Hello! My name is Constantine Kanakis and I am very happy to contribute to Lab Medicine’s online blog! As my first post, I would like to introduce myself, tell you a little bit about my interests in laboratory medicine, and also discuss Zika virus research I’m actively involved in.
I studied molecular biology at Loyola University and medical laboratory science at Rush University, both in Chicago. From undergraduate to graduate school, I was fortunate enough to work on research topics involving the neurology of nematodes, enzymatic plant assays, social justice/urban planning work, microbiological lab equipment development, and novel biochemical hematopoietic interventions. This comprehensive experience in research work provided a strong foundation which I have found useful in my career both in and out of the hospital laboratory. Other than research, I spent nearly nine years working in some of Chicago’s busiest hospitals. I learned the ropes in a variety of settings: trauma center transfusion medicine, academic center quality assurance, public health work, and community hospital laboratory work. I feel personally drawn to laboratory medicine and pathology, as it connects translational research to patient outcomes and puts us in a position to mobilize fellow professionals to improve health care in our communities.
This bridge from lab discoveries to bedside and beyond motivated me to write for this blog community. The current Zika virus outbreak as well as the start of my medical school career has provided a great opportunity for me to explore translational research and its direct impact into a local community. Currently, I am a second year medical student at American University of the Caribbean School of Medicine located on the island of Sint Maarten, in the Netherlands Antilles (Figure 1). I find myself in the epicenter of the now infamous viral epidemic of everyone’s new favorite Arbovirus: Zika. Studying in the Caribbean, I am actively involved in projects assessing the emergence of this viral phenomenon. Today, CDC lists countries with active infections with a Level 2 travel active warning notice, “[to] Practice Enhanced Precautions.” These projects have three tiers: laboratory studies, collaboration with local health partners, and integration of research with public health efforts. My location here provides ample opportunity to gather information at its source, most notably from our neighbors in Brazil, Puerto Rico, and even Florida. This island is high on the list of endemic countries with 1,730 suspected Zika cases reported as of July, 2016, however only 12% of those cases were serologically confirmed. The suspected cases have been rising in the last few months (Figure 2) and epidemiologists are watching the trends very closely.

Figure 1. The Centers for Disease Control and Prevention (CDC), updates regions on the world map which have reported active Zika virus infections, CDC 5 October 2016.
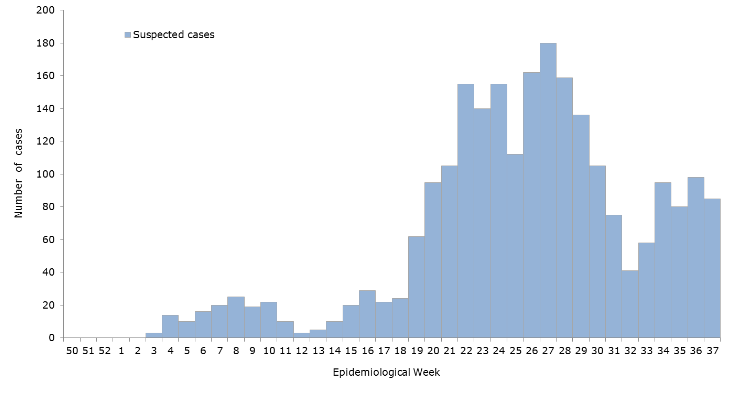
Figure 2. Suspected Zika viral infection cases per epidemiological week, Pan-American Health Organization (PAHO) and World Health Organization (WHO) 2016.
As a primer for those who are interested, the Zika virus is a Flavivirus/Arbovirus undergoing its second recent epidemic spread in the last decade. Discovered in the 1950s, it has been considered a minor viral infectious agent. To date, researchers near and far are exploring both potential vaccination and prevention measures, as well as infection control efforts as some claims link the virus to microcephaly, Guillain-Barre, and other various sequale. It is transmitted primarily by mosquito bites directly into the blood, though its antigenic presence has persisted in urine and even seminal fluid. Research in public health and epidemiology has also related the management of this outbreak to previous ones, including that of the 2014 Ebola epidemic. There is contention between various public health organizations and laboratory researchers in detailing any exact correlation of the viruses secondary effects as well as the difficulty in specific detection and diagnosis relative to reported vs. confirmed cases (Figure 3).

Figure 3. A general demonstration of the purported Zika infection cases and how this reflects the true nature of the epidemic in the Caribbean in collaboration with the PAHO and WHO, from the Caribbean Public Health Agency (CARPHA) 2016.
Several research projects are starting here on campus, a majority of which involve serologic prevalence and surveillance studies. Some new studies are aimed directly at using commercially available testing, while others compound data from previously significant outbreaks of other arboviruses (e.g. Chikungynya, Dengue, Yellow Fever, West Nile). Our work in the laboratories here is also matched with significant public outreach. I am involved in one particular service and outreach project through the university here which targets the dissemination of Zika prevention/infection knowledge through various informational outlets such as town hall meetings, health drives for children, and vector control projects in the field. Our school-based task forces have been fortunate enough to form partnerships with the local Ministry of Public Health, Social Development, and Labor here on the island. And, coordinating with their Collective Prevention Services, they are now involved in reaching out to the community at large (see Figure 4).

Figure 4: One of the newest school projects sponsored this year included a vector control initiative partnership with the Sint Maarten Red Cross, and the Ministry of Health’s Collective Prevention Services, conducting home inspections in areas of statistically high reportable cases, photo credit: A. Yancone 2016.
On a personal note, I will add that my wife and I, along with several of our friends here have ironically been “bitten by the Zika bug.” We all suffered the same relative symptoms (fever, malaise, myalgia, headaches, and the infamous maculopapular rash), so I can speak personally on the effects of an active Zika infection! Really though, it isn’t that bad; it felt like a bad flu—most locals are not too worried about Zika because they already have several other arthropod-borne viral infections to stay away from with significantly worse courses of infection. Chikungynya, Dengue Fever, Yellow Fever, West Nile, less often Plasmodium/Malaria, and others offer more of a threatening presence than the several day woes of a Zika infection. Moreover, those other infections sometimes have even worse complications and clinical presentations.
As I begin and continue my work through these projects, I will provide updates—both on our efforts here in the laboratory as well as our work in reaching out and partnering with local public health officials to try and make a positive impact on our local community. And since I am now “inoculated,” I’ll be happy to get really close to the action for all of you.
Thanks for reading!

-Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student at the American University of the Caribbean and actively involved with local public health.

4 thoughts on “An Arbovirus Abroad”