Hello everyone! Back again with another post about that interesting space between my experiences working in laboratory medicine as an MLS and my current path through medical school toward a career in pathology. Last month, I discussed how the new 5th generation cardiac enzyme assays are evolving and reaffirming the relationships between lab data and clinical decision making. This month, as I adjust to a very different circadian rhythm, I’d like to talk about some topics in my surgery rotation as they relate to surgical pathology and the lab.
Just to summarize, besides epidemiological research and public health initiatives I’ve written about here on this blog, I had several years of lab work before medical school. In my experience, I have seen the gamut of required steps for pathology specimens peri/post-operatively. Everything from placenta, bone, blood, marrow, skin, brain, lung, GI, to any other organ system’s tissue is processed, blocked, stained and examined on glass by pathologists who write reports for their clinical colleagues. Often, we in the lab receive phone calls from providers inquiring about turn-around times and results as they follow-up on their patients and cases. In Chicago, I was able to see and train in a great trauma center at Northwestern, community hospitals like Swedish Covenant and Weiss Memorial, and an academic hospital centers like Rush and UIC. What I learned there is just how much really depends on those pathology reports. Cytology, diagnostic immunohistochemistry, morphology, margins, and gross analysis all contribute to a final diagnosis. After an extended observership at UAB Medical Center, I was fortunate to see first-hand the critical process involved in signing out dermatology consults, examining gross pathology, and even frozen neuropathology specimens. Sitting with attendings in the OR and frozen rooms deciding between glioblastoma multiforme, lymphoma, or something benign (read: defer to permanent slide diagnosis later) was fascinating. Meanwhile, I’m now a month into formal surgical rotations at Bronx-Care Hospital in NY and I get to see the other side of the pathology report.
The Relationships Between Surgeons and Pathologists are Critical
Many surgical interventions and procedures require resection of known or suspected pathologic tissue. Whether it’s malignancy, benign growth, obstruction, adhesion, or otherwise mechanically compromising tissue, many patients require a surgeon to remove the entity in question. And, while the difficulty of these excisions and resections may vary depending on location, cases rely heavily on the pathologist-surgeon collaboration. Virtually all neoplasms are diagnosed through anatomic pathology assessment under a microscope. Fine needle aspirates, pap smears, bone marrow biopsies, and countless other tissues must go through pathology before being finalized. This interdisciplinary collaboration between the surgical team and the pathology team is, of course, by nature acutely critical. In proper circumstances, open cases in the operating room are consulted to a pathologist STAT. The effective communication between the pathologist and surgeon awaiting the intraoperative consultation is key to effectively treating their shared patient. Sometimes operating rooms will have live microscopic image-casting, sometimes there is an intercom system, sometimes its solely based on electronic forms in the EHR, and sometimes pathologists need to go into the surgical field to examine the resection intraoperatively in person. However it happens, this is a very important relationship that patients might not be aware of.
The Point of View Between Surgical Pathology and Clinical Surgeons Are Different
So this sounds like a perfect match, right? Surgeons and pathologists living in harmony? Unfortunately, harmony isn’t part of regular onboarding at many institutions so, as with any staff, there are different scopes and sometimes this can be a challenge. Getting a frozen notification as a pathologist is a serious task. They are emergent and must be addressed immediately and diagnoses are made with serious gravity, often consulting with other pathologists. This is also, however, a singular teaching moment as every frozen section is different and pathologists use these learning opportunities to teach their residents and medical students. In the interests of accurate diagnoses, educational value, and appropriate response to the OR, pathologists take measures to ensure success. For example, frozen specimens will be received, a history and presentation of the patient is discussed, the specimen is partitioned for frozen section (STAT), permanent section, and further studies (routine). So, for the pathologist it’s all about accuracy, reliability, and what they can confidently report. The surgeon has a different point of view: they are operating with a specific physical goal in mind by either resecting a tumor, or isolating good margins from a known malignancy, or ensuring the tissue being removed is correct/adequate for its therapeutic purpose. Fun fact: surgical pathology was a field originally developed by surgeons! There are things a pathologist only knows, and there are things a surgeon only knows—but when working together, the overlap of medical knowledge increases the coverage of care for their shared patients’ outcomes.

The Cold Truth About Frozen Sections
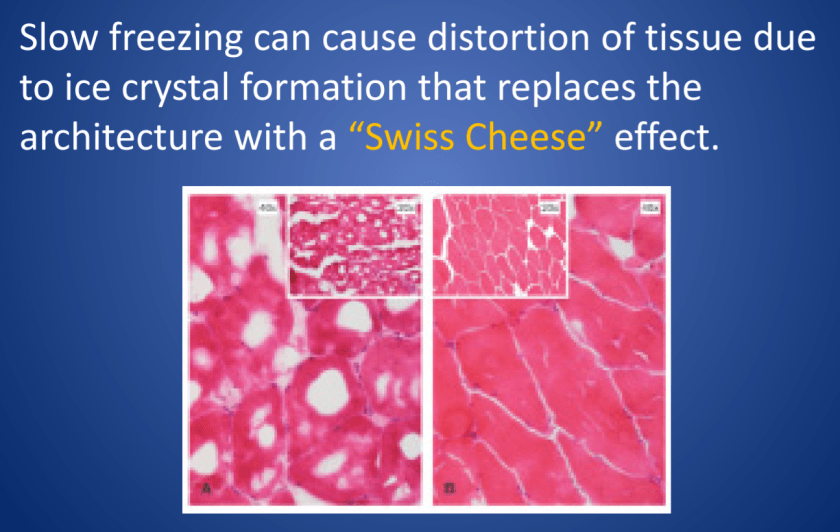
Frozen specimens aren’t perfect. In these specimens, tissue gets stiffened by freezing instead of routine paraffin embedding, and because of that a frozen section could be distorted by folds, tears, and other artifacts that might appear because of mechanical manipulation during processing. Frozen samples also leave artifacts where water would crystallize and freeze, but one of the caveats regarding artifacts in frozen sections is that FAT DOES NOT FREEZE. Instead, specimens that have large fat content (i.e. brain tissue) have to be examined carefully to not confuse findings with inflammation or other pathologic processes. Ultimately, it takes numerous cases to properly hone the skills required to confidently diagnose from frozen section. While they might not be perfect, it is a critical tool used between the surgical and pathology teams. Challenges in this handoff process relate to proper use of this surgical tool. For instance, if a frozen is called for and the surgery is closed by the time a pathology report is filed, then (assuming there were no serious delays) this may have been an inappropriate specimen decision. Furthermore, specimens must be discussed prior to receipt for appropriateness and clinical relevance. Fatty lipomas aren’t going to go to frozen section, they shouldn’t be ordered. A thyroid lobectomy? That’s a better utilization of resources and tools.
Ultimately, with proper training and experience a pathologist can effectively use the frozen section as a useful clinical tool to improve patient outcomes. Surgeons operating in the best interests of their patients, should strive to create a functional and successful communication between both services. My experiences in NY with surgeons of various kinds reveals a common truth among them: pathology is a critical player in surgical interventions, and without margins, diagnostic stains, and other work-ups, those interventions would be much more difficult and risky.
Thanks again! See you next time!
Bonus: for more content specifically detailing some of the cellular morphologies and cytology I discussed above, please check out I Heart Pathology, a compendium website my friend and colleague at UAB, Dr. Tiffany Graham, manages. It’s meant for other pathology residents to review and refresh on material and it’s updated as often as possible. Check out the link here: https://www.iheartpathology.net/

–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student actively involved in public health and laboratory medicine, conducting clinicals at Bronx-Care Hospital Center in New York City.

is there ego /power struggles in the lab