Maryam Zenali1*, Dmitriy Akselrod2, Eric Ganguly3, Eswar Tipirneni4 and Christopher J. Anker5*
1
Department of
Pathology, 2 Department of Radiology, 3 Division of
Gastroenterology, and 5 Division of Radiation Oncology, The
University of Vermont Medical Center (UVMMC), Burlington, VT and 4
Department of Hematology Oncology, Central Vermont Medical Center (CVMC), The
University Of Vermont Health Network, Adult Primary Care, Berlin, VT
*corresponding authors
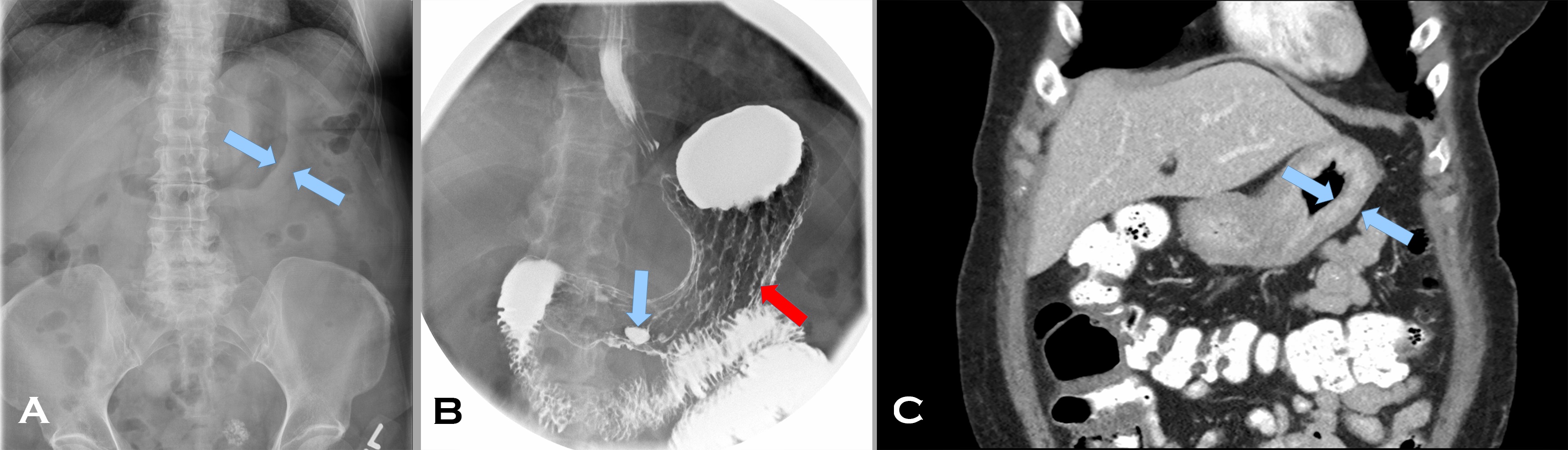
A 57 year old woman with a personal and family history of breast cancer presented with early satiety and dysphagia for 5 months. Her abdominal computed tomography (CT) scan (Image 1 A) showed marked thickening of an apparently featureless gastric wall (A, blue arrows indicating the mucosal [rightward pointing] and serosal [leftward pointing] aspects of the gastric wall). Prominent gastrohepatic lymph nodes were noted as well. Her fluoroscopic upper GI study (Image1 B), following administration of barium and effervescent crystals (a double contrast effect to allow for mucosal evaluation), showed thickened rugal folds (B red arrow) and pooling of barium within an antral ulcer (B blue arrow). A subsequent CT scan (Image 1 C) after administration of intravenous and enteric contrast, confirmed marked diffuse gastric wall thickening (C blue arrows again indicating the mucosal [rightward pointing] and serosal [leftward pointing] aspects of the gastric wall) (Image 1, composite radiographs A-C).
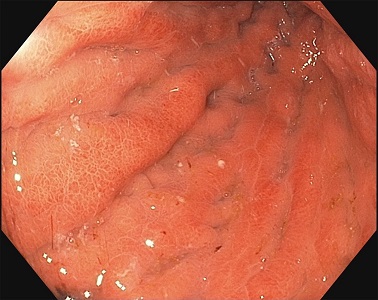
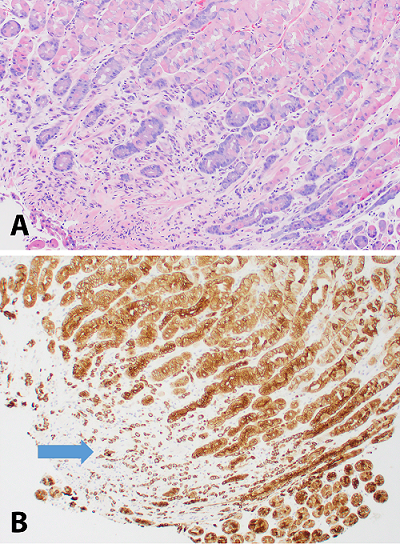
The gastric body distended poorly with insufflation and demonstrated thickened, erythematous, edematous folds with erosions (Image 2, endoscopy image). On endoscopic ultrasound, the total thickness of the stomach was 12 mm with expanded wall layers in the proximal stomach to the antrum and a thickness of 3.5 mm in spared areas. Biopsies were obtained; the corresponding H&E and keratin stains are provided (Image 3, composite photomicrographs A-B).
Image 1. Composite radiographs.
Image 2. Endoscopy image.
Image 3. Composite photomicrographs.
Based on the original radiographic imaging that led to the biopsy, what are the differential diagnoses?
Image 1. Looks like this medical lab science blogger made quite the … shady… joke. CSI: Miami’s Lt. Horatio Caine (played by David Caruso) donned his shades at pivotal plot times. (Source: CBS)
Okay-okay, I couldn’t resist that. How many times have you
just wanted a CSI-style joke on here?
No? Just me? That’s fine…
Hello again everybody! Welcome back! Last month I talked a
bit about “Just
Culture,” a sort of bridge between the values we tout as clinical leaders
in our laboratories and the medical culture’s evolving and value-informed
paradigm shift. There was a little in there about the lessons paralleled in LMU
and the benefits of interdisciplinary teamwork. This month, on the subject of
interdisciplinary collaboration, I’d like to talk about our colleagues who often
are secluded or in more remote areas in our hospitals, offices, and academic
centers. Not here to stereotype; I’m talking about our friends in forensic
pathology!
Before I get there, let me go back a bit. I’ve already written several times about the stereotypes that surround our field of lab medicine and there are two times when that is glaringly present: when you’re a medical student or when you’re in forensics. I got the chance to meet someone who falls into both categories.
I’ve just finished up my OB/GYN rotation. But before my last
day, I went to the lab at our hospital and followed up on some pending biopsy
results. Okay, I can’t lie to you guys: they wanted me to see if I could rush
“my lab friends” to expedite the process of fixing, setting, cutting, staining,
and reading/reporting—because that’s
possible. So, I went to the lab and had a pleasant chat with the staff
explaining the situation and they were happy to help. While I was there,
however, I happened to see another short white coat (ironically from my same
school) who was helping some lab personnel with some grossing. Turns out she
wants to match into a pathology residency—just like me—and specifically was
interested in forensic path, a field which I don’t know much about. After talking
more, I asked if she’d like to share some information. Here’s my conversation
with Kyla Jorgenson, a 3rd year medical student at AUC-SOM from
Toronto, Canada:
I get lots of hassle
when I say I want to become a pathologist. People often ask me, “what’s your
back up choice” or “don’t you like patients?” It can be a challenge. What’s
your experience been like?
You want to do autopsies, so you want to be a
mortician, right? Not quite. Many times, I’ve been faced with blank stares when
I say I want to be a forensic pathologist. Other times I get the other end of
the spectrum, that’s so cool! Clearly, they’ve seen a few crime-shows and think
that I’ll get to go to crime scenes in stiletto high heeled shoes with a song
by The Who playing in the background as I arrive. Even today when talking with
a dermatopathologist I got a, “well when you realize that hanging out with
dead bodies every day isn’t the greatest, you might consider surg path.”
Then after hearing my experience as an autopsy assistant and that I’m sure this
is what I want to do it was the resigned sigh signalling that I was a lost
cause already.
A “lost cause,” that’s
frustrating. A lot of specialities rag on other ones, it seems to be part of
the culture of medicine—hopefully not forever, but still can’t we all just get
along?
So, my background
leading to pathology involved me working for several years between college,
graduate school, and medical school; in hospitals of various sizes. I have
personal experiences in these fields and sort of feel “at home” when I’m
dealing with hematopathology, transfusion medicine, cell therapy—that sort of
thing. What piqued your interest in forensics?
I started my undergraduate degree in forensic
biology at the University of Toronto in the fall of 2008 just as a major review
of pediatric forensic pathology in Ontario was being released. After numerous
issues came to light, the inquiry looked at policies, procedures, practices,
accountability and oversight mechanisms, quality control measures and
institutional arrangements within the field in Ontario from 1981 to 2001. Ontario
Court of Appeal’s Honourable Justice Stephen T. Goudge developed 169 recommendations
on how pediatric forensic pathology in Ontario needed to address and correct
its systemic failings to restore public confidence.
After studying the cases that prompted the
inquiry and its recommendations in class, what left the greatest impression was
the importance of having medicolegal autopsies performed by those trained in
not just pathology, but specifically, forensic pathology. What I took away from
the cases of accidental deaths falsely attributed as homicides due to lack of
experience on behalf of the pathologist and other such issues, is that forensic
pathology isn’t something to be dabbled in. While our patients are no longer
alive, there are lives that can be affected by the work we do. In Ontario,
false convictions not only stemmed from “junk science” but also from
inadequacies in the training of pathologists working in a forensic capacity and
also a general shortage of forensic pathologists.
Seems like a lot of us
(of the few of us) who enter medical school knowing we want to go into
pathology have to sort of wait their turn, as it were, collecting experiences
which help make us competitive for residency matching—what keeps your
“commitment algorithm” going?
Since discovering that forensic medicine is a
career path as a high school student, I’ve geared my education towards training
in forensics. First my undergraduate degree and then a side trip for my master’s
degree in Forensic Death Scene Investigation and a job as a pathology
technician at the Medical Examiner’s office on my way to medical school. I have
in each step along the way, confirmed that both medicine and forensics
fascinate me. Scroll through my Netflix account and you’ll find crime dramas
(with the British shows being my favourite) or my podcast app filled with true
crime shows; I am enraptured using science to figure out what happened.
Sidebar: at this point Kyla showed me a first-author published piece in
the Journal of Forensic Sciences from
2017 that talked about law enforcement-involved firearm related deaths in
Oklahoma, where she worked at the time. Basically, it showed through metadata
analysis that gun-related deaths were on the rise. Not just over time, but
number of times being shot. Remember when we talked about pathology’s role in
the #StayInYourLane/#ThisIsOurLane discussion? Well which pathology
speciality do you think works with this stuff directly? Chemistry? Cytology?
Last time I checked GSWs don’t get screened for lead poisoning and you can’t
FNA a bullet. Forensic pathology has often been tasked with seeing trends in
morbidity and mortality and translating that to effective social and public
health change: think seatbelts, stents, and maybe someday gun-related
legislation changes.
Image 2a. Monthly aggregates of gun-related deaths over a 16-year period in OK. (Source: Jorgenson, K et al (2017) Trends in Officer-Involved Firearm Deaths in Oklahoma from 2000-2015, Journal of Forensic Sciences, doi: 10.1111/1556-4029.13499)Image 2b. Number of gun shot wounds per victim over time. (Source: Jorgenson, K et al (2017) Trends in Officer-Involved Firearm Deaths in Oklahoma from 2000-2015, Journal of Forensic Sciences, doi: 10.1111/1556-4029.13499)
I was interested when
I shadowed at the Cook County ME’s office a few years ago—I saw some cool
things. I also remember learning a lot from the first real autopsy I saw in a
hospital, ultimately it seems like a totally different field that maybe gets
underappreciated even within the pathology umbrella. AP/CP residents have to do
a certain number of autopsies to graduate, but the attitude I’ve noticed around
the topic is a “necessary evil” and most are working towards not having to do
that. So let me ask you definitively, why forensic pathology?
Medicine is science being applied to find out
what happened in the body and how we can change or manipulate those variables
to diagnose, prevent, treat and manage disease. Each diagnosis is solving a
crime occurring within the cells in the body, if you will. In forensic
medicine, not only do you get to do all that but add in the crime solving
element and you get to be “Dr. Nancy Drew.” While medicolegal systems are
different all over the US and Canada, chances are that as a forensic
pathologist you won’t only be working on your stereotypical
“forensics” cases, the gunshot wounds, stab wounds and other
nefarious causes of deaths many associate with that term. You could get the
generic, “cause of death atherosclerotic cardiovascular disease, manner of
death natural,” for a large proportion of cases.
It’s not glamorous, you could spend your day with a two-week-old decomposing decedent that has a pulsating maggot mass devouring its torso or documenting 51 stab wounds or signing out your cases after reviewing your histology and toxicology reports or testifying on a homicide case you worked on. But for me, those all sound like pretty interesting ways to spend the day, sign me up. As a pathology technician assisting with the autopsies and external exams, I was never required to think about what was happening in the body, but I wanted to understand it all. Now as I progress through medical school and look towards residency and fellowship, I eagerly await the chance to perform my first autopsy as a physician, to put all the knowledge and experience I’ve gained towards helping move Ontario and forensic pathology forward.
Image 3. Kyla M. Jorgenson is a 3rd year medical student at the American University of the Caribbean School of Medicine with prior undergraduate and graduate studies in the field of forensic pathology, professional experience as an autopsy technician, as well as a vested interest in pursuing a career in the field moving forward in residency and fellowship. (Source: Kyla M. Jorgenson)
I’d like to thank Kyla for her time in talking with me and
her willingness to share her insights with all of you. I wish her all the best
of luck as she continues through her training with electives and core rotations
both in the UK and state-side. If you have any questions to relay to her,
please feel free to comment below and I will forward appropriately. And as
always, don’t forget to share with your colleagues across every discipline!
Thanks for reading, I’ll see you next time where I’ll be
writing from the Mayo Clinic Hospital in Rochester, Minnesota, conducting a
formal rotation in Anatomic and Clinical Pathology! Don’t miss it, I’ll have
lots to share while learning at one of the nation’s top institutions!
Until next time!
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola
University Chicago with a BS in Molecular Biology and Bioethics and then
Rush University with an MS in Medical Laboratory Science. He is
currently a medical student actively involved in public health and
laboratory medicine, conducting clinicals at Bronx-Care Hospital Center
in New York City.
As with most clinical situations, there is often more going on than you can see on the surface. The classic example being the lab values that might have derangements that aren’t apparent clinically; something we rely on heavily in medicine. While most of the situations in these cases apply to diagnostic methods in patient care, sometimes those nuances exist outside of patient care. For example, a simple comment or phrase can hint at an individual’s potential biases and/or carry with them a weight of opinion that means more than what it sounded like.
Image 1. Emerging from their laboratory, a pathologist, lab manager, and shift supervisor arrive ready to discuss clinical lab metrics with hospital administration. Many of us transform our roles within and outside of the lab, creating a complex team of clinicians all for the sake of our patients. (Source: Transformers: The Movie, obviously)
Image 2. Instruments get routine service visits from industry reps, while supervisors oversee, and bench techs commiserate all in matching lab coats. Laboratorians often enjoy the exclusivity of the laboratory, working mostly “with your own” can sometimes facilitate an easier experience. But beware of comfort zones: if you don’t spend your time learning about others’ scopes, they won’t learn about yours. (Source: The Simpsons)
Last January, I brought up the topic of stereotypes in pathology which seem to reflect common misconceptions about the field of laboratory medicine. This time I think I’d like to explore that topic a little more in-depth, as I’ve noticed a few things during my clinicals as a medical student. Those of us with careers or histories of lab work or pathology experience know that we’re mostly regarded as a “behind the scene” crowd. That can be true, and to a certain extent a necessary part of patient care, but what happens when these stereotypes catch up with you? What happens when they become a part of your training? Since I have the great luck to have been on both sides of this question, here are my thoughts on what it really means when lab folks are thought of as a mysterious secret hospital-basement society.
First of all, these stereotypes aren’t anything new. We’ve all been sharing and resharing the same story every couple of years from article to article. I shared a few last January: Dr. Lori Rasca’s “Lonely Life of a Clinical Pathologist,” Dr. Sarah Riley’s call to bring the lab to the forefront of medical practice, and survey after survey about things like burn-out and wages. Go ahead and google things about careers in pathology and you’ll get a mixed bag. Often times, you’ll see programs or departments tout the importance of a profession in clinical pathology. Yale University School of Medicine conducted a survey last March where they asked middle-school students “what does a pathologist do?” The responses varied—and were mostly wrong. So the department wrote a piece about the clinical roles of those in laboratory medicine addressing specialization, patient contact, and tech-innovation. One line that stuck out to me: “[you’ll] sometimes hear a surgeon say, ‘I’m only as good as my pathologist.’” Fantastic, I wrote about that last June where I talked about how the relationships between surgery and pathology are critical. The fact of the matter is, pathology is always changing; and with it, the roles of pathologists do too. An article from April 2011 in the College of American Pathology’s CAP Today featured Dr. Sylvia L. Asa and she wrote at length about the future of pathology in response to current stereotypes:
“The 2020 pathologist should not be someone who hides in the basement of a hospital and looks at glass slides or even whole-slide images, but someone who’s able to take all the information from the clinical pathology lab, from radiology, from endoscopy, from slides and the molecular lab, and sit down with the patient to explain the disease he or she has. That is how we will stay relevant in the public eye and every patient will know who their pathologist is. And we should make sure that the patient’s pathologist is the person who, when the patient searches the Internet, is an expert in the field.”
Next, medical students experience a myriad of sifted and specialized knowledge which changes scope and tone from one month/service/attending to another. When you’re in internal medicine, ID specialists are lazy; when you’re in surgery, IM residents are flustered; when you’re in ED, the other attendings don’t have as many thrilling stories; and when you’re in clinic with family medicine staff, you know no one else can handle the “front lines” like you guys do…right? Basically, everyone has a point of view and we naturally find ourselves working with other professionals who have specialized in the same field as us. But when you get too comfortable with your homogenous staff, that’s when those (otherwise normal) opinions can get complicated. Most of the time, pathology is viewed as an outsiders’ specialty. People might think you’re socially inept, or don’t like patients, or even can’t “cut it” on the wards. (That was harder for me to type than for you to read, trust me.) But it does happen; and when it becomes a conversation piece, med students have two classic options: Smile and agree with everything your attending says because their word is gold and they ultimately sign your evaluations or take the chance to address misconceptions and stereotypes—which do you think is easier? Earlier this year, a medical student from Ireland named Robert Ta wrote about his path to pathology in an article published in the International Journal of Medical Students (yes, it’s a real thing—and it’s great!). In it he discussed his enlightening experiences observing laboratory medicine for the first time and falling for the interdisciplinary work and diagnostic algorithms pathology offers. He even cited all-too-familiar classics we’ve all heard such as ““you must really hate dealing with people,” “[you must] have no clinical skills,” “[you have] no social skills,” “[you are] only interested in research,” “[you] must love working with dead people,” and everyone’s favorite “but you’re great with patients … why you would want to go into pathology?”
Image 3. “I know you just finished—and honored—your surgery rotation but those scalpel-jockeys don’t really know how to take care of patients. Room 12B has gout and I am not about to cut his toe off!” Every time we switch rotations, medical students hear what everyone thinks about everyone else’s specialties. It can be exhausting keeping it all straight—I think by the time you graduate it just means you’ve lost track of who’s who… (Source: Medscape)
For the minority of students that figure out what specialty they like early on, those siren-songs can be a barrage to your patience. What ultimately happens is you could create a narrative of why you like pathology as an ad nauseum auto-pilot response, or you could try and engage people for their viewpoints and glean what insights you can—maybe you could even share some insight yourself. But something really interesting happens when you pursue these conversations a bit further: you learn a little more about the other person(s) and a little more about yourself in the process. I had heard the lattermost in the above list of “hits” a million times, and I used to think of it as a sort-of backhanded compliment. It wasn’t until I heard it from an attending I really respected, that my perception changed. I had done a full day’s worth of med student work in a particular clinic alongside my attending. It was full of difficult cases, challenging patients, biopsies, spot diagnoses, etc. On a few occasions I nailed a couple questions (a med student feather-in-cap moment) alongside interns and other students. At the end of the day, a conversation came up about interest in specialties, and I said pathology. Being greeted with a few comments/questions about it, along with a brief but great conversation, the attending finally said that they were impressed with me and to say that my skills would be wasted in the lab is a misnomer. Rather, my “clinical skills/work ethic” wherever I’d end up would be a valuable asset to patients anywhere in the hospital. (Um, that was a gold-star day. I think it was also a Friday, so just amazing overall.) So these stereotypic comments that used to make me feel frustrated, just got turned into one of my most memorable compliments—and I couldn’t be more grateful.
Turns out, medicine is full of moments like this. Where suddenly you learn or adjust a small piece of information and your point-of-view shifts to a new outlook. Dr. Justin Kreuter, a clinical pathologist, at the Mayo Clinic in Rochester, MN, recently wrote a perspectives piece for Mayo Medical Laboratories. It was all about taking the time to critically reflect. He linked to a few interesting articles and talked about how he takes time each day to reflect on moments and experiences he had. A mindfulness of “deliberate practice” (one of the various ways we can practice becoming better at something) shows us that being aware of opinions, cause-and-effect relationships, and our roles in certain situations can shape how we move forward from various experiences. Check his articles out and take his advice; who knows what you might learn about frustrating moments in your day, when instead you might change the entire conversation?
See you all next time!
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student actively involved in public health and laboratory medicine, conducting clinicals at Bronx-Care Hospital Center in New York City.
A 67 year old female presents with a two-month history of sore throat. She endorses dysphagia and left-sided otalgia but denies voice changes, shortness of breath, hemoptysis, weight loss, fever or night sweats. She has smoked 1 pack/day for 41 years and occasionally drinks alcohol. Her past medical history is notable for systemic lupus erythematosus for which she takes Plaquenil.
Physical examination slightly elevated systolic blood pressure. She is afebrile. Pertinent neck exam findings include mild tonsillar asymmetry (left slightly larger than right), and a firm mass at left base of tongue, and a 3 cm lymph node in the neck (left level III). A biopsy sample was taken from the tongue mass.
Biopsy
H&E stained sections reveal sheets of large lymphocytes. The lymphoid cells are medium to large in size with irregular nuclear contours and prominent nuclei. Areas of necrosis are prominent. No specific areas of epithelial ulceration are noted. Immunophenotypic characterization of the larger cells reveals positivity for CD20, CD30, CD79a, PAX5, MUM1, Epstein Barr virus encoded RNA (EBER) and a variable Ki-67 proliferation index, which is up to 60-70% in the larger cells, but around 20-30% overall. Only rare cells are positive for BCL-2 and BCL-6. The lymphoma cells are negative for keratin AE1/AE3, CD10, CD4, CD8, CD21, CD23, CD7, CD5, Cyclin D1, CD68, CD56, and CD43. The background T cells express CD5 and CD7 and are a mixture of CD4 and CD8 with CD4 predominance.
We considered the diagnosis of EBV-positive mucocutaneous ulcer (a more indolent entity); however, the lack of history of an ulcer/ulceration and the presence of a mass-lesion (with additional adenopathy) does not support this diagnosis.
The findings are most consistent with EBV-positive DLBCL, NOS (WHO 2017), previously known as EBV positive DLBCL of the elderly (WHO 2008).
Discussion
Epstein Barr Virus, a member of the Herpesviridae family is mostly known for causing Infectious Mononucleosis. However, the ubiquitous virus which is present in about 90% of adults but often asymptomatic1, has a predilection for epithelial cells including B-cells.2 Incorporation of the viral genome and viral takeover of the cells proliferative machinery underlies the pathogenesis of any EBV-related disease/malignancy. It has been associated with a gastric carcinoma, fulminant hepatitis, undifferentiated nasopharyngeal carcinoma, and B cell, T cell and NK cell lymphomas3, including EBV+ diffuse large B-cell lymphoma, not otherwise specified (DLBCL-NOS).
EBV-positive diffuse large B-cell lymphoma, not otherwise specified (EBV+ DLBCL-NOS) was formerly known as EBV-positive diffuse large B-cell lymphoma (DLBCL) of the elderly. The WHO classification substituted “not otherwise specified” in place of “for the elderly” to reflect two things: 1) EBV is associated with other specific neoplastic Large B-Cell diseases such as lymphomatoid granulomatosis, and 2) EBV+DLBCL can affect younger individuals as well as the elderly. 2
EBV+DLBCL-NOS patients may occur in nodal or extranodal sites, with up to 40% presenting with extranodal sites at least in the early stages. Patients may be asymptomatic with or without B symptoms but usually, patients present with rapidly enlarging tumors at single or multinodal sites, as well as at extranodal sites. 4
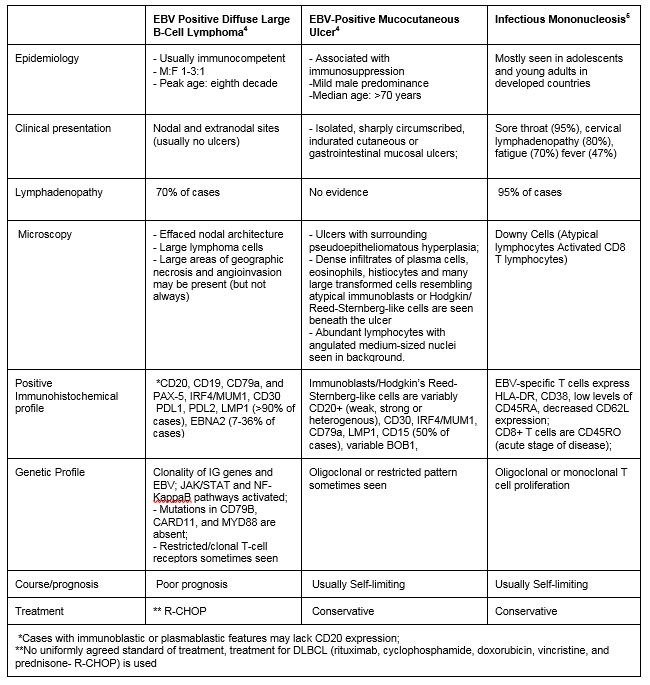
The patient’s presentation with sore throat and the finding of neck mass with EBV-positive large B-cells associated with ulcer-like necrosis raises a differential diagnosis that ranges from reactive to malignant. Table 1 shows a comparison between three differential diagnoses: EBV+DLBCL-NOS; EBV-positive mucocutaneous ulcer; and infectious mononucleosis.
Table 1. Comparison of 3 EBV-positive differentials in the head and neck
Unfortunately, there is currently no uniformly agreed standard of treatment for EBV+DLBCL which has a worse prognosis than EBV negative DLBCL.2 The standard treatment for DLBCL (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone- R-CHOP) is used but it responds poorly to treatment, with a median survival of 2 years.
Therefore, early detection by clinical suspicion and testing all DLBCL patients for EBV is very important.2
Okano, Motohiko, MD, PhD|Gross, Thomas G., MD, PhD. Acute or chronic life-threatening diseases associated with epstein-barr virus infection. American Journal of the Medical Sciences, The. 2012;343(6):483-489. https://www.clinicalkey.es/playcontent/1-s2.0-S0002962915309435. doi: 10.1097/MAJ.0b013e318236e02d.
Swerdlow S, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Arber D, Hasserjian R, Le Beau M. WHO classification of tumours of haematopoietic and lymphoid tissues. 2017.
Dunmire SK, Hogquist KA, Balfour HH. Infectious Mononucleosis. Current topics in microbiology and immunology. 2015;390:211-240. doi:10.1007/978-3-319-22822-8_9.
-Adesola Akinyemi, M.D., MPH, recently earned his MPH-Health Policy and Management from New York Medical College. He plans on pursuing residency training in pathology. His interests include cytopathology, neuropathology, and health outcomes improvement through systems thinking and design.
-Kamran M. Mirza, MD PhD is an Assistant Professor of Pathology and Medical Director of Molecular Pathology at Loyola University Medical Center. He was a top 5 honoree in ASCP’s Forty Under 40 2017. Follow Dr. Mirza on twitter @kmirza.
Hello everyone! Back again with another post about that interesting space between my experiences working in laboratory medicine as an MLS and my current path through medical school toward a career in pathology. Last month, I discussed how the new 5th generation cardiac enzyme assays are evolving and reaffirming the relationships between lab data and clinical decision making. This month, as I adjust to a very different circadian rhythm, I’d like to talk about some topics in my surgery rotation as they relate to surgical pathology and the lab.
Just to summarize, besides epidemiological research and public health initiatives I’ve written about here on this blog, I had several years of lab work before medical school. In my experience, I have seen the gamut of required steps for pathology specimens peri/post-operatively. Everything from placenta, bone, blood, marrow, skin, brain, lung, GI, to any other organ system’s tissue is processed, blocked, stained and examined on glass by pathologists who write reports for their clinical colleagues. Often, we in the lab receive phone calls from providers inquiring about turn-around times and results as they follow-up on their patients and cases. In Chicago, I was able to see and train in a great trauma center at Northwestern, community hospitals like Swedish Covenant and Weiss Memorial, and an academic hospital centers like Rush and UIC. What I learned there is just how much really depends on those pathology reports. Cytology, diagnostic immunohistochemistry, morphology, margins, and gross analysis all contribute to a final diagnosis. After an extended observership at UAB Medical Center, I was fortunate to see first-hand the critical process involved in signing out dermatology consults, examining gross pathology, and even frozen neuropathology specimens. Sitting with attendings in the OR and frozen rooms deciding between glioblastoma multiforme, lymphoma, or something benign (read: defer to permanent slide diagnosis later) was fascinating. Meanwhile, I’m now a month into formal surgical rotations at Bronx-Care Hospital in NY and I get to see the other side of the pathology report.
The Relationships Between Surgeons and Pathologists are Critical
Many surgical interventions and procedures require resection of known or suspected pathologic tissue. Whether it’s malignancy, benign growth, obstruction, adhesion, or otherwise mechanically compromising tissue, many patients require a surgeon to remove the entity in question. And, while the difficulty of these excisions and resections may vary depending on location, cases rely heavily on the pathologist-surgeon collaboration. Virtually all neoplasms are diagnosed through anatomic pathology assessment under a microscope. Fine needle aspirates, pap smears, bone marrow biopsies, and countless other tissues must go through pathology before being finalized. This interdisciplinary collaboration between the surgical team and the pathology team is, of course, by nature acutely critical. In proper circumstances, open cases in the operating room are consulted to a pathologist STAT. The effective communication between the pathologist and surgeon awaiting the intraoperative consultation is key to effectively treating their shared patient. Sometimes operating rooms will have live microscopic image-casting, sometimes there is an intercom system, sometimes its solely based on electronic forms in the EHR, and sometimes pathologists need to go into the surgical field to examine the resection intraoperatively in person. However it happens, this is a very important relationship that patients might not be aware of.
The Point of View Between Surgical Pathology and Clinical Surgeons Are Different
So this sounds like a perfect match, right? Surgeons and pathologists living in harmony? Unfortunately, harmony isn’t part of regular onboarding at many institutions so, as with any staff, there are different scopes and sometimes this can be a challenge. Getting a frozen notification as a pathologist is a serious task. They are emergent and must be addressed immediately and diagnoses are made with serious gravity, often consulting with other pathologists. This is also, however, a singular teaching moment as every frozen section is different and pathologists use these learning opportunities to teach their residents and medical students. In the interests of accurate diagnoses, educational value, and appropriate response to the OR, pathologists take measures to ensure success. For example, frozen specimens will be received, a history and presentation of the patient is discussed, the specimen is partitioned for frozen section (STAT), permanent section, and further studies (routine). So, for the pathologist it’s all about accuracy, reliability, and what they can confidently report. The surgeon has a different point of view: they are operating with a specific physical goal in mind by either resecting a tumor, or isolating good margins from a known malignancy, or ensuring the tissue being removed is correct/adequate for its therapeutic purpose. Fun fact: surgical pathology was a field originally developed by surgeons! There are things a pathologist only knows, and there are things a surgeon only knows—but when working together, the overlap of medical knowledge increases the coverage of care for their shared patients’ outcomes.
Image 1. A pathologist processes a frozen specimen on a cryostat machine. A summary of frozen sections from JAMA,2005;294(24):3200. doi:10.1001/jama.294.24.3200
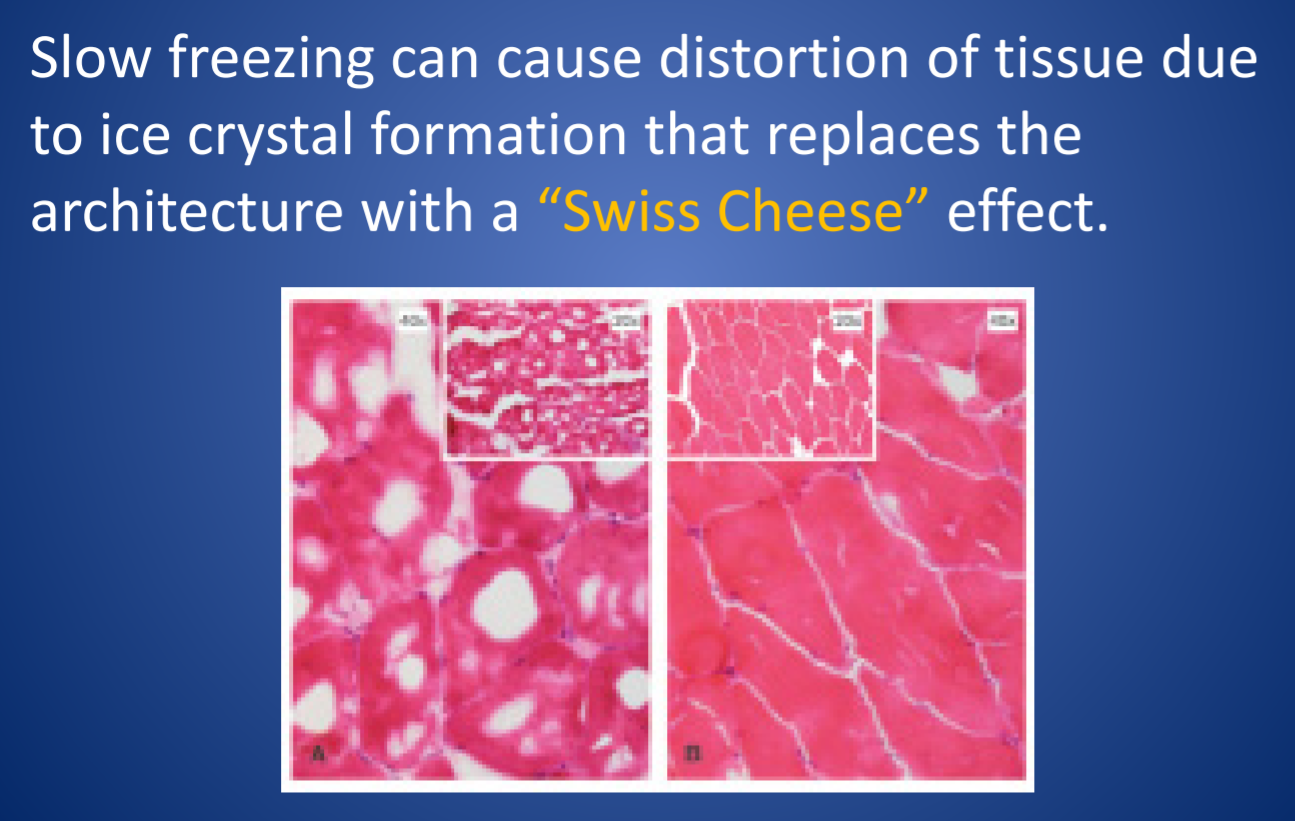
The Cold Truth About Frozen Sections
Frozen specimens aren’t perfect. In these specimens, tissue gets stiffened by freezing instead of routine paraffin embedding, and because of that a frozen section could be distorted by folds, tears, and other artifacts that might appear because of mechanical manipulation during processing. Frozen samples also leave artifacts where water would crystallize and freeze, but one of the caveats regarding artifacts in frozen sections is that FAT DOES NOT FREEZE. Instead, specimens that have large fat content (i.e. brain tissue) have to be examined carefully to not confuse findings with inflammation or other pathologic processes. Ultimately, it takes numerous cases to properly hone the skills required to confidently diagnose from frozen section. While they might not be perfect, it is a critical tool used between the surgical and pathology teams. Challenges in this handoff process relate to proper use of this surgical tool. For instance, if a frozen is called for and the surgery is closed by the time a pathology report is filed, then (assuming there were no serious delays) this may have been an inappropriate specimen decision. Furthermore, specimens must be discussed prior to receipt for appropriateness and clinical relevance. Fatty lipomas aren’t going to go to frozen section, they shouldn’t be ordered. A thyroid lobectomy? That’s a better utilization of resources and tools.
Ultimately, with proper training and experience a pathologist can effectively use the frozen section as a useful clinical tool to improve patient outcomes. Surgeons operating in the best interests of their patients, should strive to create a functional and successful communication between both services. My experiences in NY with surgeons of various kinds reveals a common truth among them: pathology is a critical player in surgical interventions, and without margins, diagnostic stains, and other work-ups, those interventions would be much more difficult and risky.
Thanks again! See you next time!
Bonus: for more content specifically detailing some of the cellular morphologies and cytology I discussed above, please check out I Heart Pathology, a compendium website my friend and colleague at UAB, Dr. Tiffany Graham, manages. It’s meant for other pathology residents to review and refresh on material and it’s updated as often as possible. Check out the link here: https://www.iheartpathology.net/
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student actively involved in public health and laboratory medicine, conducting clinicals at Bronx-Care Hospital Center in New York City.
As an unscheduled post, I’d like to make a quick side note separate from public health, zika, and medical school. You may have seen a post I wrote last January about the potential stereotypes and stigmas we might face in laboratory medicine. But, just because we as laboratory professionals operate behind-the-scenes most of the time, we’re still healthcare professionals—and clinician burnout can affect any of us.
I recently watched a video of Dr. Zubin Damania, also known as “ZDoggMD,” a primary care physician and founder of Turntable Health in Las Vegas. He’s a brilliant and passionate doctor with great opinions and an even greater creative sense of humor. Among his many parodies, and “rounds” Q&A questions, ZDoggMD recently had a guest on one of his Facebook shows called “Against Medical Advice” to address the serious issue of suicide and depression in medicine. Janae Sharp was the guest on this episode speaking about her husband, John, a physician fresh into his residency who committed suicide. They go on to talk about her life after this tragedy and how if flipped her and their children’s’ lives upside down. Janae’s described John as a father, a writer, a musician, an idealist, who always wanted to become a doctor. My interest was definitely piqued by this—I tend not to miss most of Dr. Damania’s content—and this is something I’ve been hearing more and more about as my path through medical school continues. But, at one point in the interview my heart just stopped: John was a clinical pathologist. Too close to home, for me at least. I was admittedly surprised.
Pathologist’s don’t have that much stress to make depression and suicide part of that life, I thought. But that is a cold hard assumption. Depression affects so many people at large, and when you’re in healthcare it almost seems like a risk factor on top of issues one might be struggling with. Med school is touted as one of the hardest intellectually, physically, and emotionally grueling experiences you could go through—I will personally vouch for Dr. John and Dr. Damania’s statements about how much these experiences push you to your limits. No sleep, no recognition, no support, fear of failure, imposter syndrome, a wealth and breadth of knowledge that makes you feel like you’re drowning—not to mention that if you do ask for help you’re immediately “lesser” for doing so.
Video 1. ZDoggMD interviews Janae Sharp about her tragic loss, her husband John’s suicide, and the rampant problem of depression and burnout in medicine. Against Medical Advice, Dr. Damania.
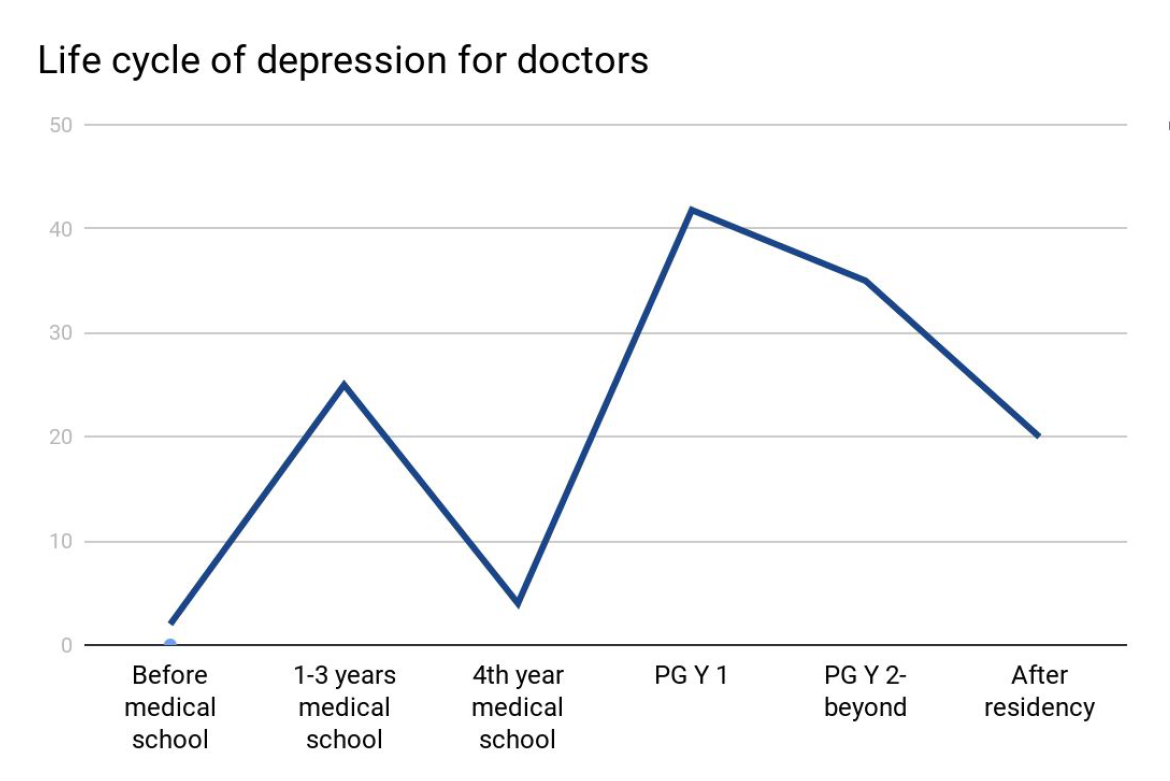
Last month, I was fortunate enough to attend a grand rounds session at my current hospital about this very topic. Presented by Dr. Elisabeth Poorman, internal medicine attending physician, and clinical instructor at Harvard Medical School, who talked about how (because of stigmas) medical trainees don’t get the help they need. She demonstrated that prior to med school students are pretty much on-par with their peers with regard to depression. However, once medical school starts, those peers all plummet together as depression rates rise and fall dramatically throughout the various stages of their careers. (I’m just going to go ahead and vouch for this too.) Dr. Poorman shared several case studies that effectively conveyed just how hard it can be when it seems like you are a source of help for many, but no one is there to help you. Story and story recounted the same model of apparent—and often secretive—burnout which ultimately led to a decrease in the quality of care, and in some instances suicide. Dr. Poorman was also brave enough to share her own story. No stranger to depression, herself, it was something that she encountered first hand. She connected herself with this increasingly difficult picture of inadequate support for those of us spending our lives serving others.
Figure 1. Dr. Poorman’s data reveals that depression rates for medical school classmates in a cohort generally rise and fall as their duties and responsibilities change during their career trajectory. I’m currently on the slope downward between the first 1-3 years of school’s peak and the 4th year trough.
There are clear problems facing those of us in healthcare jobs. An ironic consequence, however, of modern scientific advancement is the “doubling time” of medical knowledge. While not necessarily a problem, this refers to the amount, depth, and scope of knowledge physicians and medical scientists are expected to master in order to effectively treat, make critical clinical decisions, and educate our patients. While in 1980 it took 7 years for all medical knowledge to double in volume, it only took 3.5 years in 2010, and in 2020 it’s expected to double every 73 days!1. The problems come as a result of this knowledge because more data means more to do. More time on the computer, higher critical responsibility, and less time to focus on your own mental health all lend themselves to a cyclic trap of burnout. Physicians commit suicide at a rate of 1.5 – 2.3 times higher than the average population.1
Physicians, nurses, clinical scientists, lab techs, administrators, phlebotomists, PCTs—we’re all over worked, under-supported, fall victim to emotional fatigue, and have some of the highest rates for depression, substance abuse, PTSD, and suicide.1 Sometimes, reports from Medscape or other entities will report that burnout is a phenomenon of specialty, hypothesizing that critical nature specialties have more depression than lesser ones2 (the assumption that a trauma surgeon might burn out before a hematopathologist). But truthfully, this is just part of the landscape for all providers. A May 2017 Medscape piece wrote “33% chose professional help, 27% self-care, 14% self-destructive behaviors, 10% nothing, 6% changed jobs, 5% self-prescribed medication, 4% other, 1% pray.”3
So I’m talking about this. To get your attention. So that people reading know they’re not alone. So that people with friends going through something can lend a hand. I’m talking about this. ZDoggMD is talking about this. Jamie Katuna, another prolific medical student advocate, is talking about this. Dr. Elisabeth Poorman is talking about this. This is definitely something we should come together to address and ultimately solve.
What will you do to help?
This was a heavy topic. So in a lighter spirit, I have to share this with all of my laboratory family. If you haven’t heard or seen Dr. Damania’s videos yet, this is the one for you:
Thanks! See you next time!
References
Poorman, Elisabeth. “The Stigma We Live In: Why medical trainees don’t get the mental health care they need.” Cambridge Health Alliance, Harvard Medical School. Grand rounds presentation, Feb 2018. Bronx-Lebanon Hospital Center, New York, NY.
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student at the American University of the Caribbean and actively involved with local public health.
The Jaffe and enzymatic methods are the two most common methods for measuring serum creatinine. The Jaffe method is less expensive than the enzymatic assay ($0.30 vs $2.00 per test based on 2014 list prices) but is more susceptible to interferences. Although these tests are not expensive, they are high-volume tests and the savings could be substantial. We were using the enzymatic assay at the University of Utah and estimated that we could save about $50,000 per year by switching to the Jaffe assay; however, we were uncertain whether the Jaffe assay was safe to use due to the potential for interferences. For that reason, we decided to conduct a risk assessment to evaluate the suitability of the Jaffe assay.
Risk is defined as the expected cost of an action. The expected cost has two components: 1) the probability that an event will occur and 2) the consequences or cost of an event:
Risk = prob(event) x cost(event)
The event of interest was misclassification of a patient due to an error in serum creatinine measurement. Nephrologists classify kidney disease based on the estimated glomerular filtration rate which is based on the creatinine value. The distribution of eGFR for patients at our hospital is shown in Figure 1. The dashed lines show decision limits that nephrologists use to classify kidney disease. An eGFR is considered normal or healthy.
We spoke with the nephrologists and learned that they were relatively unconcerned about errors in eGFR in healthy patients (eGFR above 60 ml/min) because there was no potential for harm. Similarly, they felt there was relatively little risk of harm to patients with low eGFRs because these patients are routinely monitored and no major decision would be based solely on a single eGFR measurement. An error in creatinine measurement in a low eGFR patient would be detected by repeat measurements or be inconsistent with other measurements. From the nephrologists’ point of view, the only area of concern was in the region around 60 ml/min. Patients about 60 ml/min are considered healthy whereas those below 60 ml/min are diagnosed with stage 3a chronic kidney disease. In this zone, an error in serum creatinine could result in a false negative (i.e. observed eGFR greater than 60 ml/min when the true eGFR was less than 60 ml/min). In such cases, a patient may go without care and their disease could progress. The nephrologists believed that the potential for harm was relatively minor, but potential for harm did exist.
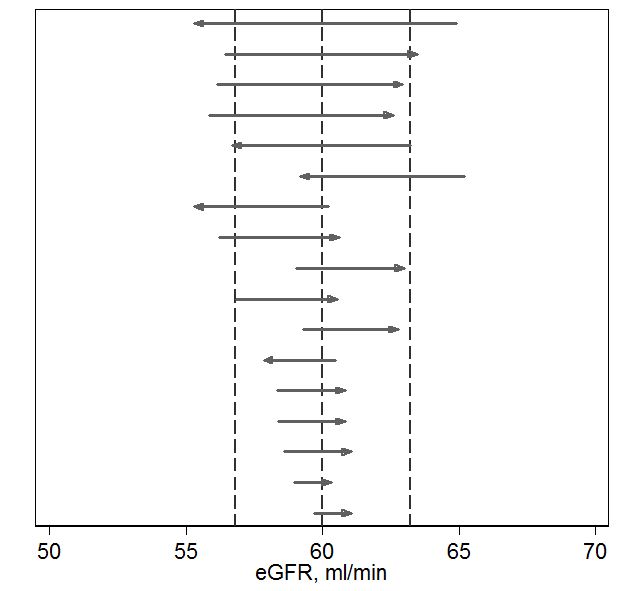
We compared the eGFRs provided by the enzymatic and Jaffee methods to estimate how often patients might be misclassified (Figure 2).1 Focusing on the 60 ml/min decision limit, we found that 17 of 500 (3.4%) of measurements were discordant. Some of these discordant results would be due to imprecision. Discordance due to imprecision would have small differences (bottom of Figure 2) and are unavoidable – they would occur using any method. Discordance due to interference would be expected to have larger differences (top of Figure 2) and could be avoided by using the enzymatic method. We used statistical techniques to estimate the proportion of discordances that were due to interference vs imprecision and found that about 60% of the discordance at the 60 ml/min limit was due to interference. In summary, our risk analysis showed that using the Jaffe method would pose about a 2% rate of avoidable misclassification which presented some potential risk to patients. The nephrologists felt the risk was low but, in theory, disease could unnecessarily progress in a patient with a false negative diagnosis.
Our risk analysis was based on analytical error. We compared magnitude of analytical error to the biological variation in eGFR and found that the analytical error was relatively small in comparison to biological variation (data not shown). Biological variation was likely to be a more significant cause of misclassification than analytical error.
So, what to do? Was the potential savings of the Jaffe method worth the risk? Some experts recommend against using the Jaffe method. 2-4 On the other hand, most US laboratories use the Jaffe assay. A recent College of American Pathologists proficiency challenge found that 70% of the submitted results were based on the creatinine assay.5
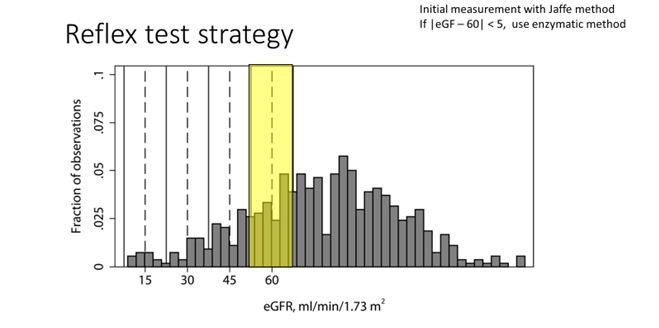
We decided to get the best of both worlds by using BOTH methods. We defined a zone of risk surrounding the 60 ml/min eGFR decision limit (Figure 3). Results in this zone would have some risk of misclassification whereas results outside of the zone would be unlikely to be misclassified using the Jaffee method. All creatinine measurements are initially performed using the Jaffe method. If the result is outside the risk zone, the result is reported. If results fell within the risk zone, they were repeated with the enzymatic method and the results of the enzymatic method are reported. This reflex procedure saves money while avoiding risk. The reflex rate is approximately 15%.
There are circumstances in which one would want to order the best possible test. To that end, we created a special orderable test, based on the enzymatic method, that the nephrologists could use to insure the most accurate results when required. For example, the enzymatic test may be indicated when making decisions regarding biopsies for renal transplant patients. The order volume for the special test has been less than 100 orders per year.
Figure 1. Distribution of Estimated Glomerular Filtration rates (eGFR). The distribution is for outpatients at University of Utah for calendar year 2014. The dashed lines indicate decision limits used for classification of chronic kidney disease (15, 30, 45 and 60 ml/min). eGFRs greater than 60 ml/min are considered disease free.
Figure 2. Discordances in estimated glomerular filtration rate (eGFR) at the 60 ml/min decision limit. The length of each arrow, represents the difference between estimates based on the Jaffe (head) and enzymatic (tail) methods. The dashed line represents two standard deviations of expected imprecision of the difference. Differences greater than 2 standard deviations would most likely be due to analytical interference (loss of specificity).
Figure 3. Reflex test strategy. The figure shows the distribution of eGFR values for outpatients at the University of Utah. The dashed lines represent clinical decision limits. The yellow zone represents the range of eGFR values where misclassification could pose a risk to patients. Creatinine is first measured by the Jaffe method. The Jaffe result is reported if the estimated eGFR is outside the yellow zone. If the eGFR is within the yellow zone, the measurement is repeated using the enzymatic method and the result based on the enzymatic method is reported.
References
Schmidt RL, Straseski JA, Raphael KL, Adams AH, Lehman CM. A Risk Assessment of the Jaffe vs Enzymatic Method for Creatinine Measurement in an Outpatient Population. PloS one. 2015;10(11):e0143205.
Cobbaert CM, Baadenhuijsen H, Weykamp CW. Prime time for enzymatic creatinine methods in pediatrics. Clinical Chemistry. 2009;55(3):549-558.
Drion I, Cobbaert C, Groenier KH, et al. Clinical evaluation of analytical variations in serum creatinine measurements: Why laboratories should abandon Jaffe techniques. BMC Nephrology. 2012;13(1).
Panteghini M. Enzymatic assays for creatinine: time for action. Scand J Clin Lab Invest Suppl. 2008;241:84-88.
College of American Pathologists. Chemistry/Therapeutic Monitoring, Participant Survey. 2014.
-Robert Schmidt, MD, PhD, MBA, MS is currently an Associate Professor at the University of Utah where he is Medical Director of the clinical laboratory at the Huntsman Cancer Institute and Director of the Center for Effective Medical Testing at ARUP Laboratories.
If you’re a laboratory professional or pathologist under 40 who is a mover and a shaker, then ASCP’s “40 under 40” should be on your radar. Update your resume and apply!