Case History
A 57 year old male with a history of stage IA malignant melanoma presented with a new pink nodule on the right shoulder (see image provided) that has persisted for one month following a tetanus shot. Resultant specimen is a punch biopsy of the lesion.

Diagnosis
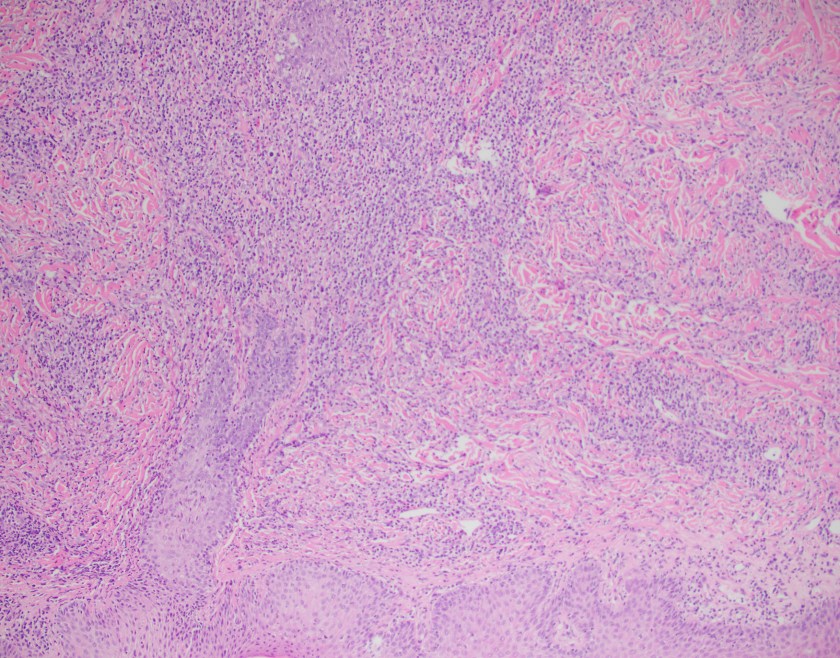
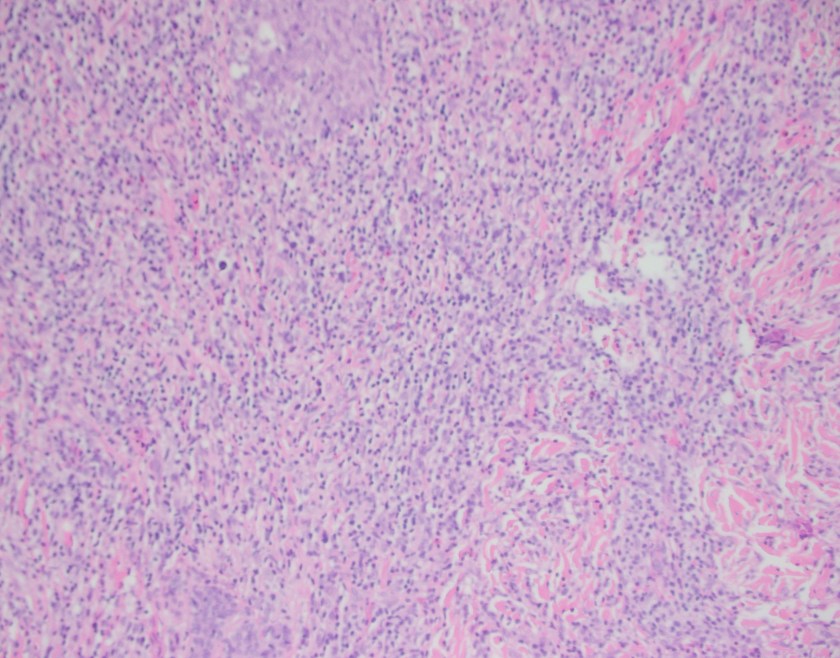
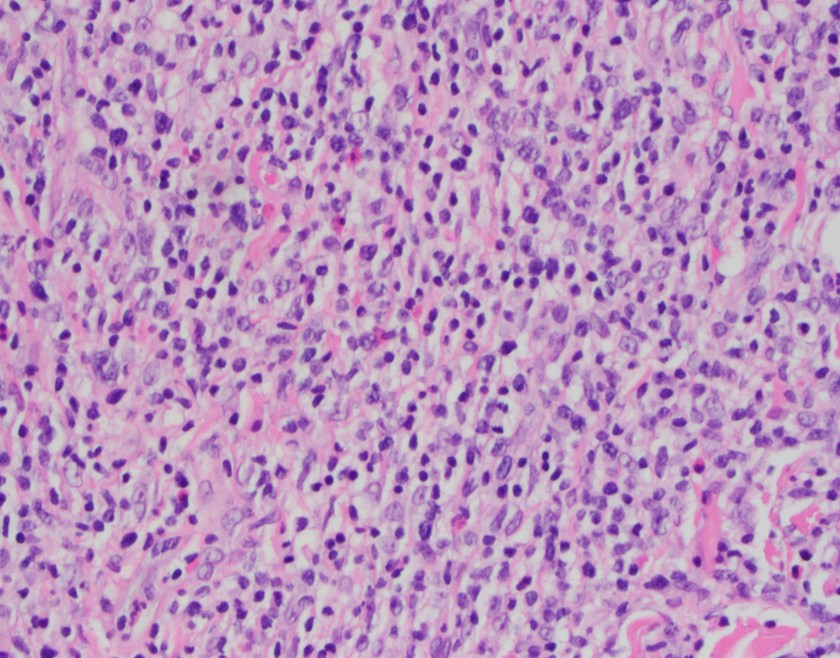






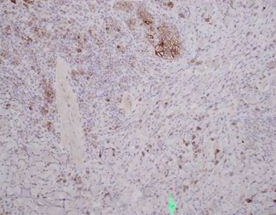
Sections show a punch biopsy of skin with a superficial as well as deep dermal infiltration of small and large lymphocytes. No epidermotropism is noted. An admixed background of inflammatory cells including eosinophils, neutrophils, and histiocytes is present.
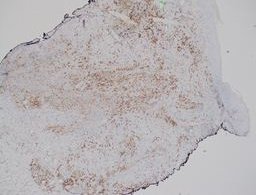
By immunohistochemistry, CD2, CD4, and CD5 highlight the abundance of lymphocytes indicating a dominant T-cell population. CD30 highlights a major subset of larger lymphocytes that co-express perforin. Granzyme is positive only in a small subset of cells. CD3 is present in a subset of CD30 positive cells indicating downregulation of CD3 in neoplastic cells. By Ki-67, the proliferation index is focally high (70%). CD20 highlights rare B-cells. CD8 is positive in a small fraction of T-cells. EMA is negative.
Overall, the diagnosis is that of a primary cutaneous CD30 positive T-cell lymphoproliferative disorder. The differential diagnosis includes lymphomatoid papulosis, type C and primary cutaneous anaplastic large cell lymphoma.
Discussion
Primary cutaneous CD30 positive T-cell lymphoproliferative disorders are the second most common cutaneous T-cell lymphoma (30% of cases). The primary groups within this entity include lymphomatoid papulosis (LyP) and cutaneous anaplastic large cell lymphoma.
Primary cutaneous anaplastic large cell lymphoma (C-ALCL) is composed of larger cells that are anaplastic, pleomorphic, or immunoblastic morphology that express CD30 in over 75% of the tumor cells. C-ALCL most commonly affects the trunk, face, extremities, and buttocks and often present as a solitary or localized nodules or tumors with ulceration. Clinically, the lesions may show partial or complete remission similar to LyP but often relapse in the skin. Interestingly enough, approximately 10% of cases may disseminate to local lymph nodes.
The histologic pattern of C-ALCL demonstrates a non-epidermotropic pattern with cohesive sheets of large CD30 positive T-cells. Ulcerating lesions may show a morphologic pattern similar to LyP with abundant inflammatory cells such as histiocytes, eosinophils, neutrophils with few CD30 positive tumor cells. By immunophenotyping, the tumor cells are CD4 positive with variable loss of CD2, CD5 or CD3 and express cytotoxic markers such as granzyme B, TIA1, and perforin. Unlike systemic anaplastic large cell lymphoma, C-ALCL does not express EMA or ALK.
The 10 year disease related survival of C-ALCL is 90%. Lymph node status or multifocal lesions does not alter prognosis significantly.
The differential diagnosis also include LyP, type C. These lesions often present on the trunk and extremities and are characterized by popular, papulonecrotic and/or nodular skin lesions. After 3-12 weeks, the skin findings may disappear. Up to 20% of LyP may be preceded by, have concurrent, or followed by another type of lymphoma such as mycosis fungoides (MF), C-ALCL, or Hodgkin lymphoma.1
Briefly, there are up to 5 types of LyP (types A-E).2,3 The more recently described LyP type D and E are determined by either simulating an epidermotropic aggressive CD8 positive CTCL and angiocentric and angioinvasive CD8 positive CTCL, respectively.
LyP has an excellent prognosis but since these patients may have other lymphomas, long term follow up is advised.
Overall, C-ALCL and LyP type C show considerable overlap both morphologically and clinically so close clinical follow up is recommended, however both demonstrate an excellent prognosis.
References
- Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC Press; 2008.
- Cardosa J, Duhra P, Thway Y, and Calonie E, “Lymphomatoid papulosis type D: a newly described variant easily confused with cutaneous aggressive CD8-positive cytotoxic T-cell lymphoma.” Am J Dermatopathol 2012 Oct; 34 (7): 762-765.
- Kempf W, Kazakov DV, Scharer L, et al. “Angioinvasive lymphomatoid papulosis: a new variant simulating aggressive lymphomas.” Am J Surg Pathol 2013 Jan; 37(1): 1-13.

-Phillip Michaels, MD is a board certified anatomic and clinical pathologist who is a current hematopathology fellow at Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA. His research interests include molecular profiling of diffuse large B-cell lymphoma as well as pathology resident education, especially in hematopathology and molecular genetic pathology.

Thanks for valuable case and review
Very interesting case, thank you for sharing with us!