Case History
An 83 year old man with rapidly growing squamous cell carcinoma of the left temple and scalp underwent workup prior to surgery which showed an elevated PTT and a slightly elevated PT. The patient denied a history of abnormal coagulation tests or excessive bleeding or bruising. He also noted that he had previous surgeries including dental procedures without excessive bleeding. In addition, he did not have a history of clot formation.
Lab Values

Differential Diagnosis
At this point, the differential diagnosis for a prolonged PTT included the presence of an inhibitor (specific factor inhibiter vs. non-specific lupus anticoagulant) vs. reduced levels/activity of intrinsic pathway factors that would prolong the PTT, but would not significantly affect clot formation. This would include factors XI and XII.
Additional Testing
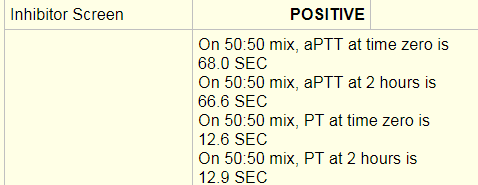
An inhibitor screen/mixing study was performed and was positive. An inhibitor screen is performed by mixing the patient’s plasma with pooled normal plasma and running a PT or PTT. If the PT/PTT corrects than the screen is negative. This means that a factor or factors were deficient in the patient’s plasma and were replaced with the pooled normal plasma resulting in a correction of the PT/PTT. In this case, a PTT at time 0 of 68 seconds and a PTT at 2 hours of 66 seconds was a failure to correct and indicated that an inhibitor was present, thus a positive result was entered.
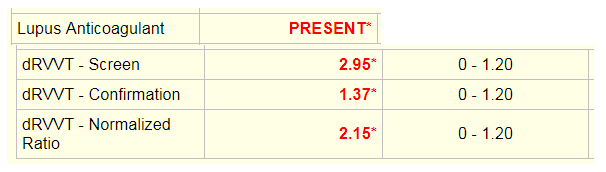
The dilute Russell’s viper venom time (dRVVT) was used to test for a lupus anticoagulant. The screening test is performed by adding Russell viper venom, which directly activates coagulation factor X in the presence of calcium and a phospholipid poor reagent to the patient’s plasma and calculating time to clot. The confirmation test is the same assay with added excess phospholipid. In the presence of phospholipid dependent antibodies, the time to clot will be shorter for the confirmation test. The screen and confirmation ratios are normalized ratios (NR) of the patient sample result in seconds divided by the mean of the normal range in seconds. If the screen is <1.20, the confirmation test will not be run. If the screen is greater than 1.20 as seen here, the confirmation test will be run. The end result is reported as a normalized ratio of the screening test over the confirmation test. If the NR is greater than 1.20, than a lupus anticoagulant is reported as present.
Specific factor assays are performed by mixing the patient’s plasma with substrate plasma that is severely deficient in the factor being measured. Factor deficient plasma would be expected to give a prolonged clotting time. When patient plasma is mixed with factor deficient plasma, the clotting time will shorten and the degree of correction is proportional to the factor level in the patient’s plasma. The clotting times for the patient sample are compared to a reference curve. The reference curve is made with dilutions of normal plasma (containing 100% factor) added to factor deficient substrate plasma. All tests are run with 3 dilutions at 25%, 50% and 100% and curves are checked for parallelism errors, which might indicate the presence of an inhibitor. For this patient, factor XI was initially resulted as 1%, which would indicate a factor deficiency.
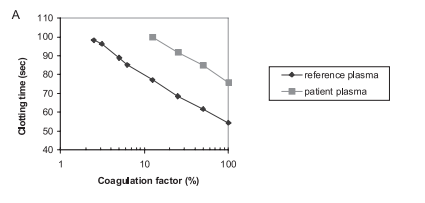
This is an example of a factor assay that shows parallelism. The reference plasma calibration curve and the patient plasma are parallel lines. 1
Analysis
From the results, it initially appeared that there was both a lupus anticoagulant and a factor XI deficiency. However, it would be odd for a patient with no reported coagulation abnormalities to suddenly have both a lupus anticoagulant and a factor XI deficiency. The raw data from the factor XI assay was obtained.
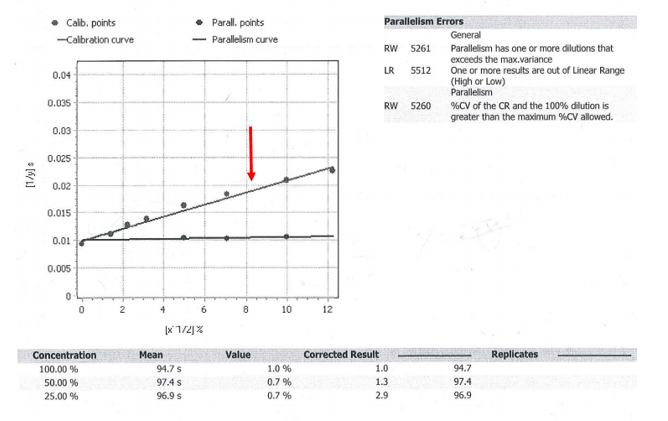
Upon review, the factor XI assay did show parallelism errors. Parallelism is tested by performing serial dilutions of a standard with known normal concentrations of factor and recording the time to clot. This line is shown with the red arrow. In contrast, the patient sample appears to be a flat line that is not parallel to the calibration curve. Parallelism errors were flagged because from the 50% to 25% dilution, the corrected results more than doubled. If there is a >20% change between dilutions, this indicates possible interference and additional dilutions should be run to dilute out the inhibitor. The 25% dilution had a corrected result of 2.9, which was greater than a 20% increase from the 50% dilution result of 1.3. Once more dilutions were performed; the Factor XI level was ultimately close to 100%.
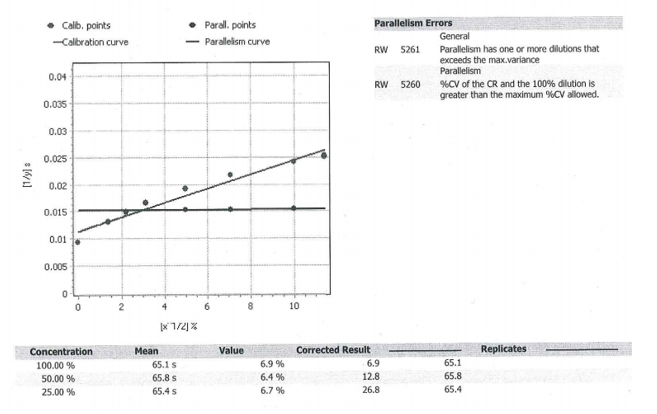
Additional factors were checked to see if they also increased with dilutions. This would add support to the theory of a non-specific inhibitor (lupus anticoagulant) that was affecting all of the factor levels, rather than a specific factor XI inhibitor or a concurrent factor XI deficiency. The curve from factor IX (below) showed a similar phenomenon. As the sample underwent additional dilutions, the corrected result increased significantly (from 12.8 at 50% to 26.8 at 25%). Ultimately, the factor level was close to 82%.
The curve from factor VIII also showed low results to begin with and ultimately normal levels with additional dilutions. Altogether, this supported the presence of a strong lupus anticoagulant that was non-specifically interfering with all of the factor levels and prolonging the PTT.
Discussion
A prolonged PTT can be caused by many factors. In a patient without a bleeding history, lupus anticoagulant and certain factor deficiencies are high on the differential. The most common specific factor inhibitors are to FVIII and FIX. These generally arise in hemophilia patients treated with factor concentrates. It is very rare for a patient to develop an inhibitor to factor XI or XII.
Factor XI acts in the intrinsic pathway of the clotting cascade and is important for hemostasis. Deficiency of factor XI is rare and mainly occurs in Ashkenazi Jews. Generally, it does not cause spontaneous bleeding; however excessive blood loss can occur during surgical procedures.
Lupus anticoagulants are directed against proteins that complex with phospholipids. Although they prolong the PTT, they are associated with an increase in thrombosis rather than bleeding. In addition to interfering with the PTT assay, lupus anticoagulants may interfere with individual factor assays and result in non-parallelism (patient curve is not parallel to calibration curve) as seen in this patient. With increasing dilutions, the lupus activity will be disproportionately neutralized and the coagulation factor activity will increase in a non-parallel manner. 1
In a letter to the editor by Ruinemans-Koerts et al., they performed a set of experiments to investigate whether lupus anticoagulants vs. individual FVIII and FIX inhibitors can cause non-parallelism in the one-stage factor assay. Non-parallelism was only detected using lupus sensitive reagents in plasma with high titers of lupus anticoagulants. The FVIII and FIX inhibitor containing samples both resulted in curves that were parallel to reference sample.
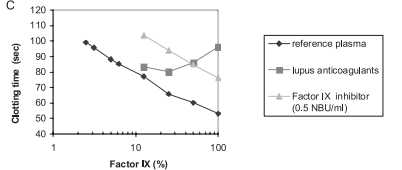
This curve shows that the factor IX inhibitor line is parallel to the reference plasma, while the lupus anticoagulant line is not. 1
Ultimately, this demonstrates the importance of running dilutions and being aware of parallelism errors when performing factor assays. This is especially important in patients with known or suspected lupus anticoagulants. In this case, the unlikely presence of a FXI deficiency with no previously reported coagulation testing abnormalities or bleeding history raised the suspicion of an inhibitor interfering with the factor assay. With a concurrent positive inhibitor screen and lupus anticoagulant test, as well as interference demonstrated with multiple factor assays, the best unified conclusion was a strong lupus anticoagulant. 1
References
- Ruinesman-Koerts, J., Peterse-Stienissen, I, and Verbruggen, B. ”Non-parallelism in the one-stage coagulation factor assay is a phenomenon of lupus anticoagulants and not of individual factor inhibitors. “ Letter. Thrombosis and Hemostasis, 2010, p.104.5.

–Chelsea Marcus, MD is a Hematopathology Fellow at Beth Israel Deaconess Medical Center in Boston, MA. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
