
Given my previous work in lab value changes in transgender individuals on hormone therapy, I was recommended to consider discussing the case of Olympic mid-distance runner, Caster Semenya. Although she is not transgender, this professional runner from South Africa has won her last 30 races and been scrutinized for her muscular build as having potentially higher levels of testosterone, a condition called hyperandrogenism. The International Olympic Committee’s (IOC) regulations require testosterone levels to be below a certain threshold for female athletes.
While no competitor can achieve great victories without hard work and practice, there are certainly examples of outliers whose genetics give them an advantage. However, I don’t think we would endorse shortening Michael Phelps’ arms or lobotomizing chess master Bobby Fisher to decrease their inborn advantages for a level playing field.
But this gets into an area of ethics that I’m not an expert on, so instead I will stick to my area of science and examine what evidence may exist to support the IOC’s policy. Then I will extrapolate the results from our study of transgender individuals to see if hormone regulation may impact contributions to athleticism. The most strongly shifted lab values in hormone therapy for transgender individuals are red blood cells (including oxygen-carrying hemoglobin) and creatinine (byproduct of muscle used to monitor kidney function, but also reflects total muscle mass).
Once looking more closely at this topic, I realized there is a lot to say about the contributions of 1) muscle mass and 2) red blood cells to athleticism. So, I will discuss muscle mass this month and wait until next month to discuss hemoglobin levels (including athletic performance by blood removal/ doping).
Mid-distance running, which is Caster Semenya’s sport, is a mix of anaerobic and aerobic activity. This means having more muscle would be advantageous. This is supported by a study that was commissioned by the IAAF (International Association of Athletics Federation), which shows a 1.8-2.6% increased competitive advantage in short distance track events (400m, 800m and, 400m hurdles)1. However, this study had several limitations. First, the sample size was quite low with only 22 female athletes. Next, they use a p-value of 0.05 for significance without correction for multiple hypothesis testing (21 hypotheses tested representing each event), which increases the likelihood of a false positive result by chance.
What makes me curious is whether following the International Olympic Committee’s recommendations of lowering testosterone levels would even have a meaningful impact and improve competitiveness?
From my research, I know that adding testosterone to individuals assigned female at birth to transition to transgender males (TM ) does substantially increase creatinine (p<0.005, Figure 1)2 to male levels (baseline TW). This is likely not due to changes in kidney function (although this has not yet been proven), but rather due to increased muscle mass.
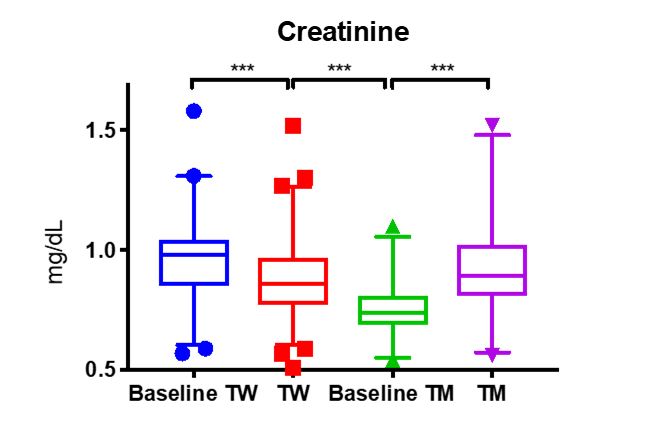
However, the inverse is not quite true for transgender women who take combinations of estrogen for feminization and spironolactone to block the effects of testosterone. In these patients, we see a slight decrease in the creatinine (TW). While this decrease is statistically significant, the range is not clinically different from male creatinine levels. This concurs with the observations that musculature in transgender women does not change substantially upon taking hormone altering medication.
A more rigorous examination of muscle mass, performed by MRI measurement, determined that after 1 year of hormone therapy testosterone increased muscle mass in transgender men to biological male levels3, similar to our observations of creatinine. Further, they saw a significant reduction in muscle mass from baseline of transgender women on hormone therapy for 12 months, but it was still much higher than the muscle mass of biologic females4.
Therefore, were Casten Semenya to take testosterone blocking medication, I suspect there would be little impact on her overall muscle mass. Which is one of, if not the explicit purpose of taking testosterone lowering medicine. The strength of my conclusions is limited by the fact that we don’t know Casten Semenya’s testosterone levels, and furthermore a hyperadrogenic female is not the same as a male-to-female transgender woman.
As mentioned above, I will continue this discussion next month with an exploration of how testosterone lowering therapy could affect red blood cell levels, which would affect athletic performance differently.
References
- Bermon S and Garnier P. Serum androgen levels and their relation to performance in track and field: mass spectrometry results from 2127 observations in male and female elite athletes. British Journal of Sports Medicine. 2017; 51(17): 1309-1314.
- SoRelle JA, Jiao R, Gao E et al. Impact of Hormone Therapy on Laboratory Values in Transgender Patients. Clin Chem. 2019; 65(1): 170-179.
- Gooren LJ, Bunck MC. Transsexuals and competitive sports. Eur J Endocrinol. 2004; 151(4): 425-9.
- Jones BA, Arcelus J, Bouman WP, Haycraft E. Sport and Transgender People: A Systematic Review of the Literature Relating to Sport Participation and Competitive Sport Policies. Sports Med. 2017;47(4):701-716.

-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and advancing quality in molecular diagnostics.
