listen to US Global AIDS Coordinator, Deborah L. Birx, MD had to say regarding ASCP’s global contributions to HIV/AIDS research and public health efforts. She spoke about resource limited laboratories and how ASCP has been an active and longstanding partner to the President’s Emergency Plan for AIDS Relief (PEPFAR), a global health initiative to address HIV/AIDS.


The relationship between laboratory data and epidemiology is evident, as results from screening and routine testing demonstrates both snapshots of evolving health statistics as well as progress in public health initiatives like PEPFAR. ASCP’s global initiatives reach all the way to Africa as those resource-limited laboratories gain support from telecommunications and shared materials. From rapid HIV tests with Western Blots, to Zika seroprevalence research, laboratory data and public health are dependent on each other. So how does this manifest in a place like New York, specifically the Bronx where my clinical rotations are located?
First, let me illustrate a snap shot of the scene in this New York borough. Something that demonstrates important data are a region’s social determinants of health—something I have found in my research and experience to be invaluable pieces of information when trying to address health concerns and influence outcomes with particular patient populations.

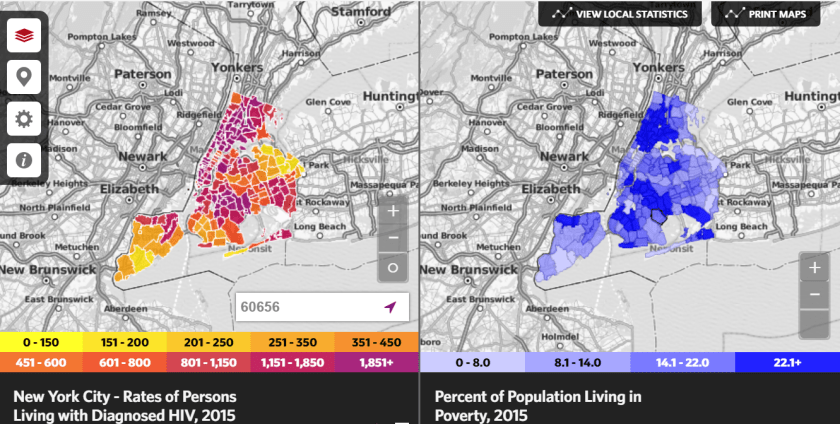
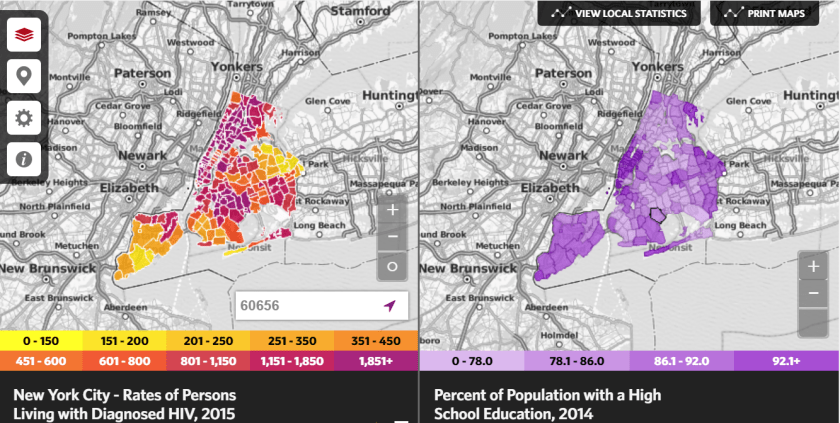


It’s clear to see here that the Bronx area has the most significant epidemiologic presence of active and new HIV cases. Parallel to this, the data demonstrates that the social determinants of health illustrated in Figures 2-5 are clearly correlative. More so, in the most recent report by the New York City Department of Health and Mental Hygiene (DOHMH) and the office of HIV Epidemiology and Field Services Program (HEFSP), data collected since 1981 from reported clinical encounters, viral loads, CD4 counts, and HIV genotypes reveal significant social health statistics. According to their 2016 NYC HIV/AIDS Annual Surveillance Statistics, the Bronx remains plighted with high numbers for HIV. It would appear as well, that regardless of HIV status, an overwhelming majority of the population (>71%) live in very high poverty—defined as >30% of the federal poverty line. According to data from Community Board 6, the local representation for the Bronx and specifically the zip code around my clinical site, the median household income is $24,537. A majority of this population is comprised of minorities as well, >40% Black and >40% Latino. The data differs slightly between men and women (including transgendered men and transgendered women) with regard to transmission risk. For men the highest risk factor continues to be sexual transmission between homosexual men, or men who have sex with men (MSM). For women, the risk stratifies to a high majority of heterosexual transmission (>70%). Read the full 2016 NYC DOHMH report here: https://tinyurl.com/ycf82xld. According to AIDSVu.org nearly 3,000 people out of 100,000 residing in the Bronx are living with active diagnosis of HIV/AIDS. The same source reports that between 2011 and 2015, the number of new cases approaches 200 annually.
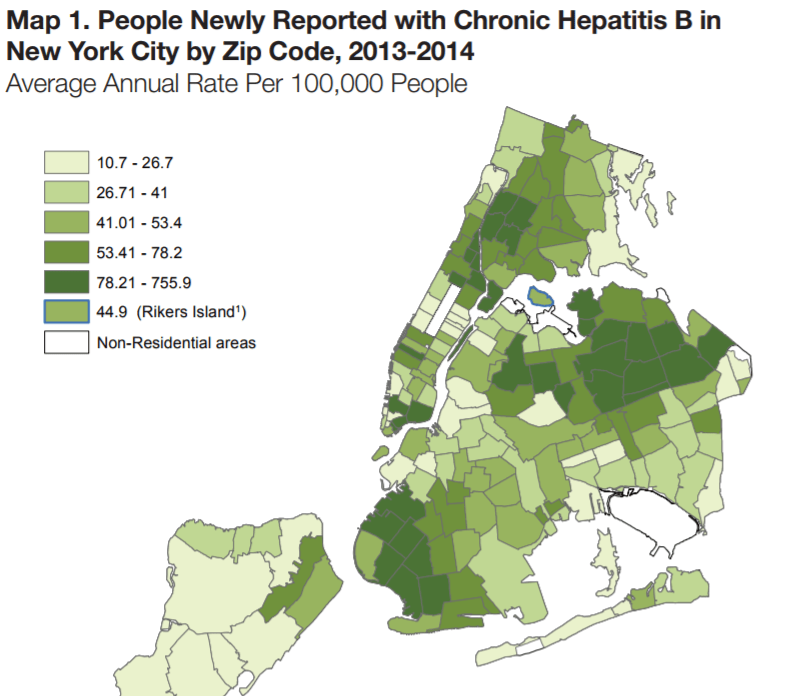
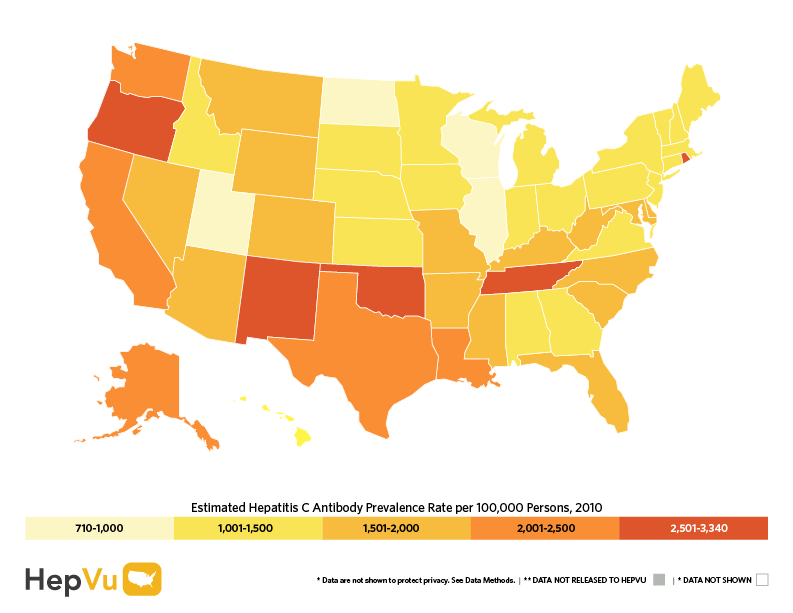
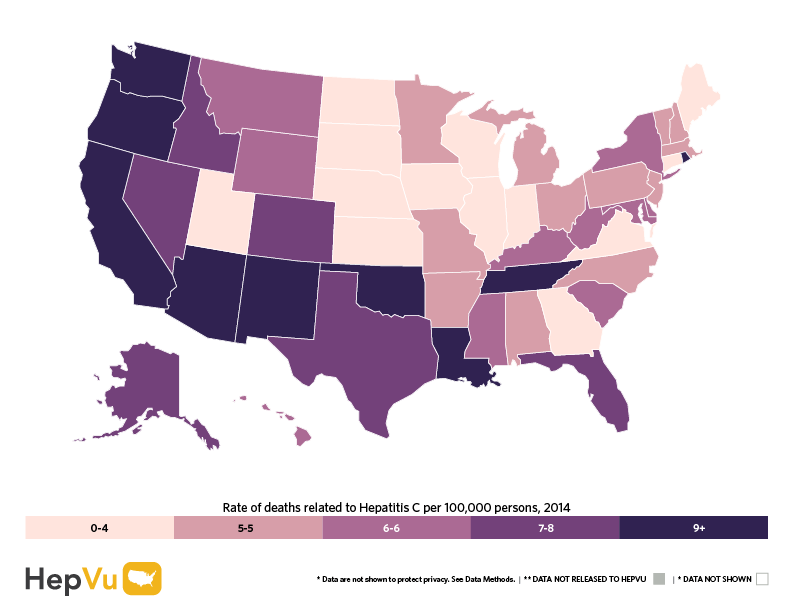
Another valuable function of the AIDSVu.org website is their HepVu.org companion site which provides incidence and infographic data about Hepatitis infections. The Hepatitis B and C Annual Report for 2014 published by the NYC DOHMH in 2016 also provides information about this chronic condition and how it affects the population. The maps below demonstrate that chronic Hepatitis is a serious and prevalent problem, and at a slight majority directly affects patients proportional to age.



But what does all this data mean? First and foremost it means progress. Progress for our patient populations because we’re busy tracking and keeping ahead of health statistics as they happen, and progress in our innovative ways to test earlier, screen better, and use the data wisely. None of this would be possible without the lab. From every hepatitis viral load, antigen immunoassay, and serology, lab data becomes translated to health data. And, all the while, clinical encounters with real patients experiencing real chronic illnesses are reported into epidemiologic data. Together we use those two sets of data to improve patient outcomes—I talked about that a lot with Zika in Sint Maarten.
I am honored to be at that bridge between the lab and the patient. Translating data back and forth from bedside to primary source is something that brings me a real sense of purpose. As part of this clinical rotation I will have to be involved in patient education, delivering presentations and conducting follow-up with those in the community who these public health messages are targeted to. So, instead of boring you some more with facts about lab science, testing/screening opportunities, and a promising future for those with chronic illness, I’ll go ahead and get a presentation ready for them!
Talk to you soon with some more in-depth clinical case-based blogging! Thanks for reading!

–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student at the American University of the Caribbean and actively involved with local public health.

great material,,,,,thank you for your time and effort.