A 54 year old male with a past medical history of Type II diabetes mellitus and obesity was admitted for a few days history of severe pain over right upper quadrant accompanied by fevers, chills, nausea, vomiting and diarrhea. Physical exam revealed a palpable gallbladder. Ultrasound imaging showed a distended gallbladder with a thickened, edematous and hyperemic wall that was interpreted as acalculus cholecystitis. The patient underwent percutaneous drainage of the gallbladder with plans to undergo a cholecystectomy once the acute phase of his illness stopped. The gallbladder fluid was sent to microbiology for analysis.
Laboratory Findings
Anaerobic plates obtained from organisms growing in thioglycollate broth grew low, convex opaque white colonies. The organisms did not produce the classic double zone of beta hemolysis (Image 1). Gram stain of the culture showed gram positive bacilli that were “boxcar” shaped (Image 2). Aerobic plates had no growth. The organisms were catalase negative and non-motile. MALDI-TOF identified the organism as Clostridium perfringens.
Image 1. Growth on CNA plate in anaerobic environment Image 2. Gram stain from the anaerobic culture shows boxcar-shaped gram positive bacilli.
The patient was also placed on piperacillin-tazobactam while in the hospital. His condition improved and he was discharged home with a seven day course of cefpodoxime and metronidazole with a general surgery follow up appointment.
Discussion
Clostridium
perfringensis a gram
positive bacilli with blunt ends (boxcar shaped). These obligate anaerobes are
spore formers, however these are rarely seen. When seen, they produce
subterminal spores. These organisms cause of crepitant myonecrosis (gas
gangrene), gangrenous cholecystitis, septicemia, and food poisoning. They are present in large numbers as normal
microbiota in the gastro-intestinal tract of humans and animals, the female
genital tract and oral mucosa. Typically, infections are caused by endogenous
strains gaining access to normal sterile sites due to a predisposing factor
that compromise normal anatomy: surgery, trauma, or altered host defense
mechanisms (diabetes, burns, immunosuppression, and aspiration).
Penicillin is recommended in most infections,
however resistance has been reported. Optimal management of intra-abdominal
infection is to achieve appropriate source control and drainage is important.
Murray
P. Medical Microbiology. Seventh Edition. Elsevier; 2013.
-Angela Theiss, MD is a 3rd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
Outside the city of New Bern, in Craven County, North
Carolina, there is a particular system for residents to dispose of their
garbage. Locals must go to the nearest participating gas station and purchase
stickers which cost about $2.00 each. These stickers must be placed on each bag
of garbage generated in the household, otherwise they will not be picked up
during the weekly trash collection. In order to save money, a group of widows
has formed a club in which members scout out the open dumpsters in town
(usually behind stores or gas stations). Then they call and let group members
know where they can covertly dump their trash for free that week.
This story may seem funny, but for the most part, it is
true. I have no doubt this also occurs in other parts of the country where the
system for trash collection is similar. Why do people behave this way? Are they
purposely trying to circumvent the trash collection system in place or is the
system just not easy for locals to utilize? If you’re having difficulty getting
people to change safety behaviors (like PPE compliance) in your laboratory, you
might need to determine that for the systems you have in place and ask similar
questions.
In one laboratory the manager struggles with staff who work
part of the day in a clean office and another part in the lab itself. When the
employees go into the lab for brief periods, they often fail to don their PPE.
Upon further investigation, you would learn that staff are not allowed to keep
their lab coats on their chairs and that all PPE is kept in one lab store room
located on the opposite side away from the offices. The system is set up to reinforce
PPE non-compliance.
In another lab the manager placed a permanently-mounted
counter face shield in the chemistry department so that staff would be forced
to use it when popping specimen caps. Staff loaded instrument racks behind the
shield, but when they carried the racks over to the analyzers, their faces were
not protected from splashing. Exposures continued to occur. Here the system is
at play again. A face shield was put in place to change behaviors, but it was
only a partial solution. In order to protect staff fully here, they would need
goggles or a face shield that can be worn. Offer light-weight reusable or
disposable face protection that staff can use easily. Be sure to give them a
say in whatever option is chosen.
Sometimes the system issues are not apparent until there is
a safety event, and unfortunately, that can result in bigger problems. If your
training program does not include regular fire safety training, a small fire
situation may get out of hand quickly. Does your staff have experience handling
a fire extinguisher? Would they easily be able to put out a fire? Do they know
their evacuation routes and meeting places, and could they get there with ease?
What about the lab emergency management plan? Have staff participated in a
table-top drill so they have a basic understanding of how to respond during a
chaotic disaster? These are examples of some safety systems that need to be in
place to keep staff ready and safe at all times.
When people take shortcuts or find ways to circumvent the system, there is usually a pretty good reason, Often, it is the design of the system. In New Bern, elderly women can’t lift large heavy trash bags, so they use smaller bags. They don’t want to pay the same price for a garbage bag sticker that others are paying for big bags. There’s a problem with the system- and those ladies found a way around it. What problems do you see in your lab safety system? If you don’t know what they are, ask around. Staff will talk. It’s better to find out what the workarounds are now and to fix them before an injury or exposure occurs.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years
experience as a certified medical technologist. Today he is the
Laboratory Safety Officer for Sentara Healthcare, a system of seven
hospitals and over 20 laboratories and draw sites in the Tidewater area
of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Jennison Hartong, MLS(ASCP)CM,
PA(ASCP)CM, is a Pathologists’ Assistant who recently went to
Ethiopia to teach grossing techniques. The editors of Lablogatory asked her a
few questions about her experiences.
Lablogatory: How’d you get involved with ASCP’s Center for Global Health?
Jennison: Dr. Milner, Chief Medical Officer of ASCP, initially reached out to one of the pathologists at M.D. Anderson to inquire if any Pathologists’ Assistants (PAs) would be interested in attending a workshop in Nigeria. I reached out and expressed my interest in teaching grossing techniques rather than public speaking (not one of my strengths). Dr. Milner then told me about this opportunity in Ethiopia where pathologists were requesting advanced, gross training in lymph node dissections on breast and colon specimens. I immediately jumped at the opportunity to help in this way.
L: What were your motivations for going?
J: Whether with basic health needs or more complex areas like cancer treatments, I’ve always wanted to use my education and experience to help others and impact lives in areas around the world where certain aspects of healthcare may not be accessible. Before becoming a PA, I was a medical technologist and was always interested in working with Doctors Without Borders, however, I did not have the years of experience to apply. I decided to go to PA school and was disappointed to learn that Doctors Without Borders does not utilize PAs. I figured that dream would have to be accomplished another way, which was why I was so eager to work with the ASCP and their global health initiatives.
Another motivation for going on this trip was
experiencing the work and organizational skills required for making a trip like
this successful. I am currently finishing my second master’s degree in public
health with a focus in health policy and management. I was very interested in
learning everything I could about planning programs to help developing
countries as well as being able to network with like-minded health
professionals.
L: What did you hope to accomplish while you were there?
J: My main goal of this trip was to help advance Ethiopian residents and pathologists in certain grossing techniques. More specifically, I aimed to assist with lymph node dissections and, as it turned out, how to locate and sample the radial margin in colon cancer cases. I also wanted to experience a different culture than my own, step out of my comfort zone and challenge myself as a PA by teaching others. At the end of this experience, I can say that this trip was definitely a life changing experience and one I am extremely grateful for.
Image 1. Jennison (black scrubs) training residents from St. Paul Hospital to locate radial margins on colorectal cancer cases.
L: What did you learn about lab medicine in Ethiopia?
J: During my week in Addis Ababa, I quickly realized that it was up to me to make this trip as successful as possible. Never before in my professional career were all the decisions up to me, and at first, it was slightly uncomfortable. I was worried I would come across as too bossy or even condescending. However, after meeting Eshetu Lemma, the ASCP local representative, along with the other participants and experiencing their kindness and eagerness to learn, I was newly determined to make this trip an absolutely positive experience for everyone. I made some changes to the training sessions and after the first day, the rest of the week ran smoothly. I learned a lot about how lab medicine is practiced in Ethiopia. I learned that, in the case of a power outage, you carefully set your blade down and wait it out. I learned that resources like aprons and sleeves are not thrown away unless completely used up. I learned that due to cassette shortages, tissue submission is done quite thoughtfully- more so than in the United States. I learned that the overwhelming majority of cancer cases are presented at stage 4 due to issues surrounding resources, fear, myths, and lack of cancer education. But most importantly, I learned that the labs in Addis Ababa, Ethiopia, are doing an amazing job with the resources they are given and are eager for opportunities to positively impact patient care.
L: Is what you learned there applicable to your work in the States?
J: I’ll take what I learned there and incorporate it into my work here in the States. I’ve gained confidence in my ability as a health professional and reignited my passion to help others.
To put it simply, this trip has been life
changing. It has allowed me to experience and accomplish a lifelong dream for
which I am forever grateful. I’m hopeful that my future holds more
opportunities to serve other communities and help strengthen cancer programs in
developing countries.
Image 2. View from St. Paul Hospital.
-Jennison Hartong,MLS(ASCP)CM, PA(ASCP)CM is a board certified Pathologists’ Assistant, specializing in surgical and gross pathology working mainly in oncology cases. Before attending graduate school, she worked as a Medical Laboratory Scientist (MLS) at Lurie Children’s Hospital of Chicago, Illinois. Upon graduating, Jennison started working at Memorial Sloan Kettering Cancer Center. In 2018, she relocated to Houston and currently works at M. D. Anderson Cancer Center in Houston, Texas. In May of 2019, Jennison will graduate with a second Master’s in public health with a focus in health policy and management from New York Medical College. She plans to use her extensive lab experience and newfound knowledge of public health to help bring basic healthcare to communities that would otherwise not have access to these necessities.
As a part of my
Molecular Genetic Pathology fellowship, we experience a clinical component to
training in addition to all of the laboratory training we receive. This last
month, I rotated through Cancer Genetics, where genetic counselors discuss
genetic testing with patients with a personal or family history of cancer. The
counselors describe the process of genetic testing and help chose genetic tests
to look at the patient’s risk for an inherited cancer syndrome.
Patients are
looking forward to the certainty that will come from a genetic test, because it
is the wave of the future and they think you can learn so many things from your
genetics. The truth, however, can be much less clear. Up to 30% of people receive
a Variant of Uncertain Significance (VUS) as their genetic test result. This
rate increases as larger panels are test more genes.
Figure 1. A set of genes and associated cancer types tested by a hereditary cancer genetic test. (Taken from Myriad MyRisk Gene Table.)
A VUS
represents a variation in a person’s gene that doesn’t have enough information
to say that it is benign or pathogenic. This gray zone is very uncomfortable
and confusing for patients and providers alike. There are several cases where
someone acted on a VUS as if it were a pathogenic variant and ended up having
radical interventions like a bilateral mastectomy.
We know that as
scientific and medical knowledge increases, our ability to reclassify these
variants improves. For laboratories, this means periodic reanalysis of previously
reported variants. If this process is not properly set up, it can be very
laborious and extensive. Furthermore, not only was a timeline for variant
reanalysis unknown, but also the likelihood of variants becoming upgraded or
downgraded had not been described.
Two recent
studies helped provide some answers to these questions. The first, published in
JAMA, comes from the cancer genetic group I was working with, led by Dr. Theo
Ross M.D. Ph.D., worked in conjunction with Myraid (Lab that first started
testing the BRCA genes, and now tests many more) to determine how often
variants were reclassified. Looking at 1.1 million individuals tested at
Myriad, the average time to reclassification for a VUS was 1.2-1.9 years (Mersch
J et al Jama 2018). Additionally, 90% of VUS were downgraded to benign/ likely
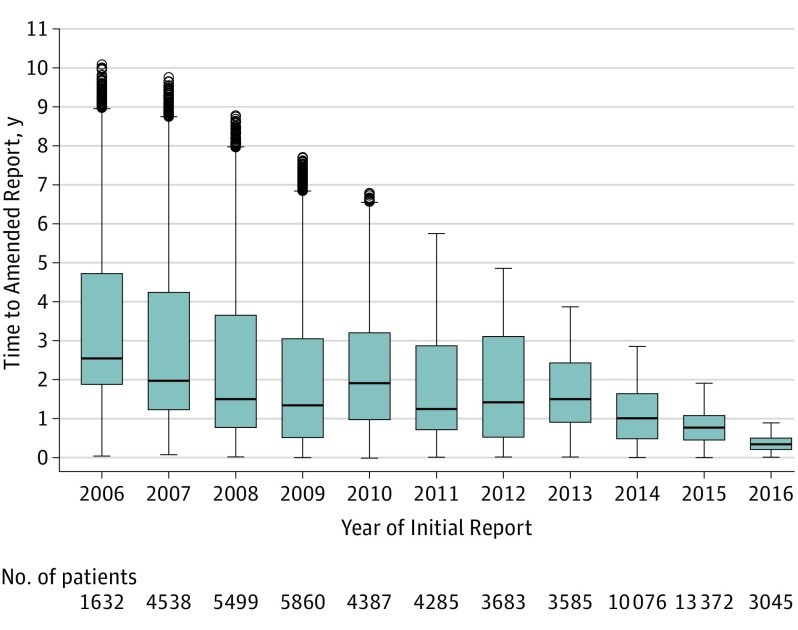
benign representing 97% of patients with a VUS. This figure from the paper
shows how the time to issuing a reclassification (amended report) has decreased
(Figure 2).
Figure 2. The time to sending an amended report is shown by the year the report was first issued. From Mersch et al. JAMA 2018.
I worked on the
second study, which looked at variant reclassification in childhood epilepsy
genetic testing (SoRelle et al JAMA Peds 2019). The results, published in JAMA
Pediatrics, also found most patients had a VUS reclassified to benign/likely
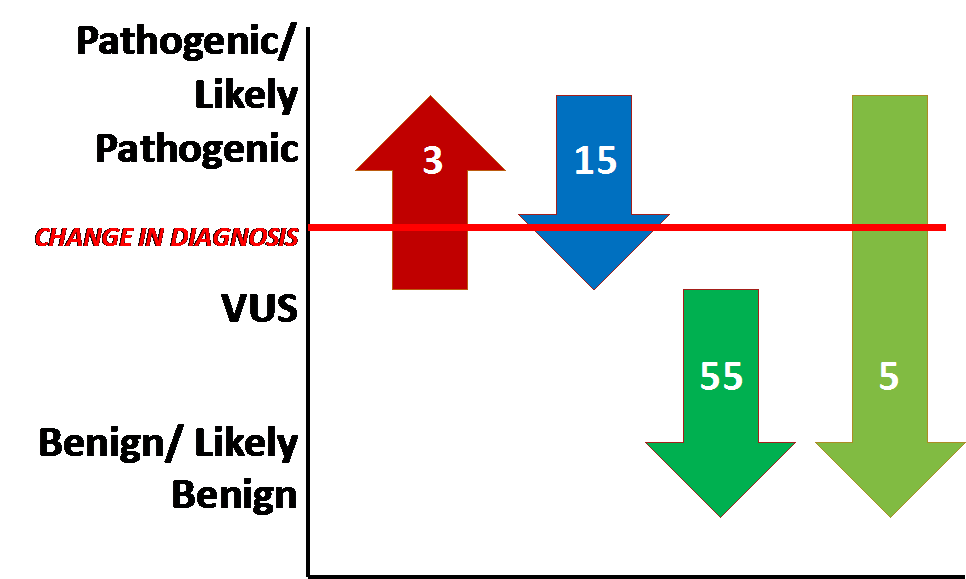
benign. However, several clinically significant changes (reclassified to or
from pathogenic/ likely pathogenic) occurred as well (Figure 3).
Figure 3. Patients with reclassification of gene variants from each category. Arrows that cross the red line represent an instance where a change in diagnosis would result from variant reclassification. Seven patients had both a pathogenic or likely pathogenic variant and VUS reclassified and are only represented once.
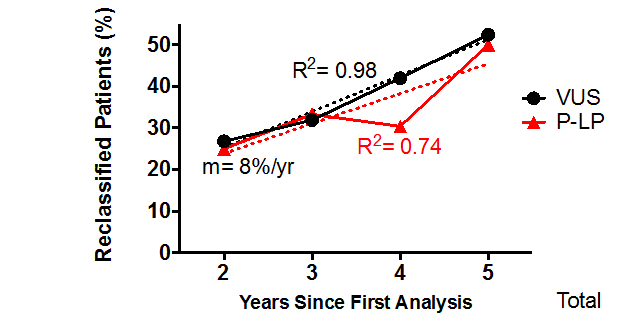
Furthermore,
there was a linear relationship between the time the test was reported and the
rate of variant reclassification (Figure 4). We found that 25% of patients with
a VUS would experience a reclassification within 2 years.
Figure 4. Reclassification rate is plotted as the fraction of reclassified variants for each year testing was performed (VUS= black line, pathogenic or likely pathogenic= red line). Solid lines represent patients with a reclassified result and dotted lines are extrapolated slopes.
Overall, the
conclusions of the two studies are somewhat similar:
Most
patients with a VUS experience a downgrade reclassification to likely benign or
benign.
Variant
reclassification should be performed at least every 2 years
Rates
of reclassification may differ by disease type. Investigation by a similar
study design should be performed in other genetic diseases.
SoRelle
JA, Thodeson DM, Arnold S, Gotway G, Park JY. Clinical Utility of
Reinterpreting Previously Reported Genomic Epilepsy Test Results for Pediatric
Patients. JAMA Pediatr. 2018 Nov 5:e182302.
-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the
University of Texas Southwestern Medical Center in Dallas, TX. His
clinical research interests include understanding how the lab intersects
with transgender healthcare and advancing quality in molecular
diagnostics.
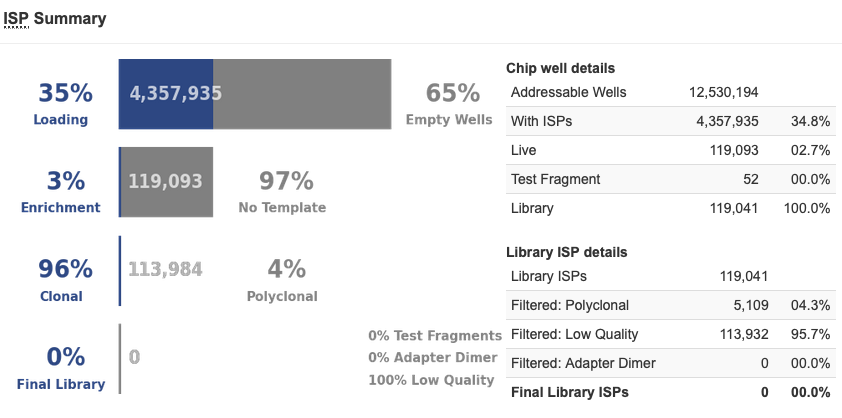
Ah, the blue chip – not much fun to see after spending a day
preparing the libraries and running clonal amp overnight. There are a couple possible explanations for
a blue chip, and you can figure them out by looking at the metrics of the
run.
Test Fragments
The test fragments serve as a
control for the sequencing run. They are
spiked into the mixture of library ISPs before they are loaded on the
chip. These will allow you to figure out
where the problem occurred if you encounter a blue chip. If the Test Fragments are detected and are of
sufficient quality, then this means the sequencing run worked and the problem
most likely occurred before sequencing, during library prep or clonal
amplification. If the Test Fragments are
not detected, then it could mean one of two things – one – the clonal
amplification did not work for either the library or the Test Fragment ISPs, or
– two – the sequencing run was somehow at fault. Let’s take a look at both examples.
Troubleshooting a Blue Chip
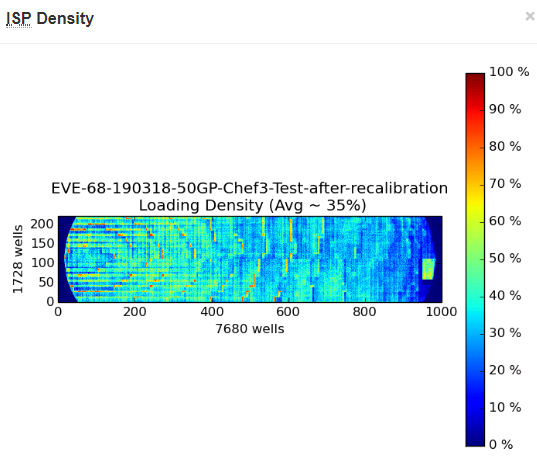
In the event you see a blue chip,
first, check to see what kinds of ISPs showed up after the analysis. For the chip pictured above, there were ISPs
that had product on them, as you can see in the Live category (6,475,553 ISPs
or 95.3% of the ISPs, shown in the screenshot below). This means clonal amp was successful for a
small number of the library ISPs. Next,
there were also Test Fragments detected, at 433,392 ISPs or 6.7% of the total
ISPs. Scroll down to the bottom of the
page, and you will see how the Test Fragments sequenced. We like to see the Percent 50AQ17 and Percent
100AQ17 at least in the 80’s, but even still, you can see that these were
detected and were sequenced. Because of
this, the sequencing run looks to be fine, so most likely the problem occurred
before sequencing. In this case, we
believe the library prep did not yield the expected 100pM concentration, so the
library pool was over-diluted prior to clonal amplification. The library prep was repeated, and clonal
amplification was run on the new pool of libraries, and the sequencing was
successful.
In this next example, we have the
other possibility. This chip was blue as
well (this is a 520 chip, instead of a 530, to explain the different sized
pictures).
First, there are only 2.7% Live
ISPs, so even lower than the chip above.
But the even stranger thing was that there were 0.0% Test Fragments, and
at the end of the analysis, there were absolutely no ISPs left to be analyzed,
library or Test Fragment. This was the
only time we had ever seen a chip like this; generally, if we had blue chips,
they were like the previous example. We
looked at our library pool quant and it was in the expected range, so we did
not believe it was a library prep issue.
The sequencing initialization was successful and did not have any
errors, so we did not believe it was a sequencing problem. We repeated clonal amplification with the
same library pool and had successful sequencing. In speaking with our Field Application
Scientist, it was decided it must have been a failure of one of the reagents of
the clonal amplification – either a Taq was not present or something, so the
clonal amplification never occurred, or something similar.
Hopefully you will not experience
too many of these blue chips, but if you do, I hope you are a little more
prepared to troubleshoot! Happy
sequencing!
-Sharleen Rapp, BS, MB (ASCP)CM is a Molecular Diagnostics Coordinator in the Molecular Diagnostics Laboratory at Nebraska Medicine.
Maryam Zenali1*, Dmitriy Akselrod2, Eric Ganguly3, Eswar Tipirneni4 and Christopher J. Anker5*
1
Department of
Pathology, 2 Department of Radiology, 3 Division of
Gastroenterology, and 5 Division of Radiation Oncology, The
University of Vermont Medical Center (UVMMC), Burlington, VT and 4
Department of Hematology Oncology, Central Vermont Medical Center (CVMC), The
University Of Vermont Health Network, Adult Primary Care, Berlin, VT
*corresponding authors
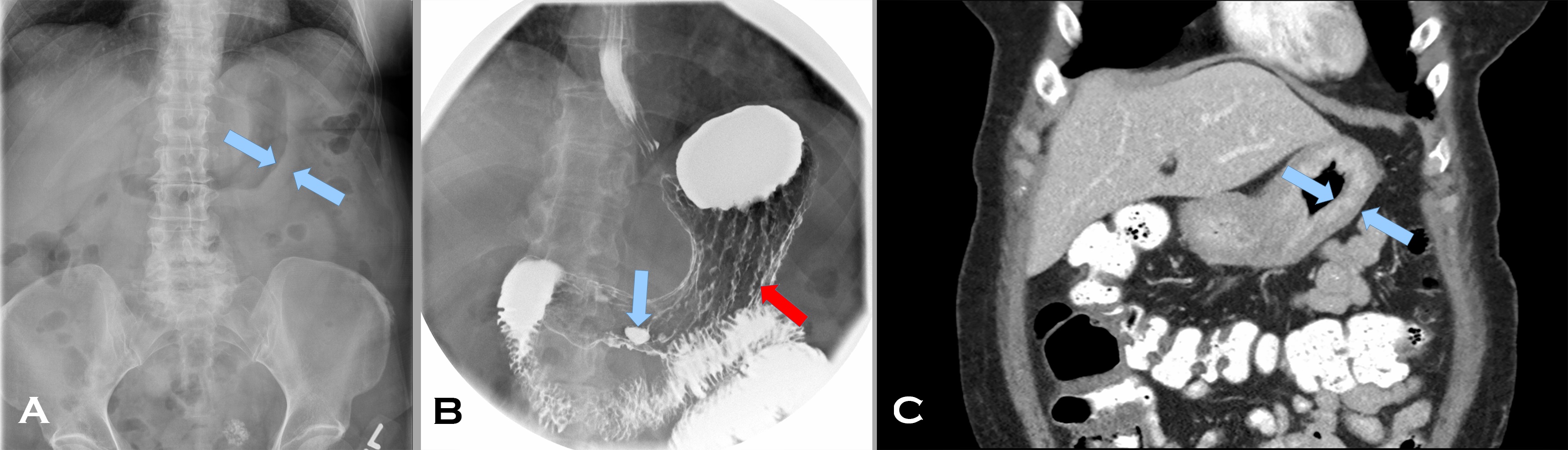
A 57 year old woman with a personal and family history of breast cancer presented with early satiety and dysphagia for 5 months. Her abdominal computed tomography (CT) scan (Image 1 A) showed marked thickening of an apparently featureless gastric wall (A, blue arrows indicating the mucosal [rightward pointing] and serosal [leftward pointing] aspects of the gastric wall). Prominent gastrohepatic lymph nodes were noted as well. Her fluoroscopic upper GI study (Image1 B), following administration of barium and effervescent crystals (a double contrast effect to allow for mucosal evaluation), showed thickened rugal folds (B red arrow) and pooling of barium within an antral ulcer (B blue arrow). A subsequent CT scan (Image 1 C) after administration of intravenous and enteric contrast, confirmed marked diffuse gastric wall thickening (C blue arrows again indicating the mucosal [rightward pointing] and serosal [leftward pointing] aspects of the gastric wall) (Image 1, composite radiographs A-C).
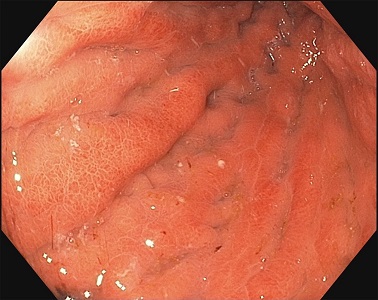
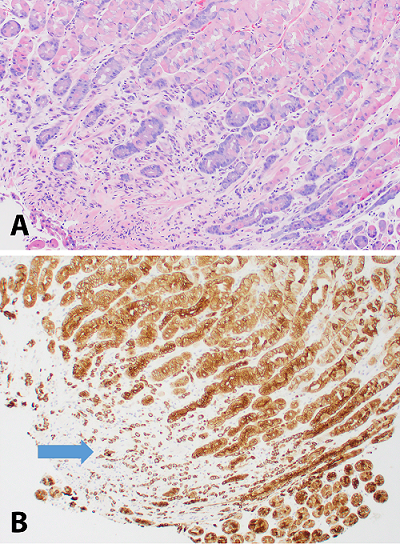
The gastric body distended poorly with insufflation and demonstrated thickened, erythematous, edematous folds with erosions (Image 2, endoscopy image). On endoscopic ultrasound, the total thickness of the stomach was 12 mm with expanded wall layers in the proximal stomach to the antrum and a thickness of 3.5 mm in spared areas. Biopsies were obtained; the corresponding H&E and keratin stains are provided (Image 3, composite photomicrographs A-B).
Image 1. Composite radiographs.
Image 2. Endoscopy image.
Image 3. Composite photomicrographs.
Based on the original radiographic imaging that led to the biopsy, what are the differential diagnoses?
A 19 year old woman with no significant past medical history
presented to an outside clinic with psychological distress after passing a worm
per rectum. She had no other complaints or symptoms.
Image 1. Eggs are spherical, 31 to 43 μm in diameter, with a thick yellow-brown (bile-stained) shell having radial striations and contain a hexacanth oncosphere (Image courtesy of: Fred Patterson, Parasitologist).Image 2. Adult proglottids are longer (up to 20 mm) than they are wide (up to 7 mm) and have a genital pore (*) at the lateral margin.Image 3. Formalin-fixed paraffin-embedded H&E stained section of a proglottid’s lateral uterine branches on each side of a central uterine stem (20x).
Discussion
Adult cestodes (tapeworms) have long, ribbon-like bodies
made up of proglottids (egg-producing segments) that develop at the posterior
of a scolex (specialized structure for attachment to the small intestine of a
host). Taenia has 32 species, 2 of
which are medically important for causing taeniasis: Taenia saginata and Taenia
solium (beef and pork tapeworm infection, respectively). These parasites
are distributed worldwide, with T.
saginata being more common than T. solium.
The lifecycle of Taenia
involves adult, egg, and larval stages. Adults release gravid proglottids and
eggs that are passed in feces. The eggs reach pasture land via soil or water
and are ingested by an intermediate host. For T. saginata, the intermediate host is a herbivore (cow), as eggs of
T. saginata do not infect humans, and
for T. solium, the intermediate host
is a pig, human, or other animal. Ingested eggs hatch and release the hexacanth
oncosphere (6-hooked embryo) that can penetrate tissues. Over 2 to 3 months,
infective cysticerci (0.5 to 2.0 mm in diameter larvae) develop in muscles. Of
note, only T. solium can cause
cysticercosis (extra-intestinal larval forms within human tissues, ie. the
human becomes the intermediate host) and this can be life-threatening if
cysticerci invade the brain. When humans consume raw or undercooked beef/pork
meat that is infected, cysticerci will attach to the small intestinal mucosa
and, over 3 to 5 months, mature into the adult form. The adult T. saginata can reach 4 to 12 meters in
length and the adult T. solium can
reach 1.5 to 8 meters in length. Adult tapeworms can live within intestines for
over 25 years while gravid proglottids and eggs are passed in stool.
Infections are usually asymptomatic or cause mild
indigestion, anorexia, and abdominal discomfort. The eggs can be identified by
ova and parasite examination (Figure 1) or a cellulose tape preparation of
perianal skin. The oncosphere must be visualized to avoid misidentifying a
pollen grain. However, eggs of Taenia
species and Echinococcus species are
indistinguishable. Diagnosis is also made by recovering gravid proglottids from
the anal opening or passed in feces (Figures 2 and 3). Distinguishing the two
species can be done by examining gravid proglottids for the number of lateral
uterine branches present on one side of a central uterine stem. T. saginata have 15 to 30 lateral
uterine branches while T. solium have
7 to 13 branches. Both species have a small anterior scolex (measuring 1 to 2
mm in diameter for T. saginata and 1
mm in diameter for T. solium) with 4
suckers. Definitive identification is possible since T. solium’s scolex has a rostellum (crown) with 2 rows of hooks
whereas T. saginata’s scolex bears no
rostellum or hooks. Treatment is a single dose of praziquantel and successful
treatment is defined as passing zero proglottids over 4 consecutive months.
-Adina Bodolan, MD is a 3rd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
Generation Y is coming and they are coming in strong! It is
fast becoming the world’s largest working generation and their impact on the
workforce will become even clearer in the next few years. These digital natives
find communication natural, in any shape or forms it comes. They prefer texting
and instant messaging, but also appreciate face-to-face meetings and
hand-written notes. They use social media for both personal and professional
use and consider it essential to know how and where to access information.
Instant gratification has become one of this generation’s key values, because
they grew up with the world of information at their fingertips. They value
professional development and feedback and they are at work to learn and grow.
When working with a Millennial the first step is to show
them that you respect them and what they bring to the table. This generation
has received more negative attention than other generations, but they have a
tremendous amount to offer to the workplace (as do all the other generations).
They value collaboration and learning opportunities, so they are typically
quick to adjust when giving constructive feedback. Because of their
collaborative approach, they value inclusion and Social Media to bring people
together. They are well versed in finding information and can typically solve
smaller technological issues without any help.
This generation is focused on having their work mean
something, to have a purpose that is larger than simply getting a paycheck.
They dislike long email and voicemails and anything that is a waste of paper.
They appreciate flexibility and sending documents electronically. They
experiences high academic pressures, so they are comfortable working in a
fast-paced environment. They are comfortable multitasking and handling multiple
projects simultaneously.
Millennials who work in larger organizations are on the
brink of entering leadership positions. However, there are many self-starters
who have had to learn leadership skills along the way. Because this generation
values collaboration, leaders tend to encourage group work and giving people an
acknowledgement for trying. They dislike people who are afraid or do not want
to learn new technology and cynicism as they are a generally very positive
generation.
When working with Millennials, note that they respond well to a participation work environment so ask for their input and suggestions. Be open about any processes, systems, and share information freely. Provide them with lots of feedback to help them learn and grow. Millennials respond well to a faster pace work environment, so do not try to slow them down. They dislike formality and stiffness, so allow flexibility whenever possible. For example, invite them to provide input for their own goals and do not hover over them. Give them multiple things to work on simultaneously so that they can go from project to project when their energy shifts. This generation is crucial to bring your organization to the next level, so mentor them, help them grow and develop and you get their dedication, passion, collaboration, and positivity in return.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
What’s the purpose? That’s the question that most Gen Ys, or
commonly known as Millennials, ask of their job. Why am I here? Can I make a
difference in the world if I remain doing what I am doing?
The Baby Boomers worked because they felt an obligation to
put in a hard day’s work whether they liked doing what they were doing or not. It
was a job. The Generation Xers introduced a focus on work-life balance, which
was not the case for the Baby Boomer. The Boomers never heard of the concept of
“work-life balance” until their children, the Gen Xers, made it a job
requirement and reality.
As for the Millennials, they need to really believe in their
job and what they are doing. Millennials ask questions that the Boomers and Gen
Xers wouldn’t think of asking. This is often misinterpreted as being lazy or
looking for the easy way out. This is not the case. The Millennials took the
best of their predecessors. Most Millennials have a good work ethic and they definitely
look for balance. However, they’re also searching for a purpose.
My favorite story of a Millennial is centered on the importance of taking lunch at work. This topic surfaced from a Roundtable Discussion with laboratory professionals last October 2018, at the ASCP Annual Meeting in Baltimore. The actual topic for this Roundtable Discussion was “diversity.” However, that quickly changed when the nine people at the Roundtable focused on generational differences. This roundtable was rich in generational diversity. The table was comprised of Boomers, Gen Xers and Millennials. Boomers stated that they found it both necessary and easy to work through lunch. Why? It’s because they pride themselves in their incredible work ethic. The Boomers praised themselves for being better than “most Millennials” who often don’t and won’t work through lunch. Instead of that mindset, perhaps the better approach would be “What can we learn from Millennials in the work place?” That answer is “purpose and balance.”
-Catherine Stakenas, MA, is the Senior Director of Organizational
Leadership and Development and Performance Management at ASCP. She is
certified in the use and interpretation of 28 self-assessment
instruments and has designed and taught masters and doctoral level
students.
I had the pleasure of talking recently with Danny Milner, Jr., MD, MSc(Epi), who serves as the Chief Medical Officer of ASCP. He has worked to improve diagnostic access and improve laboratory medicine services in low- and middle-income countries [LMICs] his entire career. I recently read his book for which he served as editor for titled “Global Health and Pathology.” This highly informative compilation of articles written by the foremost experts in the field is a MUST READ for anyone interested in global health! You can order your copy here: https://www.elsevier.com/books/global-health-and-pathology-an-issue-of-the-clinics-in-laboratory-medicine/milner/978-0-323-58158-5.
After reading the book, I hoped to learn more about Dr.
Milner and how he became a leader in global health and pathology. Below you
will find his fascinating narrative of his career and his reflections on the
importance of providing high quality pathology services worldwide.
Q: Dr. Milner,I’m curious to know where your service in
global health began and how your career in pathology has intersected with that?
A: Truly, many
events occurred that were serendipitous in shaping my career and life. I grew
up very poor in a rural community in Alabama, in an area known as the
“black-belt” of the southern states due to the rich black soil found there.
This area was home to many of the relocated former slaves after the end of the
civil war and is now home to a 50/50 mix of Caucasian and African-American members
of the community.
Towards the end of high school, I was awarded a scholarship
for high achievement and a scholarship geared to support healthcare
careers. At the award ceremony, a person
giving me an unrelated award knew of my scholarship for pre-med and said to me
and the crowd, “go become a doctor”. When I was in college, I worked as a
nurse’s assistant for a physician and became interested initially in primary
care . After some careful consideration, I decided to embark on a path that
would take me to medical school, finishing my pre-med requisites and graduating
in three years. I was accepted to the MD/PhD program at the University of Birmingham
[UofB] wanting to do my PhD in Medicinal Chemistry. Unfortunately, this
particular PhD wasn’t allowed, so I decided to pursue a MD only.
In medical school, I decided to slow down my fast track through
school– so I applied to a post-sophomore fellowship in Pathology and at the
same time applied for a summer program offered by UofB that entailed working in
a clinic in The Gambia. This would be the first time that I had traveled outside
the United States. I first went to Africa, with my fellowship to follow on my
return.
In The Gambia, I lived in a compound with 12 people in an extremely
rural area with no running water or electricity. I spent four weeks working in
a clinic with a Gambian doctor, seeing patients without the use of diagnostics.
I was traumatized by the extreme suffering of the patients we saw. My take away
from the experience was the idea that it would have been so much easier to help
had there been any sort of
diagnostics available – a malaria smear, a microscope, anything that could have
helped us do a better job than we were doing.
When I returned from Africa, I started my post-sophomore
fellowship and my first rotation was autopsy. There was a neuropathologist
there named Angelica Oviedo, and she had just gotten back from Malawi. Hearing
about my recent trip to The Gambia, she encouraged me to pursue more work in
global health. She put me in contact with Terrie Taylor – who is an internal medical
physician who has been working in Africa since 1986. It was in the 1990’s and she
had just started a cerebral malaria autopsy study which would become the
largest study on this topic in the world.
This post-sophomore fellowship really inspired me to pursue
pathology. I was thrilled to be offered a position at the Brigham and Women’s
in Massachusetts for pathology residency.
I finished medical school by spending time in Germany and then under the
supervision of Terrie Taylor in Malawi working on the cerebral malaria autopsy
study. I continued to work with her for thirteen years following this.
In residency, it was a natural fit for me to gravitate
towards all things related to global health which meant a focus on infectious
diseases. I continued to work in Africa and traveled there 4-5 times during
residency, scrounging together any time and any money that I could to try to
help. It was during my second time in
Malawi, around 2001, that I was surprised to find that all the cases crossing
the surgical pathology bench were cancer – there was nothing but cancer, and it
was often very advanced. This was 15 years before the WHO resolution on cancer.
I was suddenly very interested in this aspect of care. Up until this point, I
was heavily focused in infectious disease, and how this related to oncology,
but now I wanted to really focus on cancer. I was not encouraged by my elders
to try and tackle this because they said, “they are all going to die anyway.”
Fast forward, I finish a fellowship in Microbiology and am
joining the Brigham as faculty to work in infectious disease pathology. During
this time, I continue to go to Malawi and I am continuously signing out cancer
cases for Africa. This was tragic since there was no intervention at that time,
and every case was essentially a death sentence. The first oncologist did not
arrive in Malawi until somewhere around 2008-2009.
During my time at the Brigham, Partners in Health [PIH]
began sending tissue biopsy cases to us to diagnose. Every year, the cases
increased more and more. Because cancer started to become the majority, PIH
decided to strategize the best way to meet this need. Larry Shulman, the lead
for PIH based at Dana-Farber in Boston, reached out to me to build a pathology
laboratory in Haiti, but since that idea was quickly followed by an epidemic of
cholera, it was decided to build a pathology lab in Rwanda instead – this was
in 2011. After a massive effort entailing equipment installation, capacity
building, infrastructure, and staff training, Butaro Cancer Center officially
opened 6 months later. With the help of a few other volunteers, we continued to
run the lab remotely using static image telepathology. In 2016, a full-time local
pathologist took over the lab and ASCP brought in whole-slide telepathology
services.
In 2015, I met Blair Holladay in person for the
first time. He shared his vision for ASCP to expand their global outreach and
we had a healthy discussion about the details of making it happen. Blair asked
me to volunteer to become part of the team, and I worked together with ASCP to
launch the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
The project grew and ASCP reached out to recruit me to work as the Chief Medical
Officer and lead the global health team. I was excited to have the opportunity
to work in global health full time.
Dr. Milner (left center, front row) with members of the Partners Initiative local team at the 2017 ribbon cutting ceremony to celebrate the opening of the second telepathology lab in Rwanda.
Q: Why is pathology
the essential cornerstone of global health?
A: First, you
should consider how important the laboratory is in medicine. An often-quoted
study says approximately 70% of the clinical decision making is based on
laboratory results. In certain subspecialties of medicine, like surgery or
oncology, these clinicians are nearly 100% dependent on the laboratory for delivering
care. In fields like psychiatry, it is going to be much less dependent on the
laboratory. Even so, it is reasonable to say that almost all medical decisions
are best informed by high quality laboratory results.
Starting with that statement, the laboratory is what allows
clinicians in certain fields to function. In the field of cancer, which is a
major problem in LMICs, you cannot treat the patient without a diagnosis – and
the diagnosis must come from the laboratory.
Q: Historically, pathology
hasn’t always been associated with creating global health solutions. Why do you
think that is now that we know it is an essential component of building health
systems?
A: It’s a general
challenge in global health that pathologists haven’t been involved as much as
they could be. This could be due to multiple reasons. The need for pathologists
to serve in low- and middle-income countries hasn’t traditionally been
recognized. This may be due to a disconnect in understanding our potential to
make an impact. We, like surgeons and radiologists, require electricity,
supplies, and resources in order to volunteer in very remote settings
worldwide. This is unlike clinicians and emergency medical doctors for
instance, that can see patients without extensive resources available – they
are more readily available to serve in small, remote communities. An exception
would be the use of cytology which can, with very limited resources, be
extremely effective even in remote areas. However, as a specialty, pathologists
are typically able to serve in larger cities in LMICs and, there, have an
enormous impact. So, there are plenty of opportunities for pathologists to
practice their specialty in improving global health and make an impact.
It may also be that people and their families have concerns
about their safety, or they don’t have the support of their institution in
terms of time, or they may not feel they have a connection to a potential site.
The desire may be there but there are perceived obstacles.
ASCP works to create relationships and facilitate connections, as well as allay fears for safety concerns. We also offer institutional support, for example, we provide a letter of explanation and support for our Trainee Global Health Fellows. We try to bridge the gaps for people to feel that they have the ability and are empowered to volunteer, remove the barriers to participation, and make it as easy as possible for people to do so.
-Dana Razzano, MD is a Chief Resident in her third year in
anatomic and clinical pathology at New York Medical College at
Westchester Medical Center and will be starting her fellowship in
Cytopathology at Yale University in 2020. She was a top 5 honoree in
ASCP’s Forty Under 40 2018 and was named to The Pathologist’s Power
List of 2018. Follow Dr. Razzano on twitter @Dr_DR_Cells.
An 83 year old man with rapidly growing squamous cell carcinoma of the left temple and scalp underwent workup prior to surgery which showed an elevated PTT and a slightly elevated PT. The patient denied a history of abnormal coagulation tests or excessive bleeding or bruising. He also noted that he had previous surgeries including dental procedures without excessive bleeding. In addition, he did not have a history of clot formation.
Lab Values
Differential
Diagnosis
At
this point, the differential diagnosis for a prolonged PTT included the
presence of an inhibitor (specific factor inhibiter vs. non-specific lupus
anticoagulant) vs. reduced levels/activity of intrinsic pathway factors that
would prolong the PTT, but would not significantly affect clot formation. This
would include factors XI and XII.
Additional
Testing
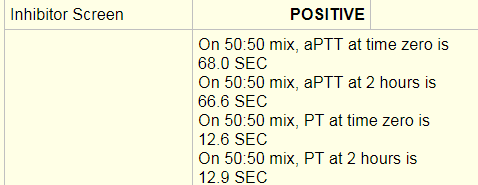
An
inhibitor screen/mixing study was performed and was positive. An inhibitor
screen is performed by mixing the patient’s plasma with pooled normal plasma
and running a PT or PTT. If the PT/PTT
corrects than the screen is negative. This means that a factor or factors were
deficient in the patient’s plasma and were replaced with the pooled normal
plasma resulting in a correction of the PT/PTT. In this case, a PTT at time 0
of 68 seconds and a PTT at 2 hours of 66 seconds was a failure to correct and
indicated that an inhibitor was present, thus a positive result was entered.
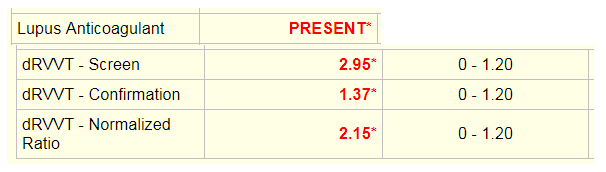
The
dilute Russell’s viper venom time (dRVVT) was used to test for a lupus
anticoagulant. The screening test is performed by adding Russell viper venom,
which directly activates coagulation factor X in the presence of calcium and a
phospholipid poor reagent to the patient’s plasma and calculating time to clot.
The confirmation test is the same assay with added excess phospholipid. In the
presence of phospholipid dependent antibodies, the time to clot will be shorter
for the confirmation test. The screen and confirmation ratios are normalized
ratios (NR) of the patient sample result in seconds divided by the mean of the
normal range in seconds. If the screen is <1.20, the confirmation test will
not be run. If the screen is greater than 1.20 as seen here, the confirmation
test will be run. The end result is reported as a normalized ratio of the
screening test over the confirmation test. If the NR is greater than 1.20, than
a lupus anticoagulant is reported as present.
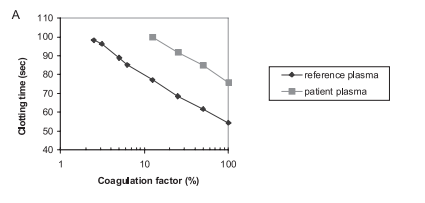
Specific
factor assays are performed by mixing the patient’s plasma with substrate
plasma that is severely deficient in the factor being measured. Factor
deficient plasma would be expected to give a prolonged clotting time. When
patient plasma is mixed with factor deficient plasma, the clotting time will shorten
and the degree of correction is proportional to the factor level in the
patient’s plasma. The clotting times for the patient sample are compared to a
reference curve. The reference curve is made with dilutions of normal plasma
(containing 100% factor) added to factor deficient substrate plasma. All tests
are run with 3 dilutions at 25%, 50% and 100% and curves are checked for
parallelism errors, which might indicate the presence of an inhibitor. For this
patient, factor XI was initially resulted as 1%, which would indicate a factor
deficiency.
This
is an example of a factor assay that shows parallelism. The reference plasma
calibration curve and the patient plasma are parallel lines. 1
Analysis
From the
results, it initially appeared that there was both a lupus anticoagulant and a
factor XI deficiency. However, it would be odd for a patient with no reported
coagulation abnormalities to suddenly have both a lupus anticoagulant and a
factor XI deficiency. The raw data from the factor XI assay was obtained.
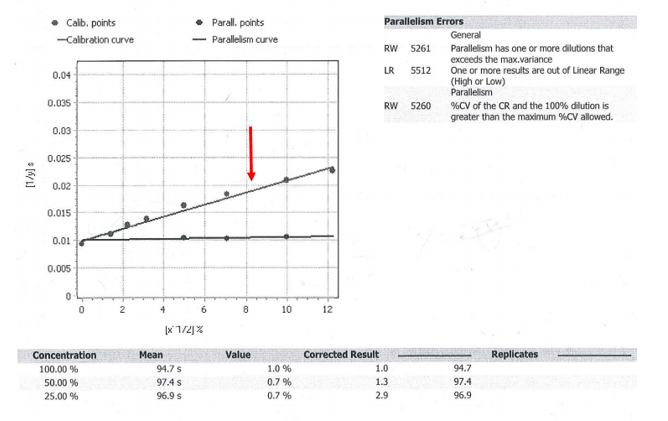
Upon
review, the factor XI assay did show parallelism errors. Parallelism is tested
by performing serial dilutions of a standard with known normal concentrations
of factor and recording the time to clot. This line is shown with the red
arrow. In contrast, the patient sample appears to be a flat line that is not parallel
to the calibration curve. Parallelism errors were flagged because from the 50%
to 25% dilution, the corrected results more than doubled. If there is a >20%
change between dilutions, this indicates possible interference and additional dilutions
should be run to dilute out the inhibitor. The 25% dilution had a corrected
result of 2.9, which was greater than a 20% increase from the 50% dilution
result of 1.3. Once more dilutions were performed; the Factor XI level was
ultimately close to 100%.
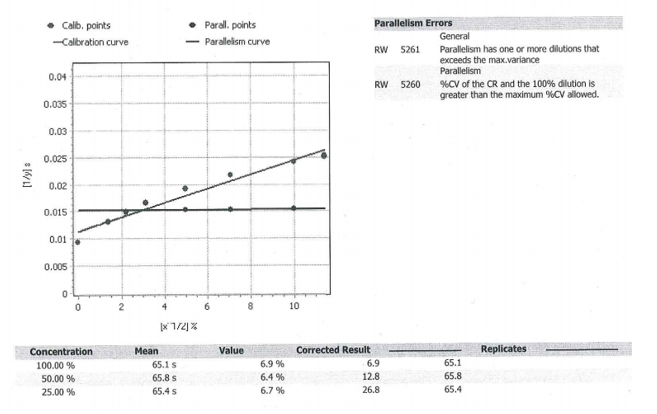
Additional
factors were checked to see if they also increased with dilutions. This would
add support to the theory of a non-specific inhibitor (lupus anticoagulant)
that was affecting all of the factor levels, rather than a specific factor XI
inhibitor or a concurrent factor XI deficiency. The curve from factor IX
(below) showed a similar phenomenon. As the sample underwent additional
dilutions, the corrected result increased significantly (from 12.8 at 50% to
26.8 at 25%). Ultimately, the factor level was close to 82%.
The
curve from factor VIII also showed low results to begin with and ultimately
normal levels with additional dilutions. Altogether, this supported the
presence of a strong lupus anticoagulant that was non-specifically interfering
with all of the factor levels and prolonging the PTT.
Discussion
A
prolonged PTT can be caused by many factors. In a patient without a bleeding
history, lupus anticoagulant and certain factor deficiencies are high on the
differential. The most common specific factor inhibitors are to FVIII and FIX.
These generally arise in hemophilia patients treated with factor concentrates.
It is very rare for a patient to develop an inhibitor to factor XI or XII.
Factor
XI acts in the intrinsic pathway of the clotting cascade and is important for
hemostasis. Deficiency of factor XI is rare and mainly occurs in Ashkenazi
Jews. Generally, it does not cause spontaneous bleeding; however excessive
blood loss can occur during surgical procedures.
Lupus
anticoagulants are directed against proteins that complex with phospholipids.
Although they prolong the PTT, they are associated with an increase in
thrombosis rather than bleeding. In addition to interfering with the PTT assay,
lupus anticoagulants may interfere with individual factor assays and result in
non-parallelism (patient curve is not parallel to calibration curve) as seen in
this patient. With increasing dilutions, the lupus activity will be
disproportionately neutralized and the coagulation factor activity will
increase in a non-parallel manner. 1
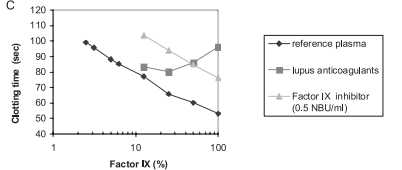
In a letter to the editor by Ruinemans-Koerts et al., they performed a set of experiments to investigate whether lupus anticoagulants vs. individual FVIII and FIX inhibitors can cause non-parallelism in the one-stage factor assay. Non-parallelism was only detected using lupus sensitive reagents in plasma with high titers of lupus anticoagulants. The FVIII and FIX inhibitor containing samples both resulted in curves that were parallel to reference sample.
This
curve shows that the factor IX inhibitor line is parallel to the reference
plasma, while the lupus anticoagulant line is not. 1
Ultimately,
this demonstrates the importance of running dilutions and being aware of
parallelism errors when performing factor assays. This is especially important
in patients with known or suspected lupus anticoagulants. In this case, the
unlikely presence of a FXI deficiency with no previously reported coagulation
testing abnormalities or bleeding history raised the suspicion of an inhibitor
interfering with the factor assay. With a concurrent positive inhibitor screen
and lupus anticoagulant test, as well as interference demonstrated with
multiple factor assays, the best unified conclusion was a strong lupus
anticoagulant. 1
References
Ruinesman-Koerts,
J., Peterse-Stienissen, I, and Verbruggen, B. ”Non-parallelism in the one-stage
coagulation factor assay is a phenomenon of lupus anticoagulants and not of
individual factor inhibitors. “ Letter. Thrombosis
and Hemostasis, 2010, p.104.5.
–Chelsea Marcus, MD is a Hematopathology Fellow at Beth Israel
Deaconess Medical Center in Boston, MA. She has a particular interest in
High-grade B-Cell lymphomas and the genetic alterations of these
lymphomas.