Case History
A 6 year old male presented to the emergency department with a concern for ventriculo-peritoneal shunt (VP) malfunction. His past medical history is significant for myelomeningocele and hydrocephalus since birth. On arrival, symptoms included high fever (102.7°F), headaches and swelling at the VP shunt catheter site in the neck. Over the past week, his mother also noted nausea, vomiting and diarrhea. CT scan of the head revealed increased size of the 3rd and lateral ventricles which was concerning for either a VP shunt malfunction or infection. Lab work showed a white count of 13.5 TH/cm2 and elevated CRP values suggestive of an infection/inflammatory process. He was taken to surgery for VP shunt removal and placement of an external ventricular drain (EVD). Intra-operatively, purulent yellow material was noted at both the proximal and distal ends of the catheter. Cerebrospinal fluid (CSF) was sent for Gram stain and bacterial culture. He was started on vancomycin and ceftriaxone.
Laboratory Identification


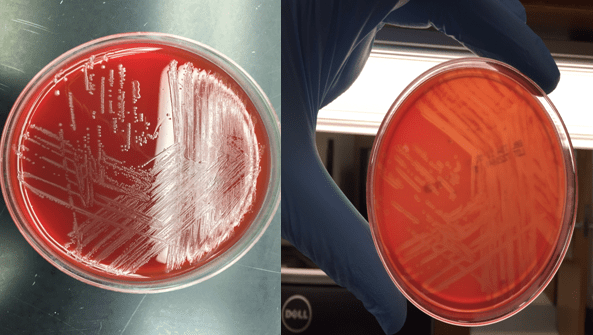
Bacterial cultures collected from a shunt tap and intra-operatively both showed short gram positive bacilli on Gram stain (Image 1&2). The organism grew on blood and chocolate agars as small, gray colonies with a narrow zone of beta-hemolysis when observed closely (Image 3) after incubation at 35°C in CO2. The isolate was positive for catalase and showed a “tumbling motility.” MALDI-TOF MS identified the isolate as Listeria monocytogenes.
Discussion
Listeria species are gram positive bacilli that grow as facultative anaerobes and do not produce endospores. The major human pathogen in the Listeria genus is L. monocytogenes and it is found in soil, stream water, sewage & vegetable matter and may colonize the gastrointestinal tract of humans and animals.
The most common mode of transmission is ingestion of contaminated foods, in particular, raw milk, soft cheeses, deli meats and ice cream. L. monocytogenes’ ability to grow at cold temperatures (4°C) permits multiplication in refrigerated foods. In a healthy adult, it causes an influenza like illness and gastroenteritis. Pregnant women are especially susceptible to disease and neonates infected in utero can develop granulomatosis infantiseptica which can lead to miscarriage, stillbirth or premature delivery. Elderly or immunocompromised can present with a febrile illness, bacteremia and meningitis (20-50% mortality).
In the microbiology laboratory, L. monocytogenes is usually identified via blood, CSF or placental bacterial cultures. It grows well on standard agars and after overnight incubation, the small, gray colonies show a narrow zone of beta hemolysis on blood agar. L. monocytogenes is positive for catalase & esculin and the CAMP test demonstrates block like accentuated hemolysis. It has characteristic tumbling motility at room temperature and an umbrella shaped motility pattern in semi-solid agar. Automated methods of identification provide reliable species level differentiation on the majority of current platforms.
Susceptibility testing should be performed on isolates from normally sterile sites. Ampicillin, penicillin, or amoxicillin are given for L. monocytogenes, and gentamicin is often added for its synergistic effect in invasive infections. Trimethoprim-sulfamethoxazole and vancomycin can be used in cases of allergy to penicillin. Cephalosporins are not effective for treatment of listeriosis.
In the case of our patient, after L. moncytogenes was identified, his antibiotic therapy was changed to ampicillin and gentamicin. Antibiotics were administered for 3 weeks before the placement of a new VP shunt. On further questioning, his mother revealed his diet consisted heavily of hot dogs and soft cheeses. She was educated on how to prevent subsequent infections prior to discharge.

-Jaspreet Kaur Oberoi, MD, is a Pathology resident at the University of Mississippi Medical Center.

-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the director of the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.
