Maryam Zenali1*, Dmitriy Akselrod2, Eric Ganguly3, Eswar Tipirneni4 and Christopher J. Anker5*
1 Department of Pathology, 2 Department of Radiology, 3 Division of Gastroenterology, and 5 Division of Radiation Oncology, The University of Vermont Medical Center (UVMMC), Burlington, VT and 4 Department of Hematology Oncology, Central Vermont Medical Center (CVMC), The University Of Vermont Health Network, Adult Primary Care, Berlin, VT
*corresponding authors
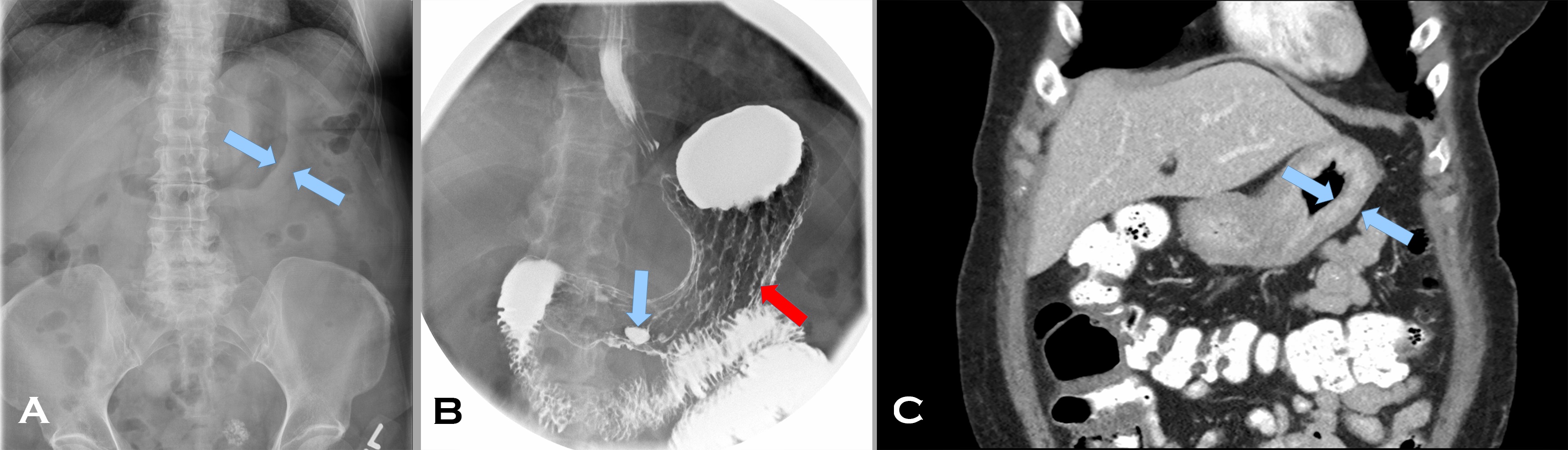
A 57 year old woman with a personal and family history of breast cancer presented with early satiety and dysphagia for 5 months. Her abdominal computed tomography (CT) scan (Image 1 A) showed marked thickening of an apparently featureless gastric wall (A, blue arrows indicating the mucosal [rightward pointing] and serosal [leftward pointing] aspects of the gastric wall). Prominent gastrohepatic lymph nodes were noted as well. Her fluoroscopic upper GI study (Image1 B), following administration of barium and effervescent crystals (a double contrast effect to allow for mucosal evaluation), showed thickened rugal folds (B red arrow) and pooling of barium within an antral ulcer (B blue arrow). A subsequent CT scan (Image 1 C) after administration of intravenous and enteric contrast, confirmed marked diffuse gastric wall thickening (C blue arrows again indicating the mucosal [rightward pointing] and serosal [leftward pointing] aspects of the gastric wall) (Image 1, composite radiographs A-C).
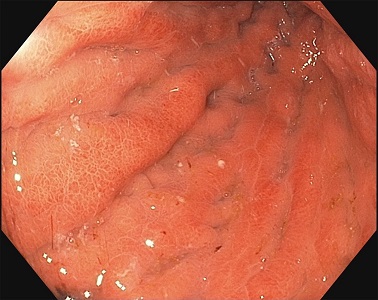
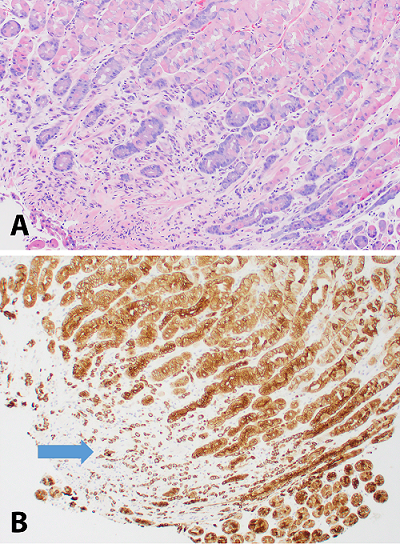
The gastric body distended poorly with insufflation and demonstrated thickened, erythematous, edematous folds with erosions (Image 2, endoscopy image). On endoscopic ultrasound, the total thickness of the stomach was 12 mm with expanded wall layers in the proximal stomach to the antrum and a thickness of 3.5 mm in spared areas. Biopsies were obtained; the corresponding H&E and keratin stains are provided (Image 3, composite photomicrographs A-B).
Based on the original radiographic imaging that led to the biopsy, what are the differential diagnoses?
