Case History
A 63 year old man presented with a long standing history of a recurring pleomorphic adenoma of the parotid gland. As a child, the patient had radiotherapy to the bilateral parotid glands for parotid swelling. He then developed a left parotid mass ~15 years later and underwent parotidectomy. After another recurrence ~15 years after the initial parotidectomy, he underwent a second resection of multiple masses in the preauricular region. The patient then developed a recurrence ~20 years after the second resection and underwent neutron beam therapy. The patient tolerated the treatment well noting mild dry mouth, which is persistent, and left ear pain, but otherwise has no major long-term sequelae from the treatment. Eighteen years after the neutron beam therapy, the patient developed a left submandibular mass. A subsequent biopsy of the mass revealed a pleomorphic adenoma. Enlarged left and right submental and submandibular nodes were noted, with biopsies performed at an outside hospital of these nodes demonstrating metastatic poorly differentiated carcinoma within three lymph nodes. It was noted on this pathology report that the histological features, in light of the history, could represent a carcinoma ex pleomorphic adenoma. A CT scan of the head and neck revealed a large multiloculated, cystic, rim-enhancing mass within the left parotid gland, as well as large enhancing lymph nodes within the right anterior and posterior cervical triangle and the right submandibular space, the largest of which measured 2.1 cm. A PET scan showed increased activity within the right neck. Upon meeting with otolaryngology, a 4.0 x 7.0 cm lobular, non-fixed left parotid mass, and two level 1B right sided nodes, were palpated. Based on the patient’s history, physical exam, and prior biopsy results, it was decided to proceed with a parotidectomy and bilateral neck dissection.
Diagnosis
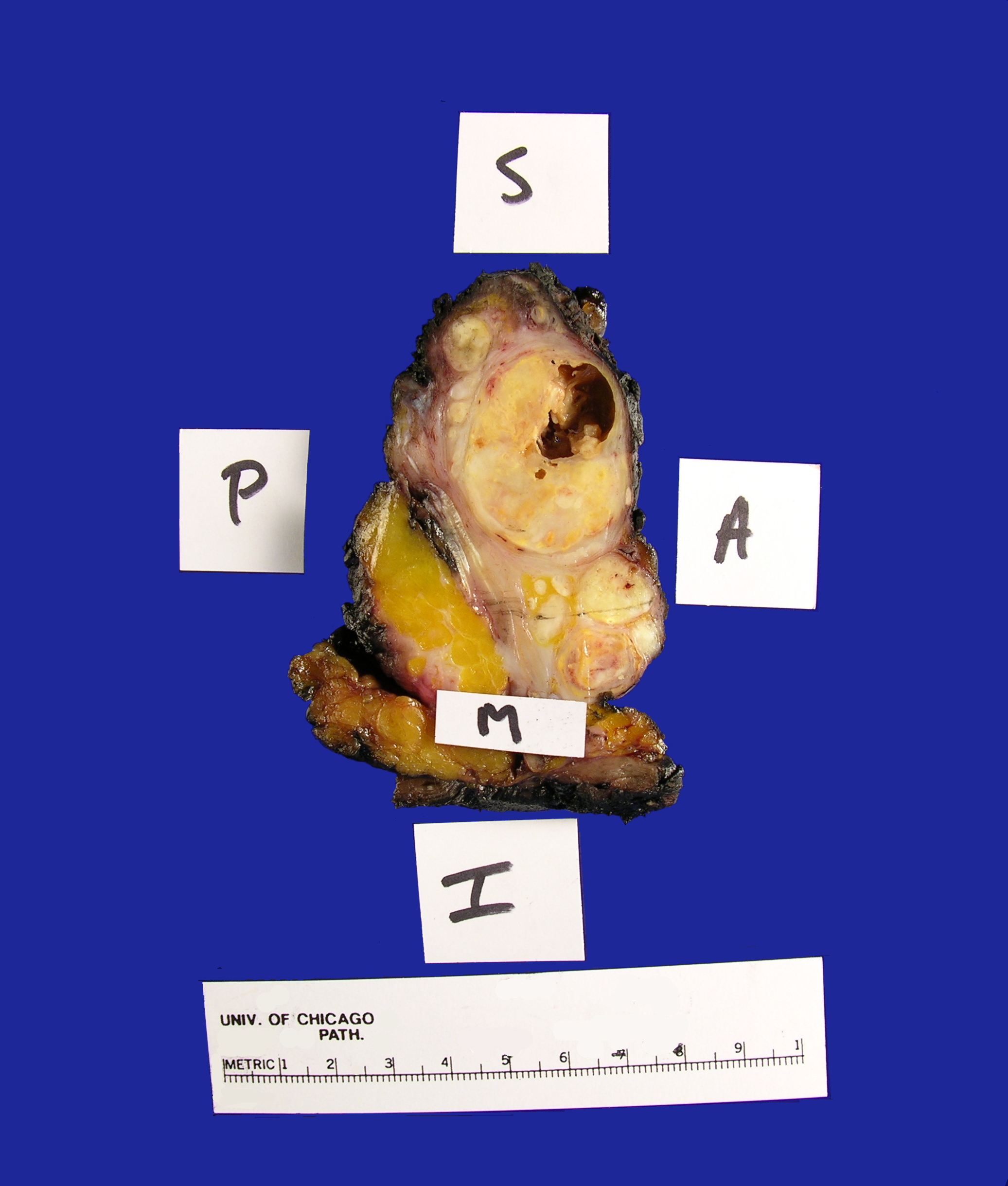
Received in the Surgical Pathology laboratory is a soft tissue mass resection from the area of the left parotid gland measuring 9.0 x 6.0 x 4.2 cm. The specimen is oriented by a single long stitch designating the superior aspect, and a double long stitch designating the lateral aspect (Figure 1). The specimen is entirely inked black, and then bisected to reveal multiple discrete, white-tan, partially cystic masses ranging in size from 0.2-4.0 cm in greatest dimension and measuring 7.0 x 3.5 x 3.0 cm in aggregate dimension (Figure 2). The largest mass is partially cystic with the cystic component measuring 1.2 cm in greatest dimension. This largest mass abuts the anterior, medial and lateral margins. The remaining tumor deposits are located:
– 1.2 cm from the inferior margin
– 0.4 cm from the superior margin
– 0.9 cm from the posterior margin
No gross salivary gland tissue is identified. The remainder of the specimen consists of unremarkable yellow adipose tissue and red-brown skeletal muscle. The specimen is submitted as follows.
Cassette 1: superior margin
Cassette 2: representative sections of anterior margin
Cassette 3: anterior superior margin
Cassette 4: anterior inferior margin
Cassette 5: posterior margin
Cassette 6-9: representative sections of mass with approach to lateral margin
Cassette 10: representative sections of mass with approach to medial margin
Cassette 11: mass in relation to surrounding skeletal muscle
Cassette12-15: representative sections of mass

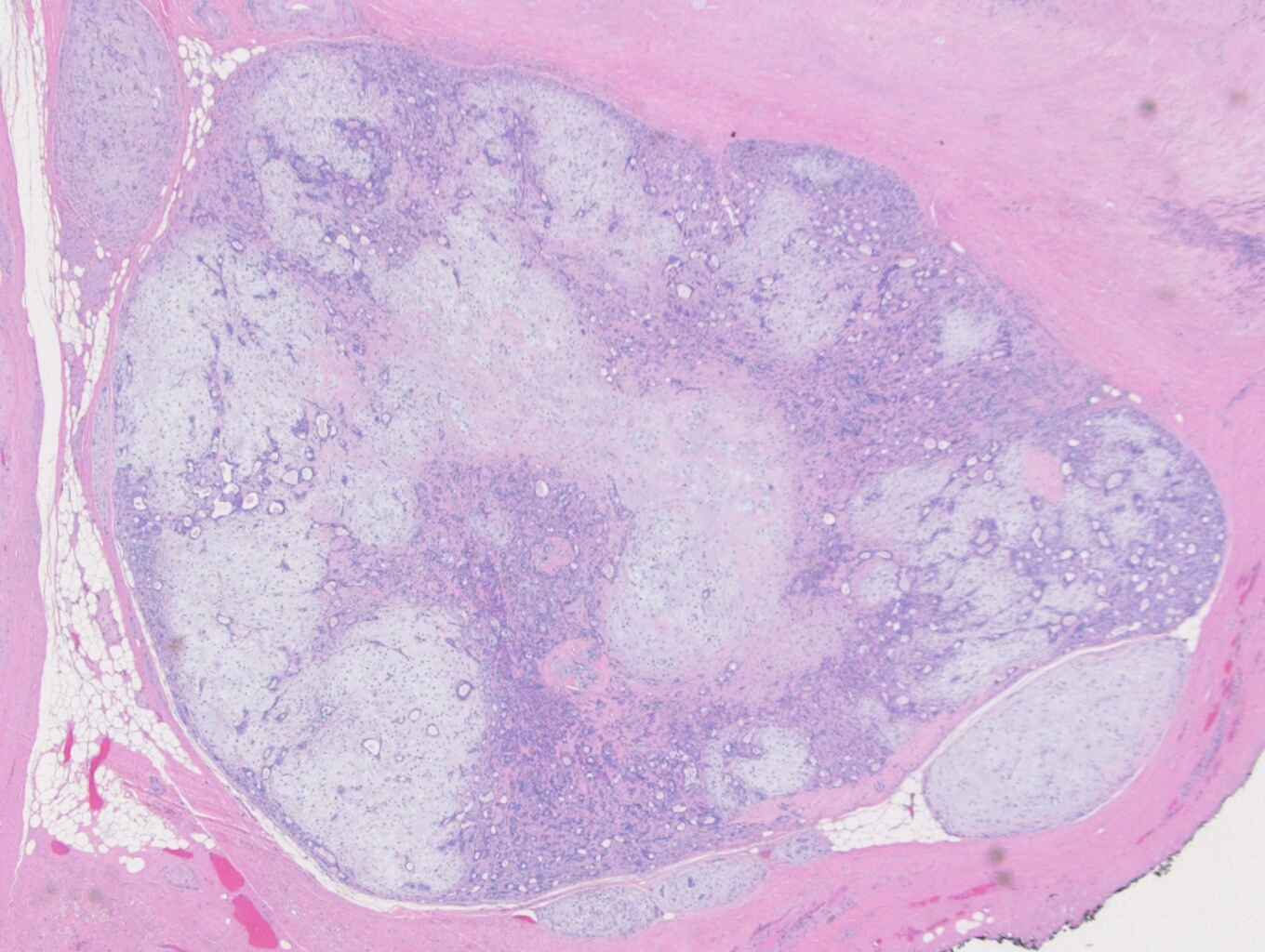
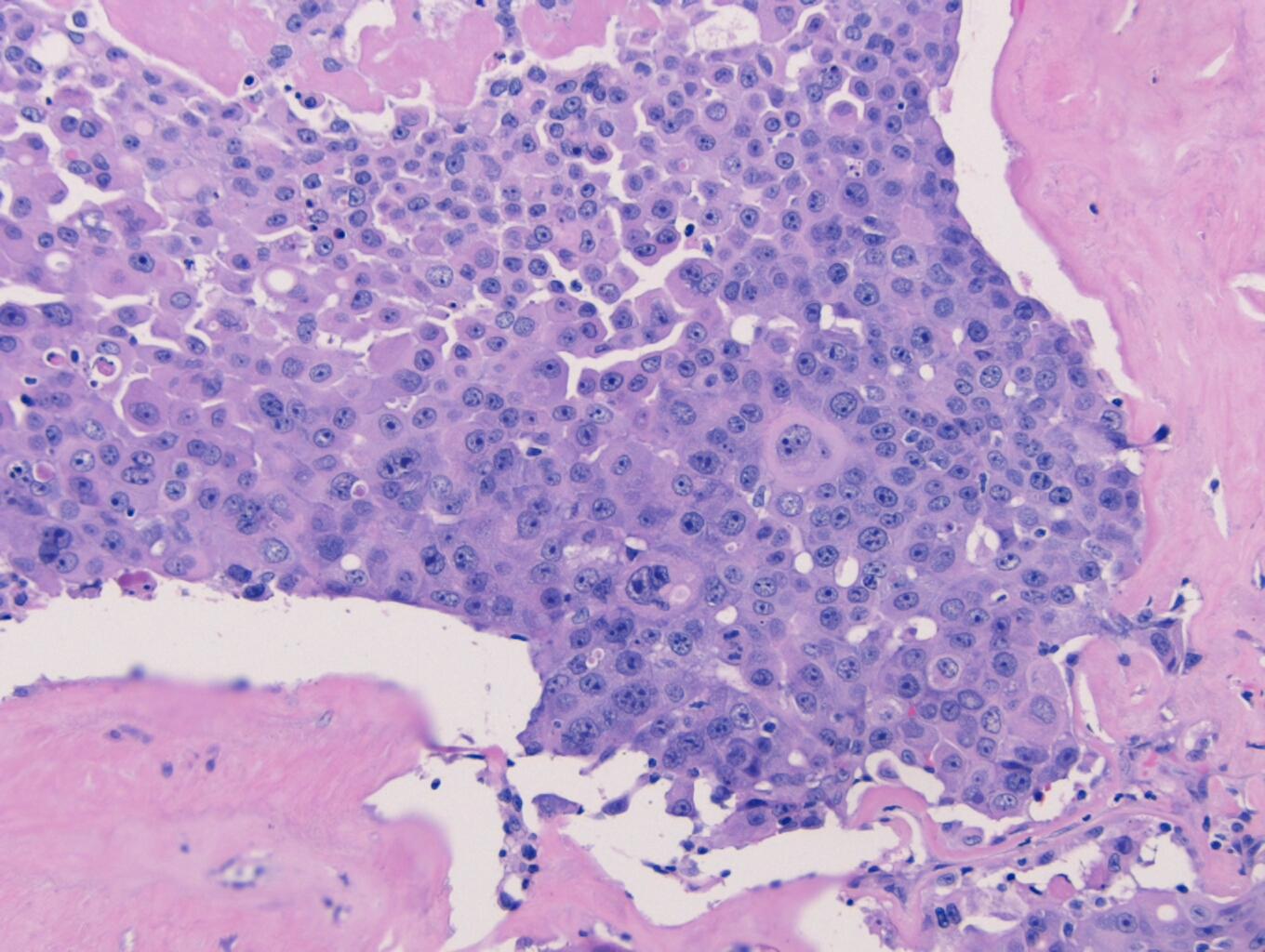
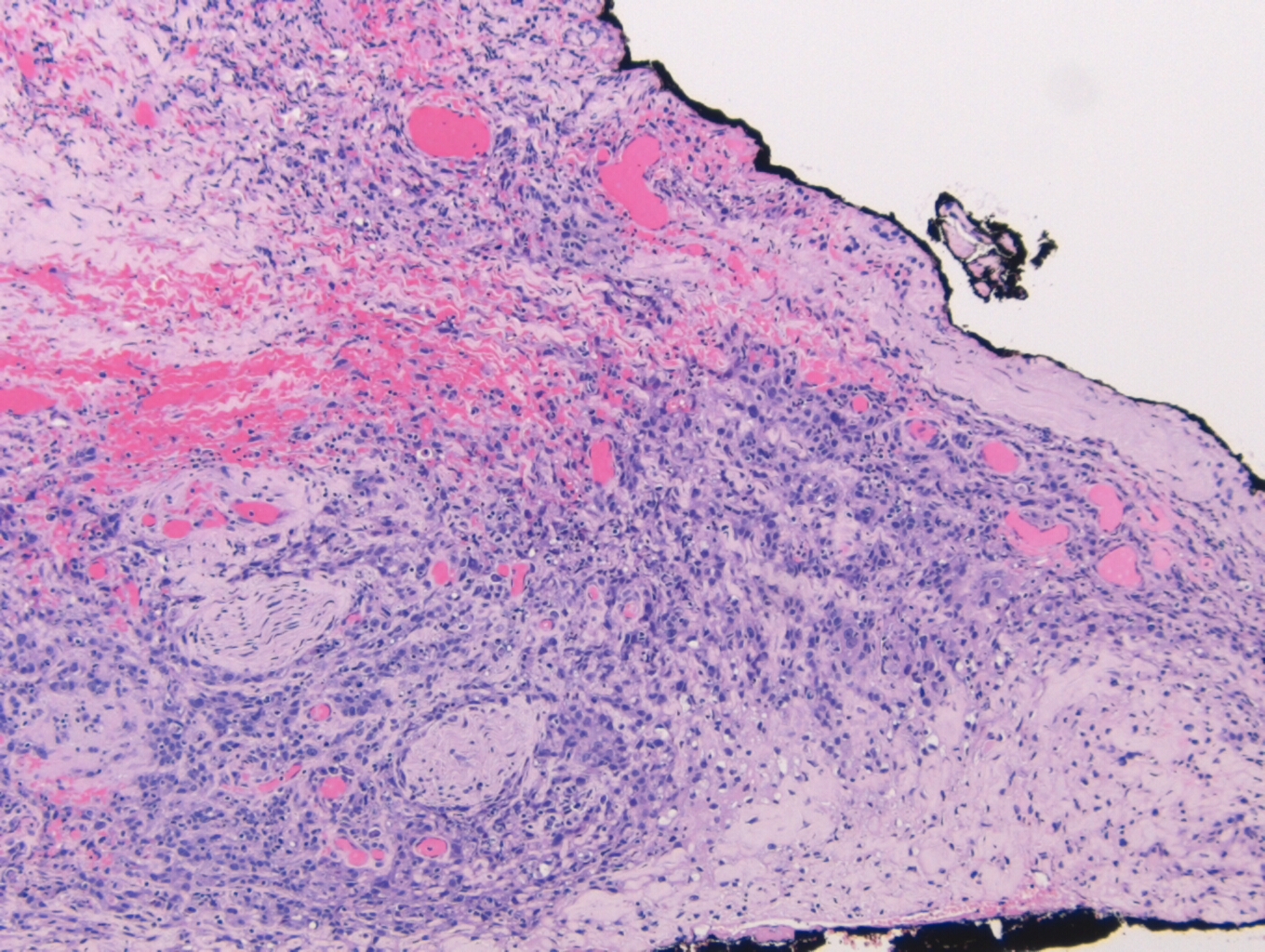
On microscopy, the specimen contains nests of tumor cells ranging in size from 0.2 to 4.0 cm within a dense fibrous matrix. Although these deposits may represent lymph node metastases, no residual lymphoid tissue is present. The tumor is represented by residual pleomorphic adenoma and numerous soft tissue deposits of pleomorphic adenoma (Figure 3). Admixed are broad areas of high grade carcinoma with necrosis (Figure 4). Most regions show adenocarcinoma, although a rare focus of squamous differentiation is also present. The lateral margin is positive for carcinoma, and a pleomorphic adenoma component approaches within 0.1 cm of the medial margin. The anterior, posterior, inferior, and superior margins are all free of tumor. No salivary gland tissue is identified.
In addition, eleven frozen sections are submitted from various areas surrounding the mass, with five of the eleven frozen sections demonstrating tumor deposits. A right neck dissection is performed with following results:
Level IB: 2 of 3 positive (largest deposit: 1.8 cm)
Level II and III: 1 of 14 positive, Level II (1.9cm)
Level IV: 1 of 8 positive (2.0 cm)
Based on these results, the specimen was signed out as carcinoma ex-pleomorphic adenoma, and designated as pT4aN2cMx
Discussion
Carcinoma ex pleomorphic adenoma (CXPA) is a carcinoma that arises in a primary (de novo) or recurrent benign pleomorphic adenoma (PA). While a PA is the most common salivary gland tumor, accounting for approximately 80% of all benign salivary gland tumors, a CXPA is quite uncommon, accounting for only 3.6% of all salivary gland tumors. CXPA is predominantly found in the sixth to eighth decades of life, with a slight predilection for females. CXPA arises most commonly in the salivary glands, in particular the parotid and the submandibular glands. CXPA can also arise in the minor salivary glands in the oral cavity, although these tumors tend to be smaller than their counterparts in the parotid and submandibular gland. There have also been cases of CXPA in the breast, lacrimal gland, trachea, and nasal cavity.
Clinically, CXPA presents as a firm, asymptomatic mass that can go undetected for years since they are not generally invasive. When the patient does experience any symptoms, with pain being the most common, it is usually due to the mass extending to adjacent structures. If the mass was to involve the facial nerve, paresis or palsy can occur. Other signs and symptoms include skin ulceration, mass enlargement, skin fixation, lymphadenopathy, dental pain, and dysphagia. The onset of symptoms can range anywhere from 1 month up to 60 years (such as with this case), with a mean onset of 9 years. Half of patients will have a painless mass for less than 1 year. Since these symptoms are similar to those of a benign PA, it’s important that the treating physician be aware of the possibility of a CXPA, especially considering the rarity of the cancer.
Grossly, CXPA appears as a firm, ill-defined tumor, and can vary greatly depending on the predominant component. If the PA is the predominant component, the mass may appear gray-blue and translucent, and it could be possible to grossly differentiate between the PA areas and the CXPA areas. If the malignant component predominates, then the mass may contain cystic, hemorrhagic and necrotic areas.
Microscopically, CXPA is defined as having a mixture of a benign PA, admixed with carcinomatous components. Zbaren et al, in an analysis of 19 CXPA cases, found 21% of the tumors were composed of less than 33% carcinoma, 37% of the tumors were composed of 33-66% carcinoma, and 42% of the tumors were composed of greater than 66% carcinoma. Most often, the malignant component is adenocarcinoma, but can also include adenoid cystic carcinoma, mucoepidermoid carcinoma, salivary duct carcinoma, and other less common variations. In cases where the entire tumor is replaced by carcinoma, the diagnosis of CXPA will be based on the presence of a PA on the previous biopsy. Conversely, you could also have a tumor that is predominately composed of a PA, with sparse areas of malignant transformation, such as nuclear pleomorphism, atypical mitotic figures, hemorrhage and necrosis. The likelihood of malignant transformation increases with the length of the PA being present, from 1.5% at 5 years, up to 10% after 15 years.
CXPA can be further sub-divided into four categories based on the extent of invasion of the carcinomatous component outside the capsule: in-situ, non-invasive, minimally invasive, and invasive carcinoma.
#1) In-situ carcinoma occurs when nuclear pleomorphism and atypical mitotic figures are found within the epithelial cells, but do not extend out beyond the border of the myoepithelial cells (Figure 5).
#2) Non-invasive CXPA, which can include in-situ carcinoma, is maintained within the fibrous capsule of the PA, but extends beyond the confines of the myoepithelial cells. Non-invasive CXPA may begin to show malignant transformation, but will overall behave like a benign PA.
#3) Minimally invasive CXPA is defined as <1.5 mm extension into the extracapsular tissue, with a mix of benign PA components and carcinomatous components.
#4) Invasive CXPA is defined as a > 1.5 mm extension into the extracapsular tissue, and will begin to demonstrate more carcinomatous components, such as hemorrhage and necrosis.
As the carcinomatous areas begin to increase in prevalence, the PA nodules will begin to be composed of hyalinized tissue with sparse, scattered ductal structures, and the malignant cells will begin to decrease in size as they move away from the site of origin. Perineural and vascular invasion can be easily identified as the tumor extends into the neighboring tissue (Figure 6).
The development of CXPA has been shown to follow a multi-step model of carcinogenesis with a loss of heterozygosity at chromosomal arms 8q, followed by 12q, and finally 17p. Both PA and CXPA demonstrate the same loss of heterozygosity, however, the carcinomatous components exhibit a slightly higher loss of heterozygosity at 8q, and a significantly higher loss of heterozygosity at 12q and 17q. The early alterations of the chromosomal arm 8q in a PA often involves PLAG1 and MYC, with the malignant transformation of the PA to a CXPA being associated with the 12q genes HMGA2 and MDM2.
Treatment for CXPA involves surgery, radiotherapy and chemotherapy, with a parotidectomy being the most common procedure performed. If a benign PA had originally been resected, but residual remnants of the PA were left behind, then satellite PA nodules will arise in its place (Figure 3). If in-situ, non-invasive or minimally invasive carcinoma is suspected in the superficial lobe of the parotid gland, than a superficial parotidectomy can be performed. Invasive carcinoma will result in a total parotidectomy, with every attempt made to try and preserve the facial nerve. If metastasis is suspected to the cervical lymph nodes, a neck dissection may also be performed. Reconstructive surgery following the removal of the tumor may be necessary, depending on where the tumor was resected from. Other treatment options currently being considered include a combination therapy of trastuzumab and capecitabine, as well as the possibility of a WT1 peptide based immunotherapy.
References
- Antony J, Gopalan V, Smith RA, Lam AK. Carcinoma ex pleomorphic adenoma: a comprehensive review of clinical, pathological and molecular data. Head Neck Pathol. 2011;6(1):1–9. doi:10.1007/s12105-011-0281-z
- Chooback N, Shen Y, Jones M, et al. Carcinoma ex pleomorphic adenoma: case report and options for systemic therapy. Curr Oncol. 2017;24(3):e251–e254. doi:10.3747/co.24.3588
- Di Palma S. Carcinoma ex pleomorphic adenoma, with particular emphasis on early lesions. Head Neck Pathol. 2013;7 Suppl 1(Suppl 1):S68–S76. doi:10.1007/s12105-013-0454-z
- Handra-Luca A. Malignant mixed tumor. Pathology Outlines. http://www.pathologyoutlines.com/topic/salivaryglandsmalignantmixedtumor.html. Revised March 21, 2019. Accessed April 5, 2019.

-Cory Nash is a board certified Pathologists’ Assistant, specializing in surgical and gross pathology. He currently works as a Pathologists’ Assistant at the University of Chicago Medical Center. His job involves the macroscopic examination, dissection and tissue submission of surgical specimens, ranging from biopsies to multi-organ resections. Cory has a special interest in head and neck pathology, as well as bone and soft tissue pathology. Cory can be followed on twitter at @iplaywithorgans.
