As a part of my Molecular Genetic Pathology fellowship, we experience a clinical component to training in addition to all of the laboratory training we receive. This last month, I rotated through Cancer Genetics, where genetic counselors discuss genetic testing with patients with a personal or family history of cancer. The counselors describe the process of genetic testing and help chose genetic tests to look at the patient’s risk for an inherited cancer syndrome.
Patients are looking forward to the certainty that will come from a genetic test, because it is the wave of the future and they think you can learn so many things from your genetics. The truth, however, can be much less clear. Up to 30% of people receive a Variant of Uncertain Significance (VUS) as their genetic test result. This rate increases as larger panels are test more genes.

A VUS represents a variation in a person’s gene that doesn’t have enough information to say that it is benign or pathogenic. This gray zone is very uncomfortable and confusing for patients and providers alike. There are several cases where someone acted on a VUS as if it were a pathogenic variant and ended up having radical interventions like a bilateral mastectomy.
We know that as scientific and medical knowledge increases, our ability to reclassify these variants improves. For laboratories, this means periodic reanalysis of previously reported variants. If this process is not properly set up, it can be very laborious and extensive. Furthermore, not only was a timeline for variant reanalysis unknown, but also the likelihood of variants becoming upgraded or downgraded had not been described.
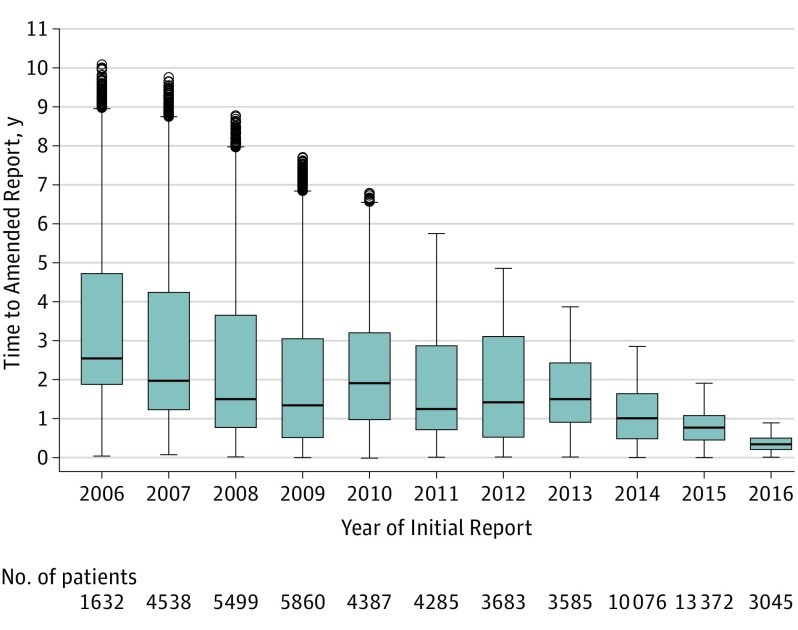
Two recent studies helped provide some answers to these questions. The first, published in JAMA, comes from the cancer genetic group I was working with, led by Dr. Theo Ross M.D. Ph.D., worked in conjunction with Myraid (Lab that first started testing the BRCA genes, and now tests many more) to determine how often variants were reclassified. Looking at 1.1 million individuals tested at Myriad, the average time to reclassification for a VUS was 1.2-1.9 years (Mersch J et al Jama 2018). Additionally, 90% of VUS were downgraded to benign/ likely benign representing 97% of patients with a VUS. This figure from the paper shows how the time to issuing a reclassification (amended report) has decreased (Figure 2).
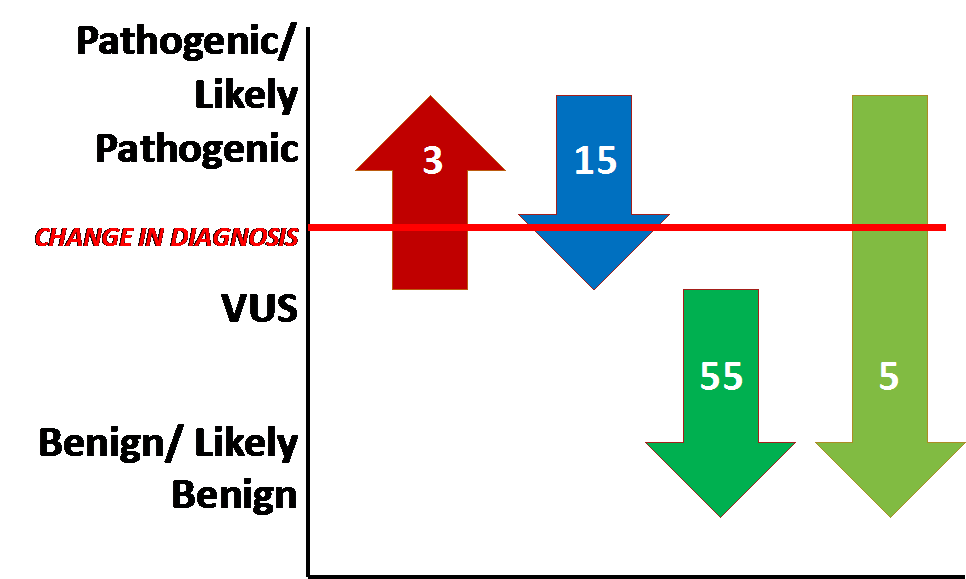
I worked on the second study, which looked at variant reclassification in childhood epilepsy genetic testing (SoRelle et al JAMA Peds 2019). The results, published in JAMA Pediatrics, also found most patients had a VUS reclassified to benign/likely benign. However, several clinically significant changes (reclassified to or from pathogenic/ likely pathogenic) occurred as well (Figure 3).
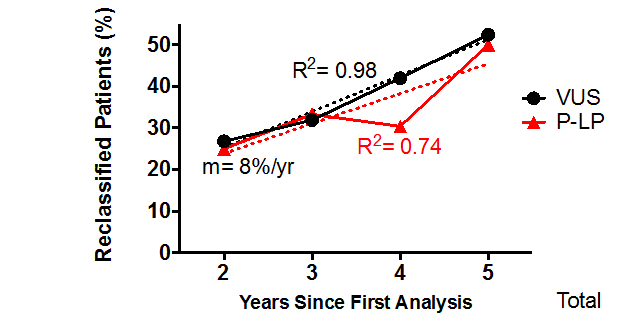
Furthermore, there was a linear relationship between the time the test was reported and the rate of variant reclassification (Figure 4). We found that 25% of patients with a VUS would experience a reclassification within 2 years.
Overall, the conclusions of the two studies are somewhat similar:
- Most patients with a VUS experience a downgrade reclassification to likely benign or benign.
- Variant reclassification should be performed at least every 2 years
- Rates of reclassification may differ by disease type. Investigation by a similar study design should be performed in other genetic diseases.
References
- Mersch J, Brown N, Pirzadeh-Miller S, Mundt E, Cox HC, Brown K, Aston M, Esterling L, Manley S, Ross T. Prevalence of variant reclassification following hereditary cancer genetic testing. JAMA. 2018;320:1266–1274.
- SoRelle JA, Thodeson DM, Arnold S, Gotway G, Park JY. Clinical Utility of Reinterpreting Previously Reported Genomic Epilepsy Test Results for Pediatric Patients. JAMA Pediatr. 2018 Nov 5:e182302.

-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and advancing quality in molecular diagnostics.
