A 64 year old male presented with a one year history of loose
stools, lower abdominal crampy/gassy pain that improved with defection, and an
unclear history of melena. A colonoscopy revealed a circumferential, villous, carpet-like
lesion extending from 15 cm to the anal verge, with biopsies demonstrating
fragments of a villous adenoma. A follow-up CT scan was negative for metastatic
disease. The decision was then made to proceed with a low anterior resection
with hand-sewn colo-anal anastomosis and diverting loop ileostomy.
Diagnosis
Upon opening the rectum, a 13.8 cm long circumferential,
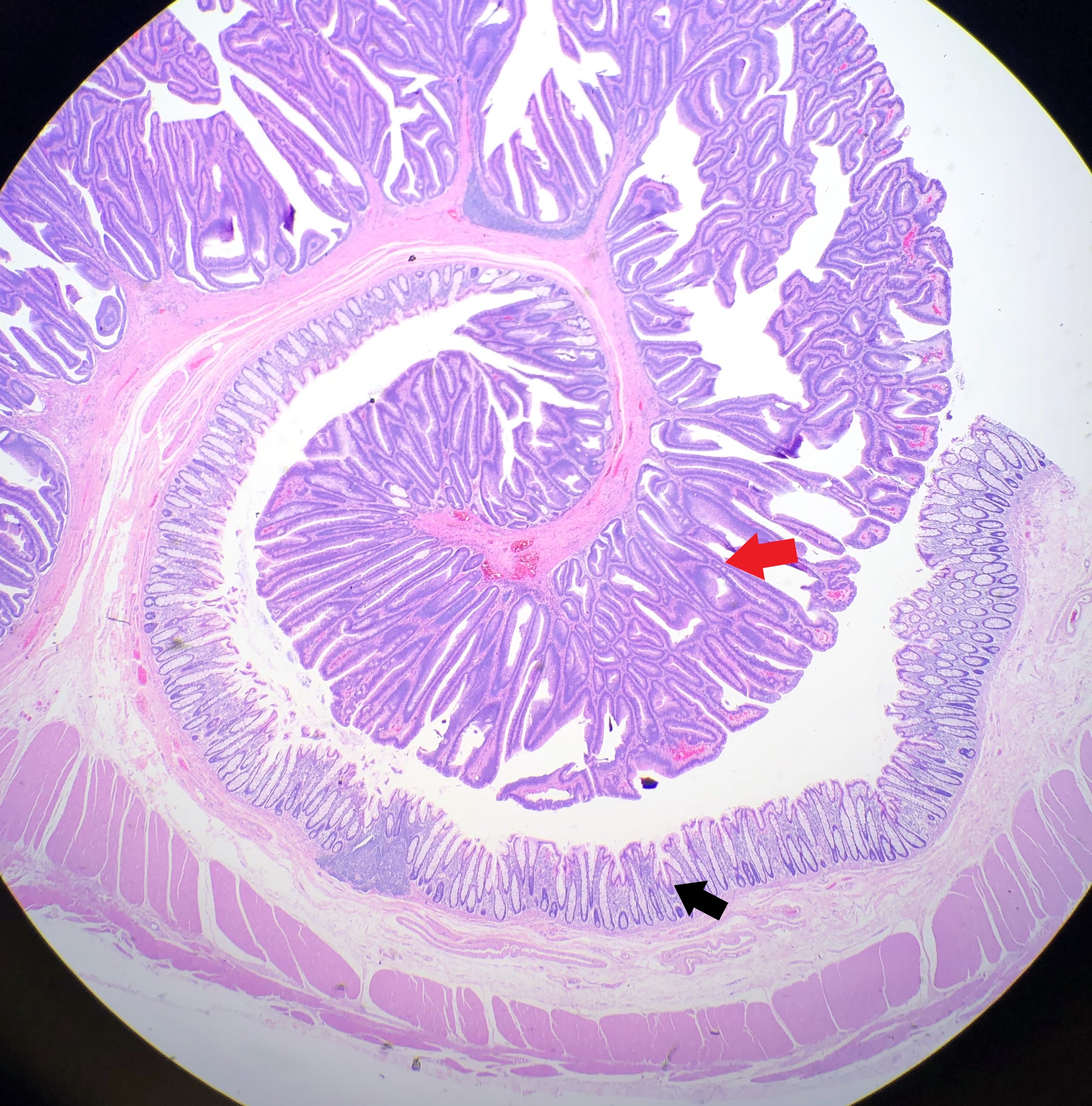
carpet-like lesion is identified, extending to the distal margin (Image 1). Sectioning demonstrated a lesion with
a maximum thickness of 1.0 cm, which grossly appears to be confined to
the mucosa. Due to the prior biopsy history of a villous adenoma, the entire
lesion was completely submitted. This required 116 blocks to be submitted,
which were then mapped out to show where each block would have been taken from
(Image 2). Although there were many foci of intramucosal carcinoma present, clear
cut submucosal invasion was not identified, and the specimen was signed out as
a villous adenoma (Image 3).
Image 1. Opened rectum demonstrating the 13.8 cm-long carpet-like lesion.Image 2. Mapping the lesion to show from where each block is taken.Image 3. Photomicrograph showing the transition from normal mucosa (black arrow) to villous adenomatous tissue (red arrow).
Discussion
Polyps are an abnormal tissue growth that is a common
occurrence within the colon, although they can also be found throughout the
small intestine, stomach and esophagus. Polyps can be further classified as
being neoplastic or non-neoplastic based on the histological pattern of the
cells. The most common types of neoplastic polyps found within the GI tract are
colonic adenomas, which are benign polyps that serve as precursors to the
majority of colorectal cancers. Nearly half of adults in the Western world will
develop adenomas by the age of 50, and there is no gender predilection. It is
because of this that it is recommended that all adults get a colonoscopy by the
age of 50 (even earlier when there is a family history of developing colorectal
cancer).
Most polyps are small, measuring 0.5 cm or less, but can grow
to be over 10 cm in size (as seen in this case). When a colonoscopy is
performed, these polyps can appear as sessile, meaning flat, or pedunculated,
meaning on a stalk. Due to the abnormal epithelial growth of the mucosa, the
surface of an adenoma can have a velvety appearance, resembling that of a
raspberry. Most patients will not demonstrate any symptoms from their polyps,
with the exception of occult bleeding and anemia which are associated with
larger polyps.
Dysplasia, which literally means “disordered growth”, occurs when the individual cells lose their uniformity and architecture, often resulting in cells with a hyperchromatic nuclei and a high nuclear to cytoplasmic ratio. The presence of dysplasia contained within the epithelium of a polyp is what classifies the polyp as an adenoma (Image 4). Based on their epithelial growth pattern, adenomas can be classified as either tubular adenomas or villous adenomas. Tubular adenomas tend to be smaller polyps, with a smoother surface and rounded glands on histologic examination. Villous adenomas, in contrast, tend to be larger polyps with long, slender villi noted on histology (Image 5). If an adenoma contains a mixture of tubular and villous elements, they are classified as tubulovillous adenomas. When a dysplastic cell is no longer contained within the epithelium, and instead breaches the basement membrane which separates the epithelium from the underlying tissue, it is termed invasive.
Image 4. Photomicrograph of the villous adenoma, demonstrating the dysplasia that is confined to the mucosa and not extending to the deeper tissue. Image 5. Photomicrograph of the long, slender villi that are commonly seen in villous adenomas.
What makes this case so interesting is that there is a direct
correlation between the size of an adenoma, and the risk of developing colorectal
cancer. This is not true with most other cancers, however, as size plays no
part in determining whether the tumor is cancerous or not. With colon polyps,
the larger the polyp, the greater the chance of developing invasive carcinoma
(i.e. cancer). This is why screening colonoscopies are so important. Studies
have shown that regular colonoscopies, combined with the removal of the polyps
found on the exam, reduce the incidence of colorectal cancer. Why this case is
so interesting is that you could assume based on the size of this polypoid
lesion, you would find some invasive component. However, after reviewing 116
blocks, not a single focus of invasion could be identified.
It should be stated that although
there is a correlation between an adenomas size and the risk of developing
cancer, the majority of adenomas will not progress to cancer, and in fact,
there are no tools currently available that help to determine why one patient’s
adenoma will progress to cancer, while another patient’s adenoma will not.
Turner JR. Polyps. In: Kumar V, Abbas AK, Fausto N, Aster JC. Robbins and Cotran Pathologic Basis of Disease, 8th edition. Philadelphia, PA: Elsevier, Inc; 2010: 815-820
-Cory Nash is a board certified Pathologists’ Assistant, specializing in surgical and gross pathology. He currently works as a Pathologists’ Assistant at the University of Chicago Medical Center. His job involves the macroscopic examination, dissection and tissue submission of surgical specimens, ranging from biopsies to multi-organ resections. Cory has a special interest in head and neck pathology, as well as bone and soft tissue pathology. Cory can be followed on twitter at @iplaywithorgans.
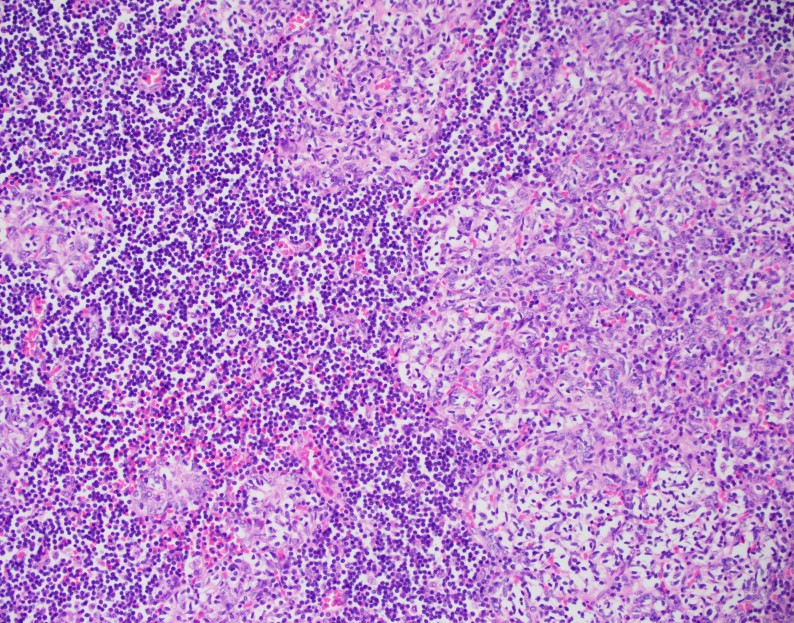
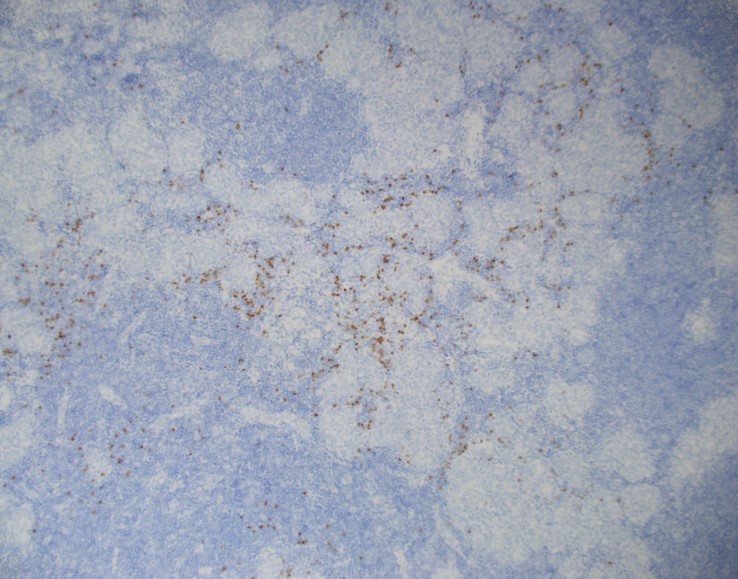
A 33 year old man of Japanese ethnicity presents with a 2 month history of a mass behind the right ear. Examination reveals a non-tender local with no other local or generalized adenopathy or hepatosplenomegaly. Laboratory investigations reveal an elevated ESR, serum IgE and peripheral blood eosinophilia. The lesion is excised.
Biopsy Findings
H&E stained sections
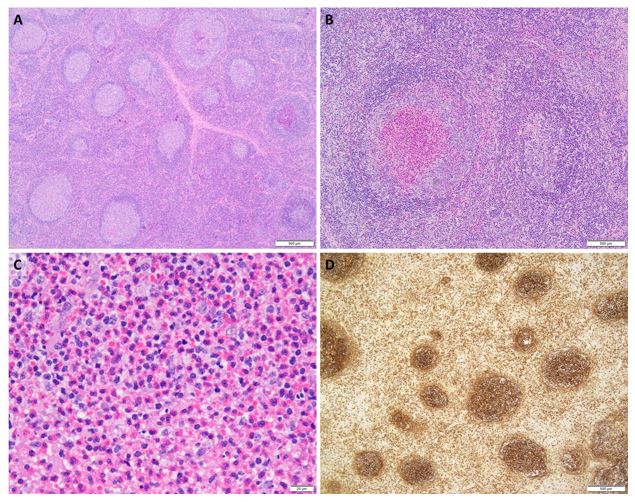
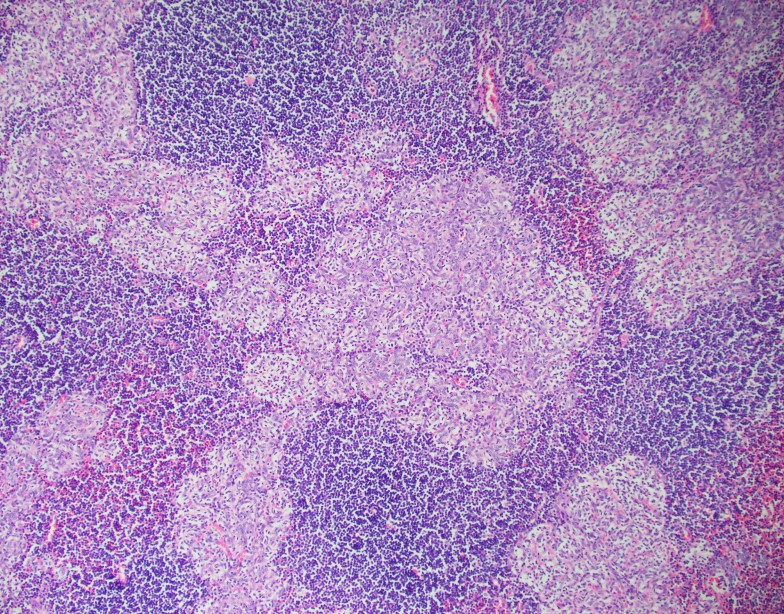
demonstrate a follicular hyperplasia. The germinal centers demonstrate polarity
and tingible body macrophages (A). Focally, follicular centers reveal
eosinophilic microabscesses (B, C). Immunohistochemical analysis with an IgE
stain reveals deposition in germinal centers (D). A diagnosis of Kimura disease
is rendered.
Discussion
Kimura
disease, also known as eosinophilic lymphoid follicular hyperplasia is a rare,
chronic inflammatory disorder of unknown etiology. While an infectious etiology
has been suggested, no pathogen has been identified to be causal, to date.
Historically, Kimura disease was considered to be the same as Angiolymphoid Hyperplasia
with Eosinophilia (ALHE); however, these entities are not the same.
Generally
occurring in Asian males, Kimura disease is most common in the 3rd decade of
life and in a head/neck site. It presents as painless, slow-growing adenopathy.
An association with nephrotic syndrome has been reported. Peripheral blood
eosinophilia, elevated ESR, and serum IgE are common findings. Histologically,
nodes reveal hyperplastic follicles with well-formed germinal centers and
mantle zones with deposition of IgE and eosinophilic microabscesses, as seen in
this case. Perinodal soft tissue may be involved. Necrosis may be present, but
is not extensive. Cytologically, FNA material may reveal polymorphous cell
population with many eosinophils.
Prognosis is
indolent; however, most cases recur after excision and radiation therapy
usually yields best outcome.
References:
Zhou P. et al. Kimura disease. Dermatol Online J. 2017 Oct 15;23(10).
García Carretero R et al. Eosinophilia and multiple lymphadenopathy: Kimura disease, a rare, but benign condition. BMJ Case Rep. 2016 Aug 31;2016. pii: bcr2015214211. doi: 10.1136/bcr-2015-214211.
Sun QF et al. Kimura disease: review of the literature. Intern Med J 2008;38:668–72.
–Kamran M. Mirza, MD, PhD, MLS(ASCP)CM is an Assistant Professor of Pathology and Medical Education at Loyola University Health System. A past top 5 honoree in ASCP’s Forty Under 40, Dr. Mirza was named to The Pathologist’s Power List of 2018. Follow him on twitter @kmirza
Last month, I discussed some really interesting topics at
the intersection between psychiatry and pathology—two
fields that aren’t exactly the closest; more so “diverged” in the hospital
milieu as if in a poem by Robert Frost. This month I’d like to bring the
conversation back to a topic I’ve addressed before: improving multidisciplinary
medicine and creating a Just Culture in medicine.
Not exactly culture with a swab or agar dish, a Just Culture
is an all-encompassing term for system-based thinking and process improvement
not at the expense of individuals. In a post I made last
July, the topic of high reliability organizations (or HROs) is one
that addresses communication and accountability in high stakes
environments—like healthcare!
Just Culture isn’t a stranger to lab medicine. The American
Society of Clinical Laboratory Science (ASCLS) published a position paper in
2015 utilizing this trending healthcare buzzword. On the subject of patient
safety, ASCLS believes “Medical Laboratory Professionals must adopt a ‘fair and
just culture’ philosophy, recognizing that humans make errors, and
understanding the science of safety and error prevention.” (Source: ASCLS 2015,
https://www.ascls.org/position-papers/185-patient-safety-clinical-laboratory-science)
We all know how we maintain patient safety in the lab, right? We do that
through quality control, QA measures, competencies (both internal and from
accrediting bodies like CAP), and continuing education. Raise your hand if your
lab is getting inspected, just finished getting inspected, will be inspected
soon, or if you’ve recently done competency/proficiency testing yourself, CE
courses for credentialing, or are reading this blog right now! We’re all
“continuing” our education in health care ad
infinitum because that’s how it works—we keep learning, adjusting, and
ensuring best practices concurrent with the latest knowledge. And, instead of
punishing lab professionals when we make errors, we try to be transparent so
that each error is a learning opportunity moving forward.
Image 1. I’d panic too if my lab was being inspected by 007. What, you wouldn’t?
I’m currently in my OB/GYN rotation at Bronx-Care and during
the most recent Grand Rounds we had someone talk about “Just Culture”—a sort of
continuation on the themes of the same lecture series that inspired my article
on HROs. Essentially, the theme is that disciplining employees for violating
rules or causing error(s) in their work is less effective than counseling,
educating, and system-oriented and best-practice-informed care. In this talk,
we watched a short video (embedded below) which walked us through approaching
faults or errors in medicine in a way that empowers and educates. A story from
MedStar Health, a Maryland-based health system, demonstrates how systems-based
thinking can be the best way to solve problems in healthcare.
Video 1. “Annie’s Story” has become a widespread example of Just Culture for nearly twenty years. Being serious about high reliability and just culture means adopting a system’s approach to analyzing near misses and harm events—shame and discipline are becoming antiques. Learn more about Quality and Patient Safety (http://ow.ly/M1aZk) and Human Factors Engineering in Healthcare (http://MedicalHumanFactors.net)
Annie, a nurse in the MedStar Hospital system, is the
spotlight story in this video. She came across an error message on a glucometer
after checking someone who was acutely symptomatic. She double checked it and
made clinical decisions, with her providing team, to give insulin. This sent
the patient into a hypoglycemic event which required ICU support. In the story,
she was actually suspended and reprimanded for her “neglect”—other nurses made
the same error just days later. This prompted some action, inciting nursing
managers and other administrators to investigate further, ultimately involving
the biomedical engineers from the company to weigh in on this systemic fault in
glucose POCT. Annie returned to work, and the problem was recognized as not
user-error, but system error; she went on to talk about how she felt unsure of
her clinical competency after being reprimanded. Imagine if you accidentally
reported the presence of blast cells in a manual differential in a pediatric
CBC while you were alone on a night shift only to find out from the manager on
days that you made a pretty big mistake with clinical implications. Then
imagine you were suspended for a few weeks instead of simply asked to explain
and identify opportunities to increase your knowledge. Pretty harsh, right? I’m
glad the MLS who did that didn’t lose his job and only had to do a few more
competency trainings…yep.
Image 2 (a, b). Take a look at that glucometer. Would you have caught the error? Did you catch the “LO” value in the background vs. the out-of-range foreground prompt? Or was the screen prompt as distracting for you as it was for Annie? Who was responsible for this error: nurse, lab, or engineer?
Anyone else notice a stark absence of professional
laboratory input in the video? I assume many of you sharp-sighted lab
automation veterans didn’t miss the glaring “LO” behind the dialogue box on the
glucometer. And, to me, that begs the question: was there any lab input on this
instrument, its training, or its users? Nurse Annie made a mistake—but she’s
not alone, according
to a Joint Commission study from November last year, close to 11% of
users make mistakes when prompted with error messages compared to 0% of users
misinterpreting normal values on screens of a particular model of glucometer.
And that’s just one type of instrument. Imagine 1 in 10 nurses, medical
assistants, or patients misinterpreting their glucose readings. (Source: The
Joint Commission Journal on Quality and Patient Safety 2018; 44:683–694
Reducing Treatment Errors Through Point-of-Care Glucometer Configuration) This
should also be a good opportunity to remind us all of CLIA subpart
M, the law that outlines who can accredit, use, and report
point-of-care results. Herein lies another problem, stated well by the American
Association for Clinical Chemistry (AACC) in 2016, “… another criteria for
defining POCT—and possibly the most satisfactory definition from a regulatory
perspective—is who performs the test. If laboratory personnel perform a test,
then this test typically falls under the laboratory license, certificate, and
accreditation, even if it is performed outside of the physical laboratory
space, and regardless of whether the test is waived or nonwaived. On the other
hand, waived or nonwaived laboratory tests performed by non-laboratory
personnel are nearly always subject to a different set of regulatory and
accreditation standards, and these can neatly be grouped under the POCT
umbrella,” and that can mean trouble when we’re all trying to be on the same
clinical page.
In previous posts, I’ve mentioned
the excellent knowledge contained within the Lab Management University (LMU)
program. One of the modules I went through discussed this topic
exactly: Empowerment as a Function of
Leadership and Peak Performance. In short, if we want to be good leaders in
the lab, we have to set expectations for positive patient outcomes, including
safety. Good leadership should empower their staff with education, support, and
resources. Poor management can create toxic environments with staff that can be
prone to mistakes. If we can be dynamic leaders, who adapt to ever-improving
best practices and respond with understanding and compassion to mistakes, then
our colleagues become just as reliable as your favorite analyzer during that
CAP inspection I mentioned.
Image 3. LMU class module for promoting Just Culture and inciting positive behavior in your department.
I often get clinician input about how the processes between
the bedside and the lab can be improved. Often, they include comments about the
need to share relevant clinical data for improving diagnostic reporting or
improving a process between specimen collection and processing. But what often
gets left out is the human element: the scientist behind the microscope, the
manager behind the protocol, and the pathologist behind the official sign out
report. Let’s continue to incorporate all of the feedback our colleagues
provide while maintaining a safe and empowered culture for ourselves, our
staff, and our patients.
What do you think? How does your lab, hospital, clinic, etc.
address POCT safety or patient safety at large? Do you operate within a Just
Culture? Share and comment!
Thanks and see you next time!
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student actively involved in public health and laboratory medicine, conducting clinicals at Bronx-Care Hospital Center in New York City.
60 year old man with recurrent bronchitis and extensive
smoking history underwent CT scan. The CT scan showed an incidental finding of
a 2.2 x 1.4 cm anterior mediastinal mass.
The tissue shows nodules of epithelial cells in a
lymphocyte-rich background. The epithelial cells have round to somewhat spindle
shaped nuclei, vesicular chromatin and small mostly inconspicuous nucleoli.
There is no high grade cytologic atypia, mitotic figures or necrosis seen. The
nodules contain very few interspersed lymphocytes, but are surrounded by
abundant lymphocytes which are small and mature appearing. A cytokeratin
cocktail highlights the epithelial nodules and shows an absence of epithelial
cells in the lymphocyte-rich areas. CD20 highlights stromal B-lymphocytes
around the epithelial nodules which are arranged in follicles. CD3 highlights
stromal T-lymphocytes, which surround the B-cell follicles and the epithelial
nodules. TdT highlights only a very small subset of immature T-cells which are
found scattered around the rim of the epithelial cell nodules. Overall, the
findings are consistent with a micronodular thymoma with lymphoid stroma.
Discussion
The differential diagnosis for an anterior mediastinal mass
includes thymoma, lymphoma, germ cell tumors, neurogenic tumors and benign
cysts among other less common entities. Patients usually present with cough,
chest pain, fever/chills or dyspnea and localizing symptoms are generally
secondary to local tumor invasion. Typically, CT scans are the best modality to
evaluate the mediastinum. Thymomas are the most common primary neoplasm of the
anterior mediastinum, but are less than 1% of all adult malignancies. Patients
are generally over 40 years old and between 30-50% of patients with a thymoma
have myasthenia gravis, which occurs more frequently in women.1
The WHO has classified thymomas into 5 categories based on
the morphology of the neoplastic epithelial cells along with the lymphocyte to
epithelial cell ratio. Type A thymomas are composed of bland spindle/oval tumor
cells with few or no admixed immature lymphocytes. Type B1 thymoma resembles
normal thymus and has scattered epithelial cells in a dense background of
immature T-cells. Type B2 thymoma is composed of epithelial cells in small
clusters with a lymphocyte-rich background. Type B3 thymoma is primarily
composed of mild to moderately atypical epithelial tumor cells in a solid
growth pattern with few intermingled immature T-cells. Type AB thymomas are
composed of lymphocyte-poor spindle cell (Type A) components as well as
lymphocyte-rich (Type B) components.2
Micronodular thymoma with lymphoid stroma (MTWLS) is a rare
type of thymoma and accounts for only 1% of all cases. Patients tend to be
asymptomatic and the finding is usually incidental. The tumor tends to be well
circumscribed and encapsulated with a tan cut surface. The histopathology is
characterized by solid nests or nodules of epithelial tumor cells in a
background of abundant lymphoid stroma. The tumor cells are bland spindle or
oval cells without significant atypia or mitotic activity. The epithelial tumor
cells are positive for pancytokeratins. The lymphoid stroma typically lacks
keratin positive cells and consists of predominantly CD20 positive mature
B-cells in follicles with admixed CD3 positive and TdT negative mature T-cells.
There is typically a population of rare TdT positive immature T-cells that
surrounds the epithelial nodules, as seen in this case. 2
Due to the rarity of MTWLS with only 74 cases reported since
the first case described in 1999, there is limited data on its pathophysiology
and prognosis. However, most cases are diagnosed as stage I/II disease
according to the Masaoka-Koga staging criteria, involving only micro or
macroscopic invasion into thymic or surrounding fatty tissue without invasion
into neighboring organs. Patients tend
to have a very favorable prognosis with most patients alive without recurrence or
metastasis many years after diagnosis.3
References
Juanpere S, Cañete N, Ortuño P, Martínez S,
Sanchez G, Bernado L. A diagnostic approach to the mediastinal masses. Insights
Imaging. 2012;4(1):29-52.
Travis WD, Brambilla E, Burke AP, et al. WHO
Classification of Tumours of the Lung, Pleura, Thymus and Heart (Revised 4th
edition). IARC: Lyon 2015.
Qu L, Xiong Y, Yao Q, Zhang B, Li T.
Micronodular thymoma with lymphoid stroma: Two cases, one in a multilocular
thymic cyst, and literature review. Thorac Cancer.
2017;8(6):734-740.
–Chelsea Marcus, MD is a Hematopathology Fellow at Beth Israel Deaconess Medical Center in Boston, MA. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
Authors: Dr. Maryam Zenali (Department of Pathology), Dr. Eric Ganguly (Department of Gastroenterology), and Dr. Christopher J. Anker (Division of Radiation Oncology), University of Vermont Medical Center
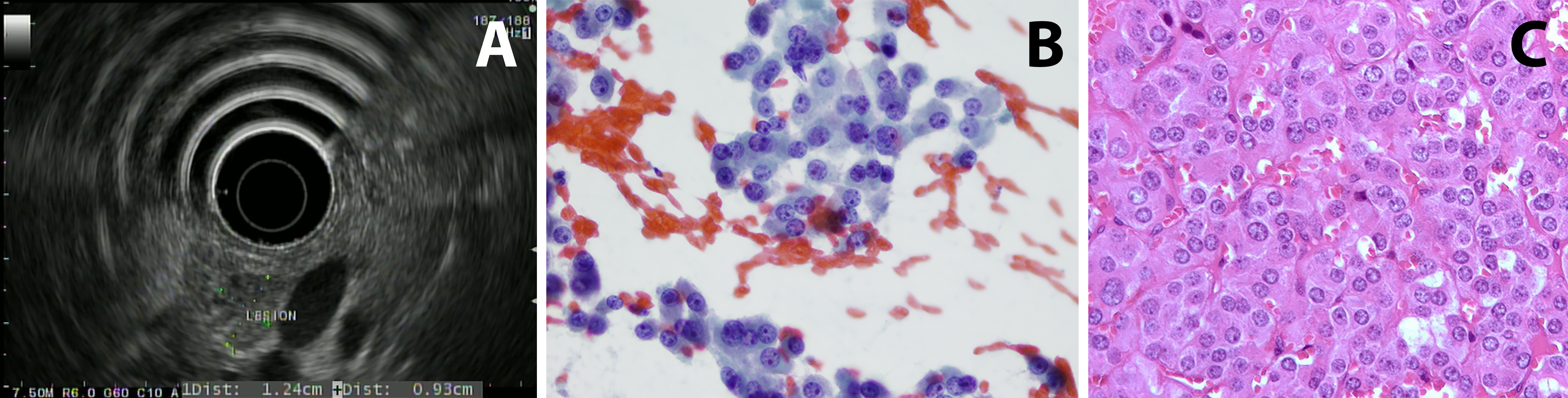
Case 1: Patient 1 is a 75 year old man with a history of gastroesophageal reflux disease (treated with a proton-pump inhibitor) who had an episode of diaphoresis and altered mental status at 3:30 am. He was found to have a glucose of 20 when rescue arrived. He was brought to the ED and symptoms resolved after glucose administration. Work-up showed fasting C-peptide of 3.5 (normal range: 1.1-4.4 ng/mL) ruling out excess insulin use; proinsulin was elevated at 300 (normal range: 3-20 pmol/L). Serum chromogranin A was noted to be mildly elevated. He had a CT scan of the abdomen that did not show any abnormal enhancement or concerning lesion. Endoscopic ultrasound (EUS) imaging demonstrated a slightly hypoechoic mass in the pancreatic head with a hyperechoic halo margin. The mass was adjacent to, although not invading, the portal vein. The remainder of the pancreatic head had a normal echotexture (figure 1A). Fine needle aspiration and biopsy of the lesion were performed; microscopic images are provided (figures 1B and 1C).
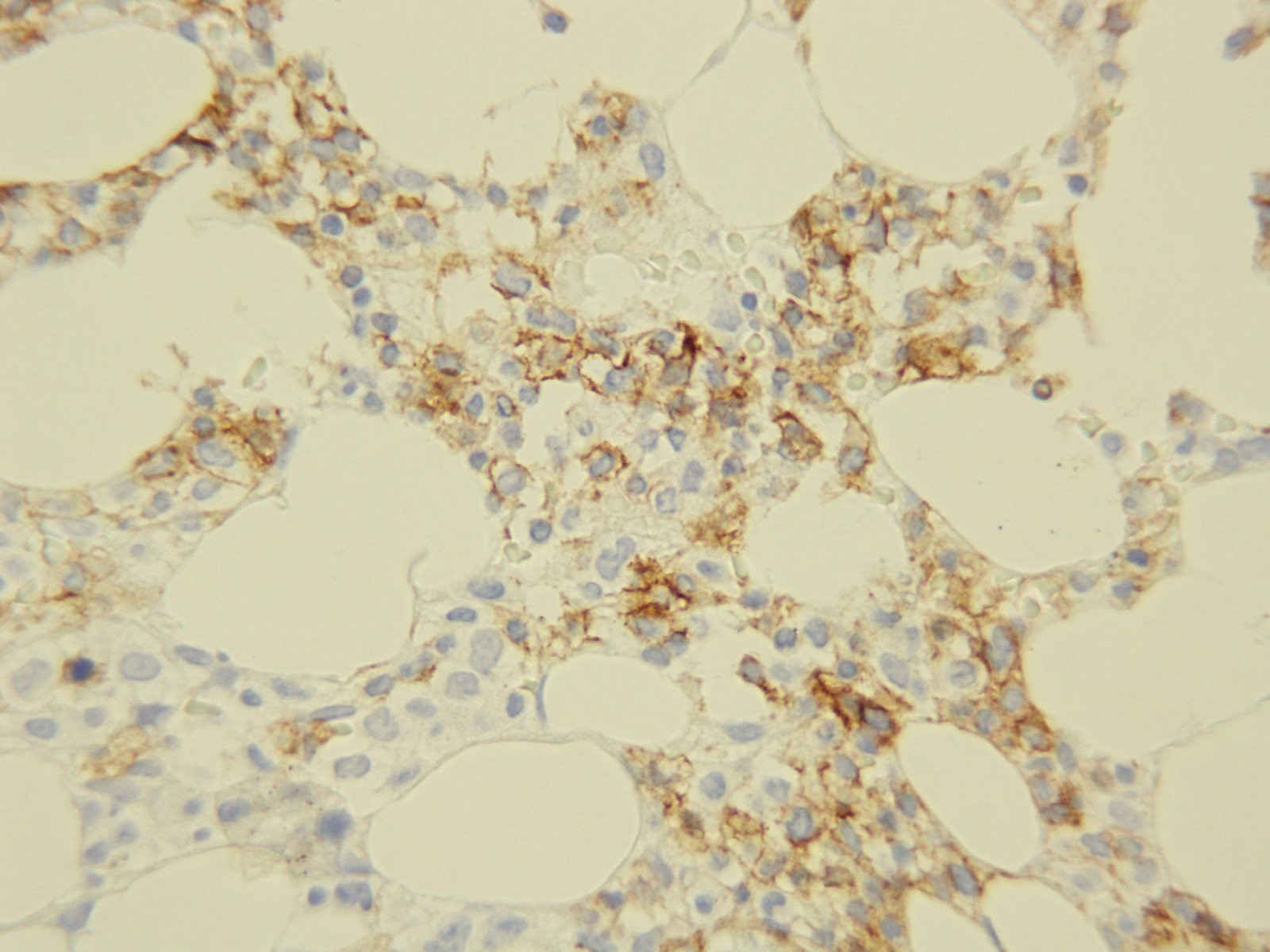
Histology: A relatively monotonous, well-differentiated tumor with regular, round salt-and-pepper chromatin and eosinophilic cytoplasm. There were only rare apoptotic cells and no mitosis. 1% of tumor nuclei were immunoreactive with MIB-1 (Ki67 K2 Leica). Tumors cells were diffusely and strongly positive for synaptophysin (27G12, Leica), chromogranin (LK2H10, Ventana) and keratin (AE1-AE3, Biocare) but negative for makers such as TTF1, CK7, Beta-catenin and GATA-3.
This month
our study results were published in a special edition of Clinical Chemistry describing how laboratory values in transgender
men and women when taking hormone therapy. While retrospective, we hope that
this information will help improve transgender medicine.
There were
many interesting results found in the study and I hope to describe bits of them
in greater detail each month.
We
wondered what we might find if we took a broad, unbiased approach comparing all
laboratory parameters commonly measured by physicians. Just because there are
no sex-specific differences in analytes, changes could still occur secondary to
exogenous hormone use.
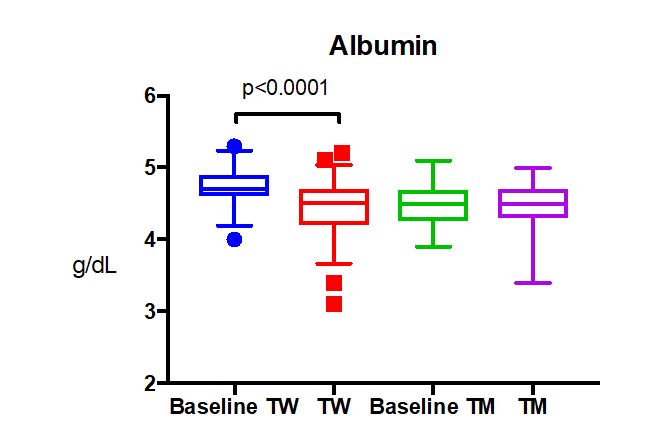
Albumin, which is the principle protein in our blood, was found to be decreased in transgender women after taking at least 6 months of estradiol therapy (p<0.0001)1. This was unexpected, because one reference range for albumin is used for cisgender males and females.
Frequently,
changes in lab values move in opposite directions for transgender patients
taking estradiol vs. testosterone (ex. hemoglobin goes up with testosterone and
down with estradiol). We wondered if a similar opposite change might occur in
albumin for transgender men taking testosterone. However, there was no change
in albumin levels from baseline for transgender men.
The cause
of decreased albumin was not readily available, but several factors could be
influential. Albumin levels reflect the long term nutritional status of a
patient as it has a long half life for turnover (t½= 3-4 weeks). Thus, the
change in albumin could reflect a dietary change in transgender women. However,
in the chart review there was nothing to suggest a substantial change in diet.
While several of the patients would go on diets and lose weight, the weight
loss was (unfortunately) often short lived (< 1 year). Looking towards a
more objective reflection of dietary changes, the body mass index was nearly
the same for transgender women pre-hormone therapy vs. while on hormone therapy
(BMI: 27 vs 29, p>0.05).
Some
studies have shown an increased prevalence of disordered eating behaviors among
transgender individuals2, which could affect overall nutritional
status as reflected in albumin. However, this should be controlled for by the
control group, which is just transgender patients who haven’t taken hormones
previously.
Another
consideration is that body composition changes in transgender patients such
that transgender women lose lean mass and have an increase in body fat percent3.
Although this could affect the metabolic profile (which it didn’t in our study),
changes in fat percent don’t explain altered albumin levels.
Albumin
levels are also low in patients with chronic liver disease, but this would be
inconsistent with the patients’ medical history or other lab results. Frank nephrotic
syndrome is unlikely as there were no reports of this disease within our population,
but we did not have data on urinalysis, so we can’t say for certain.
One study
did show that males (TW baseline equivalent) have higher albumin than females
at younger ages (<60 y.o.) that equilibrates in later decades4.
This sex-specific difference shows how estradiol decreases albumin to cisgender
female levels. However, the reverse effect (increased albumin) does not occur
with testosterone in transgender males. This demonstrates how sex-specific
reference intervals cannot be simply reversed for transgender patients.
In a
normal set of outpatients in the UK, oral contraception use (which includes
estradiol) in women decreased their albumin levels by 0.2 g/dL, which is a
smaller magnitude than found in our study, but supports a hormonal basis for
sex-specific differences in albumin4.
Although
the decrease in albumin for our cohort was not clinically significant (did not
pass lower limit of normal albumin reference interval), it would be important
to monitor albumin levels in older or elderly transgender females on hormone
therapy. Elderly patients are at increased risk of hypoalbuminemia, especially
when hospitalized5.
Summary:
Albumin
is decreased in transgender women taking estradiol therapy.
Albumin
levels do not fall below normal ranges.
This
could be more important in older or elderly transgender patients who are
already at risk of hypoalbuminemia.
References
SoRelle
JA, Jiao R, Gao E et al. Impact of Hormone Therapy on Laboratory Values in
Transgender Patients. Clin Chem.
2019; 65(1): 170-179.
Diemer EW, Grant JD, Munn-Chernoff
MA et al. Gender Identity, Sexual
Orientation, and Eating-Related Pathology in a National Sample of College
Students. J Adolesc Health. 2015;
57(2):144-9.
Auer
MK, Cecil A, Roepke Y et al. 12-months metabolic changes among gender dysphoric
individuals under cross-sex hormone treatment: a targeted metabolomics study. Sci Rep. 2016; 6: 37005.
Weaving
G, Batstone GF, Jones RG. Age and sex variation in serum
albumin concentration: an observational study. Annals of Clinical Biochemistry 2016, Vol. 53(1) 106–111.
Cabrerizo
S, Cuadras D, Gomez-Busto F et al. Serum albumin and health in older people:
Review and meta analysis. Maturitas.
2015; 81(1):17-27.
-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and advancing quality in molecular diagnostics.
A 65 year old Caucasian male presents with a skin lesion on his right shoulder. Physical examination reveals a 3 .0 cm × 1.5 cm hyperpigmented plaque with mild hyperkeratosis on his right shoulder and multiple scattered erythematous macules and plaques on the trunk and back Skin biopsy reveals involvement by Blastic Plasmacytoid Dendritic Cell Neoplasm (BPDCN). PET scan reveals no extracutaneous involvement.
The patient undergoes CHOP
chemotherapy followed by autologous hematopoietic stem cell transplantation. He is subsequently treated
systemically with lanolidomide,
venetoclax, and idelalisib due to relapses of disease.
The patient returns to
clinic three years later for follow-up. While his original cutaneous lesions are
completely resolved, new lesions are noted on his back (representative lesion,
Image 1). Hematologic evaluation is remarkable for pancytopenia with hemoglobin
8.7gm/dL, white blood cells 1.4 K/uL, and platelets 39 K/uL. A biopsy of the
bone marrow is performed.
Image 1. Skin lesion on back.
Biopsy Findings
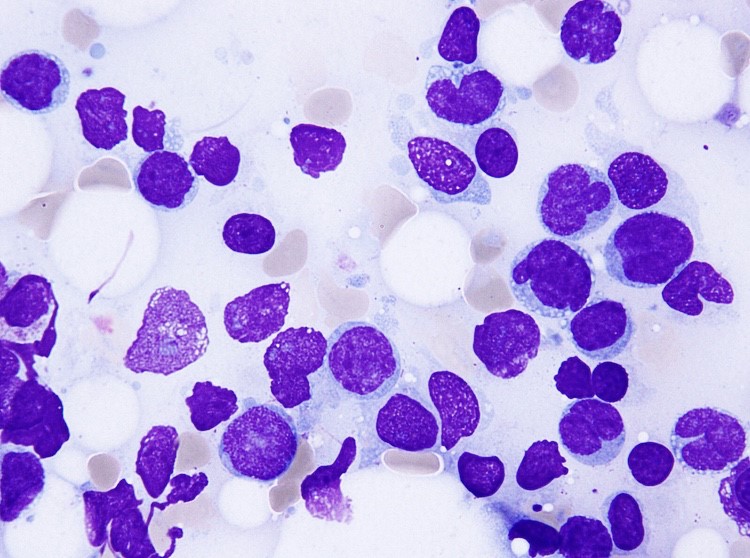
Core biopsyCD56Aspirate
H&E stained sections
demonstrate a normocellular bone marrow with diminished trilineage
hematopoiesis and sheets of amphophilic, blastoid cells with irregular borders
occupying most of the marrow cells. Immunohistochemistry demonstrates a cellular population with CD56. The aspirate smears show similar findings with numerous
clustered blastoid cells (92%) with a monocytoid appearance, often with
basophilic vacuolated cytoplasm. There is also a decrease in myeloid and
erythroid precursors.
Flow cytometric analysis
performed on the bone marrow aspirate reveals a dim CD45 population with
expression of CD4, CD56, partial CD7, dim and partial CD5, and CD38. The same population
lacks expression of immaturity markers such as CD34, MPO, and TdT. The
morphologic and phenotypic findings found in the marrow specimen are diagnostic
of extensive involvement of the marrow by BPDCN.
Discussion
BPDCN is a
rare and highly aggressive malignancy derived
from precursors of
plasmacytoid dendritic cells. Its nomenclature has constantly
changed over years as the understanding of this entity has been improved. It
has been variously known as blastic natural killer cell lymphoma/leukemia, agranular
CD4+ natural killer cell leukemia, and CD4+CD56+haematodermic neoplasm. It is currently classified under acute
myeloid leukemia and related precursor neoplasms in the most recent WHO
classification of tumours of haematopoietic and lymphoid organs.
Limited data exist regarding the incidence of
BPDCN; however, it is estimated to account for 0.7% of primary cutaneous skin
lymphomas and 0.44% of all hematological malignancies. This hematodermic malignancy predominantly
affects elderly male patients with mean age ranging from 60 to 70; however, a
few cases have also been reported in childhood and infancy. As demonstrated in
our case, the patients typically present with multiple
violaceous skin lesions, which may be associate with erythema,
hyperpigmentation, purpura, or ulceration. Extracutaneous involvement is
reported to occur in the bone marrow, peripheral blood, and lymph nodes.
Diagnosis of BPDCN relies on
histological and immunophenotypic findings. Histologically, BPDCN may show a monomorphic
infiltrate of medium-sized immature blastoid cells with round nuclei, finely
dispersed chromatin, and cytoplasmic vacuoles. They typically display immunophenotypic
expression of markers CD4, CD56, CD123, and T-cell leukemia/lymphoma 1 (TCL1) without
any lineage-specific markers of T cells or B cells. Chromosomal
abnormalities involving 5q, 12p,13q, 6q, 15q, and 9p have been reported. The differential diagnosis entails, but is not limited to, mature T-cell lymphoma, nasal-type NK/T-cell lymphoma,
myeloid sarcoma/acute myeloid leukemia and T-cell lymphoblastic lymphoma/leukemia
The clinical course of BPDCN is aggressive, with
a median survival of 9 to 16 months. The patients with disease limited to the
skin may have a better prognosis, while advanced age and advanced clinical
stage are indicators of poor prognosis. There
is currently no consensus on optimal management and treatment because of low
incidence of BPDCN; however, most patients are treated with regimens used for other hematopoietic
malignancies (i.e. CHOP and hyperCVAD) followed by allogeneic stem cell
transplantation for eligible patients. They often respond well to chemotherapy
with complete resolution of skin lesions; however, relapse of disease can occur
due to resistance to chemotherapeutic agents, which may have happened in our
case.
References
Lim
MS, Lemmert K, Enjeti A. Blastic plasmacytoid dendritic cell neoplasm (BPDCN):
a rare entity. BMJ Case Rep.
2016;2016:bcr2015214093.
Grushchak
S, Joy C, Gray A, Opel D, Speiser J, Reserva, Tung R, Smith SE. Novel treatment
of blastic plasmactoid dendritic cell neoplasm: a case report. Medicine (Baltimore). 2017
Dec;96(51):e9452.
Dhariwal
S, Gupta M. A case of blastic plasmacytoid dendritic cell neoplasm with unusual
presentation. Turk J Haematol. 2018
Jul 24. doi: 10.4274/th.2018.0181.
Shi
Y, Wang E. Blastic plasmacytoid dendritic cell neoplasm: a clinicopathologic
review. Arch Pathol Lab Med. 2014
Apr;138(4):564-9.
Bulbul
H, Ozsan N, Hekimgil M, Saydam G, Tobu M. Report on three patients with blastic
plasmactoid dendritic cell neoplasm. Turk
J Haematol. 2018 Sep;35(3):211-212.
Kerr
D 2nd, Sokol L. The advances in therapy of blastic plasmacytoid
dendritic cell neoplasm. Expert Opin
Investig Drugs. 2018 Sep;27(9):733-739.
Pagano
L, Valentini CG, Pulsoi A, Fisogni S, Carluccio P, Mannelli F, et al. Blastic
plasmactoid dendritic cell neoplasm with leukemic presentation: an Italian
multicenter study. Haematologic. 2013
Feb;98(2):239-246.
-Jasmine Saleh, MD MPH is a pathology resident at Loyola University Medical Center with an interest in dermatopathology and hematopathology. Follow Dr. Saleh on Twitter @JasmineSaleh.
-Kamran M. Mirza, MD PhD is an Assistant Professor of Pathology and Medical Director of Molecular Pathology at Loyola University Medical Center. He was a top 5 honoree in ASCP’s Forty Under 40 2017. Follow Dr. Mirza on twitter @kmirza.
66 year old man with a past medical history of Sjogren
syndrome, hypertension and hypothyroidism presented to an outside hospital with
abdominal pain and diarrhea. CT imaging showed extensive lymphadenopathy,
splenomegaly, mesenteric thickening and ureteral dilatation, all highly
concerning for lymphoma or other malignancy. A needle core biopsy of “mesenteric
mass” showed reactive lymphoplasmacytic infiltrate in a sclerotic background. A
second needle core biopsy of a retroperitoneal lymph node was performed which showed
reactive features and numerous plasma cells. An excisional biopsy of an
inguinal lymph node was ultimately performed due to worsening lymphadenopathy
with increased PET FDG avidity.
Excisional Biopsy
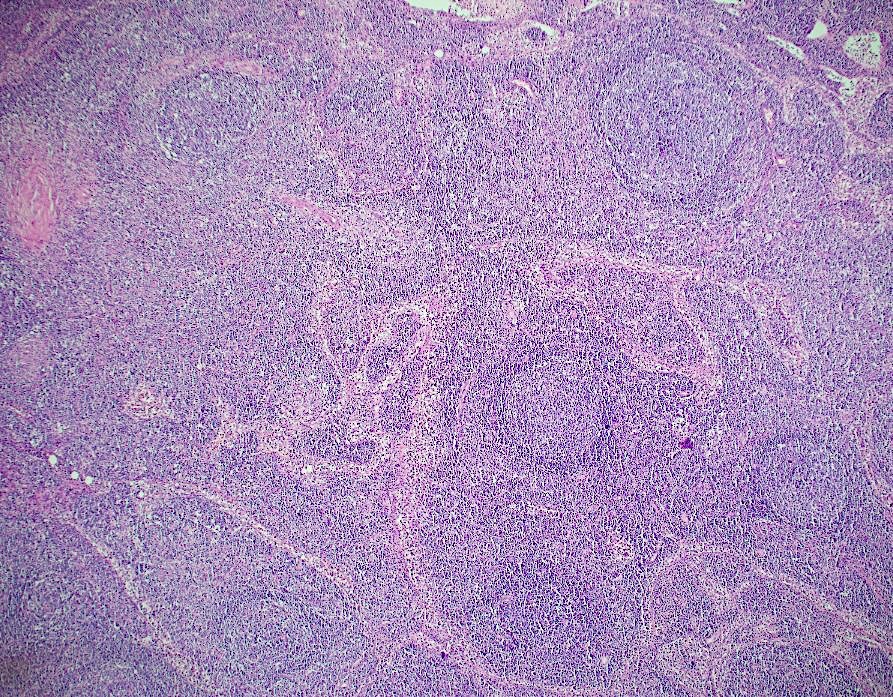
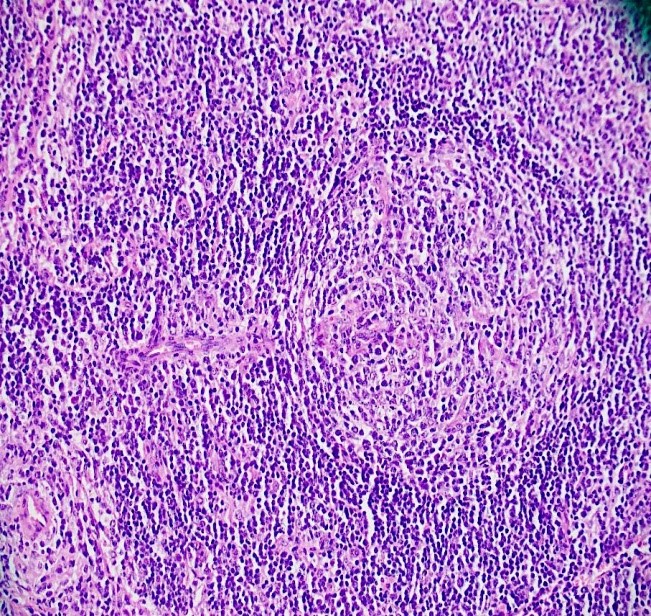
H&E 10x H&E 20xH&E 20xH&E 40xIgGIgG4
Diagnosis
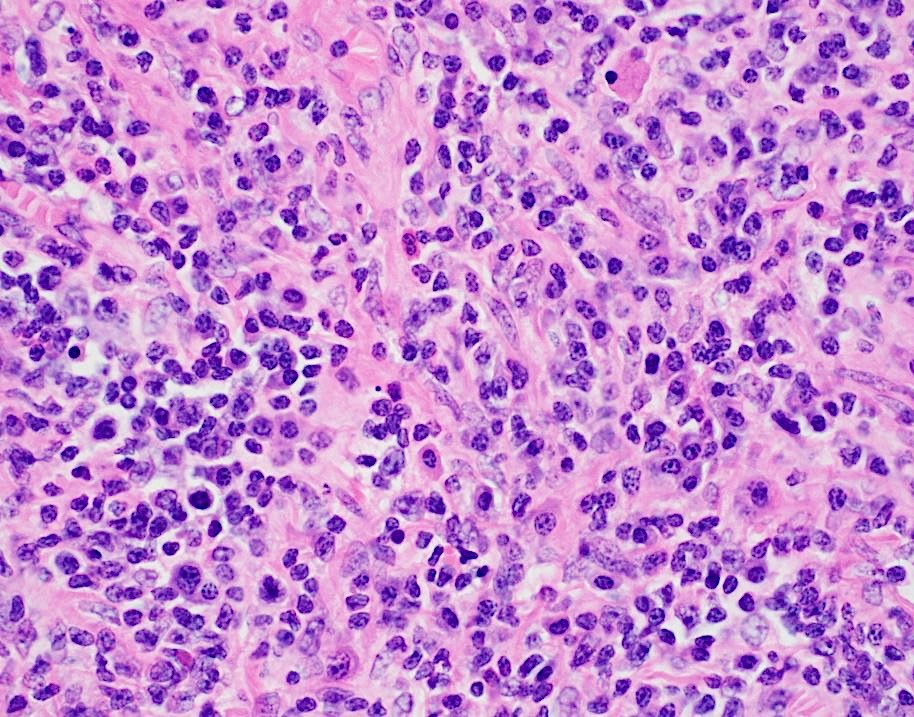
At low power view, there is intact follicular architecture
with reactive appearing germinal centers that are polarized and show tingible
body macrophages. The higher power view shows a feature that can be seen in
Castleman disease called a “lollipop” which has a thickened vessel with
hypertrophied endothelial cells penetrating the germinal center. In addition,
there are areas with sclerotic remnants of germinal centers, a feature that can
be seen in infection or other reactive conditions. Notably, the interfollicular
space is expanded by numerous plasma cells and rare scattered eosinophils. Overall,
the lymph node shows reactive follicular and paracortical hyperplasia. Stains
for IgG and IgG4 showed an elevated IgG:IgG4 ratio with 54% of IgG plasma cells
positive for IgG4. These findings raise the possibility of IgG4-related
lymphadenopathy (IgG4LAD). In addition to histopathologic findings, the patient
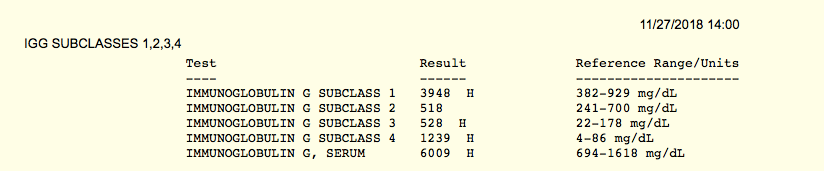
was tested for a serum IgG4 level, which is an important diagnostic criterion
for the diagnosis of IgG4 disease. Seen above, serum testing on 10/25/18 showed
a low/normal IgG subclass 4 of 17 mg/dl. After the excisional biopsy was
performed, suspicion of involvement by IgG4-related disease increased. A sample
was re-sent on 11/27/18 with instructions to perform serial dilutions in case
of the prozone effect (see discussion below). The test came back with an elevated
serum IgG subclass 4 of 1239 mg/dl, further supporting the diagnosis of
IgG4-related disease.
Discussion
IgG4-related disease is a condition that was originally
described in patients with autoimmune pancreatitis. These patients were found
to have elevated serum IgG4 concentrations and have large numbers of IgG4-positive
plasma cells. IgG4-related disease is now recognized as a fibroinflammatory
condition and has been described in almost every organ system. Similar
histopathological characteristics can be seen regardless of location and
include tumefactive lesions, dense lymphoplasmacytic infiltrate, increased
IgG4-positive plasma cells and storiform fibrosis.1
IgG4 normally accounts for less than 5% of the total IgG in
healthy people and is the least abundant IgG subclass. IgG4 is also seen to be
involved in other immune-mediated conditions such as pemphigus vulgaris,
idiopathic membranous glomerulonephritis, and thrombotic thrombocytopenic
purpura. The majority of patients with IgG4-related disease have elevated serum
IgG4 concentrations, but 30% of patients may have normal IgG4 concentrations.1
When testing IgG4 serum levels, it is important to be aware of the prozone
effect. This occurs when very high concentrations of the antibody that is being
measured are present. This will prevent appropriate antibody-antigen binding
and agglutination from occurring. This will result in a falsely low level of
antibody being detected. In a report by Khosroshahi et. al., after identifying
the prozone effect in one patient with IgG4-related disease, 38 patients who
had previously been tested for serum IgG4 levels were re-tested. The prozone
effect was found to affect 26% of patients with IgG4-related disease. The
samples were re-tested with serial dilutions and the mean serum concentration
rose from 26 mg/dl to 2,008 mg/dl. This could have a large impact on patient
care, as elevated serum IgG4 concentrations are very important in making the
diagnosis of IgG4-related disease. 2
IgG4-related lymphadenopathy (IgG4LAD) is somewhat distinct
from tissue based IgG4-related disease and presents with solitary or multifocal
lymph node enlargement. Lymph nodes are involved by a lymphoplasmacytic
infiltrate with increased IgG4-positive plasma cells and tissue eosinophils and
are not typically involved by storiform fibrosis. Five microscopic subtypes
have been described and include multicentric Castleman disease-like changes, follicular
hyperplasia, interfollicular lymphoplasmacytic proliferation, progressive
transformation of germinal centers, and a variant with the formation of
inflammatory pseudotumor-like lesions. The differential diagnosis of this
entity is broad and purely reactive lymph nodes as well as multicentric
Castleman disease (MCD), in particular needs to be ruled out. The presence of
HHV8 infection and elevated IL-6 and CRP can favor MCD, while tissue
eosinophilia favors IgG4LAD.3
The diagnostic criteria for the diagnosis of IgG4LAD
includes lymph node involvement, a serum
IgG4 level greater than 135 mg/dl, and histologic findings of lymphoplasmacytic
infiltrates with either >10 IgG4-positive plasma cells per hpf or a ratio of
IgG4-positive to IgG-positive plasma cells to be greater than 40%. As seen in
this case, patients may undergo multiple biopsies, often with extensive
work-ups before a diagnosis is made. Treatment depends on the organ involved
and extent of damage/dysfunction. While some cases may only need clinical
follow-up, others will require urgent aggressive treatment. Glucocorticoids are
typically the first line of therapy and have been shown to be effective in a
majority of patients with IgG4-related disease. 3
References
Stone, J, Zen, Y, Deshpande, V. IgG4-Related
Disease. N Engl J Med 2012;
366:359-551.
Khoroshahi, A, Cheryk, LA, Carruthers, MN, et.
al. Brief Report: spuriously low serum IgG4 concentrations caused by the
prozone phenomenon in patients with IgG4-related disease. Arthritis Rheumatol 2014; 66(1):213-7.
Wick, M, O’Malley, D. Lymphadenopathy associated
with IgG4-related disease: Diagnosis and differential diagnosis. Seminars in Diagnostic Pathology 2018;
35(1)61-66.
–Chelsea Marcus, MD is a third year resident in anatomic and clinical pathology at Beth Israel Deaconess Medical Center in Boston, MA and will be starting her fellowship in Hematopathology at BIDMC in July. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
This is a longer one but, to me, there’s a lot of
interesting stuff I wanted to share with all of you!
(TL;DR Path and Psych
aren’t too different, but they are. There
are interesting overlaps, and doing research right is really critical.)
The last month of 2018 has me rotating through my psychiatry clerkship in medical school. With that, I’ve had an interesting opportunity to look at pathology from a very distant lens. (Very distant; think diminutive picture of Earth from Mars far…) During one grand rounds session, Dr. Owen Muir, the medical director of Brooklyn Minds said something to the effect of, “[people say] Psychiatry is different, so much so that we’re the most removed from our tissue of concern.” That was pretty poignant. He was talking about the brain; in testing, treatment, and practice, it’s virtually inaccessible without a major neurologic undertaking and almost unreachable between pharmaceutical and external therapeutic interventions. Here’s the same thought another way: a neuropathologist can show you what parts of the brain do what in a particular pathologic process grossly and microscopically, while psychiatry focuses on pharmacologic, cognitive, and comprehensive behavioral therapies. A microscope versus a telescope—but both a way to focus on a problem. When I compared that to some things I heard during my orientations, it became clear that Psychiatry and Pathology might be very different animals.
I’ll get back to Dr. Muir and the Brooklyn Minds’ work with cutting-edge deep Transcranial Magnetic Stimulation (dTMS)—yes magnets—in just a minute. First I want to show you that, despite being light-years apart in distance, these two specialties overlap more than people realize. No, not with regard to behavioral stereotypes; read my previous post on stereotypes in lab medicine, and let’s get that out of the way right off the bat. The foundational concept which continues to bring every specialty closer together is translational research. Consider the following, if the field of Medicine was a tree, specialties would be complex branches and basic scientific principles would be the roots of knowledge. And what connects the roots to the branches? All the years of scientific research that translates data gathered from experimentation in fields like physiology, microbiology, or chemistry into specialties like nephrology, infectious disease, or endocrinology. Wait! That’s pretty much our job—duh. Cool, so since we translate the data, we’re all the junk in the trunk! So within the realm of research in medicine, I want to show you examples of cutting edge limitations, intersectional data sharing, and shortcomings in translational research.
Cutting edge or the
bleeding edge?
So, I mentioned Brooklyn Minds. Sounds dramatic, like a movie title; but you won’t find any groundbreaking 90’s soundtrack by Coolio or a Michelle Pfeiffer-driven story about inner city youth. Instead, what their webpage outlines very nicely is the important and impactful work they do in psychiatry which includes repetitive or deep therapeutic magnetic stimulation (rTMS/dTMS). I promised I would explain the magnets thing, okay so here goes. Essentially, dTMS is a pulsatile magnet-driven energy wave directed at specific regions of a patient’s head. The energy works like a magnetic field to activate or inhibit (think “polarize” or “depolarize”) small patches of neurons within the brain, penetrating beyond the bony cranial vault and centimeters into the parenchyma of brain tissue. Using a premise which is basically similar to an MRI, patient’s brains are “mapped” for functional region analysis—a new, subtler way of looking into focal deficits. Two major mental illness that dTMS has literature supporting treatment include Major Depressive Disorder (MDD) and Obsessive Compulsive Disorder (OCD). So first, you have to understand one thing: neurons are basically our electrical circuitry, conducting energy potentials as signals back and forth translating and calculating motion, sensory input, and position. If nerves are electrical wires, think of myelin as a conductive insulator for higher signaling strength. The conduction potentials of certain mapped regions of the brain demonstrate decreased activity in particular areas with corresponding anatomical locations where we know disease processes can occur. For example, we understand the changes in brain chemistry to treat it pharmacologically, but depression has visible impacts on the hippocampus and prefrontal cortex. Why not treat this directly, like the way a surgeon would treat a hernia?
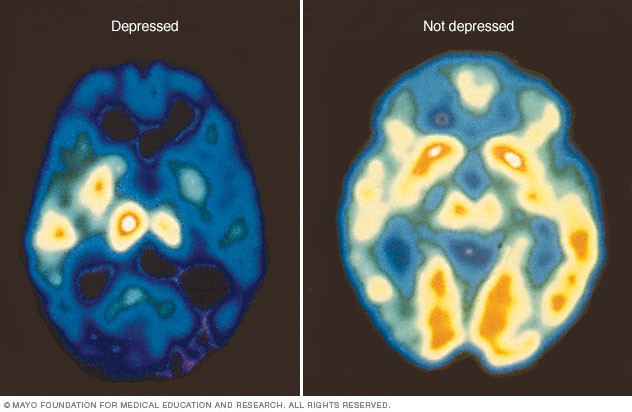
Image 4: Let’s take depression, for example. In the PET scan on the right, you can see what a “normal” brain functional status is mid-scan. On the left, however, would be a “depressed” brain. With cortisol in surge-mode and a poverty of available serotonin and norepinephrine in the brain, you can see widespread variable activity from the amygdala, hippocampus, prefrontal cortex, and beyond. (Source: Mayo Clinic)
This seems like some next-level Doctor Who science, right? So, the biggest question here would be: does this work? Since TMS (of which there are multiple types, with special equipment—not important for this discussion) is a medication-free treatment, doesn’t this sound almost perfect? Combine that with the fact that dTMS treatments often potentiate positive response for follow up treatment since the “rewiring” promotes future effectiveness and this might sound too good to be true. Studies are being published by the pound hailing this type of therapy as a potential life-saver for psychiatry which has been struggling to contribute longitudinal positive outcomes for patients. Evidence is strong for the use of dTMS in a variety of mental health issues, but it’s still early—you might find studies with large number of subjects, but you might not find ones with long-term analyses. So the research today is overwhelmingly positive and there are multiple studies in published literature about the effectiveness of this therapy in depression resistant to medication, or the utility as a maintenance therapy in an outpatient setting, or even potential use for substance use disorders. But, there are skeptics just as vocal as supporters. (Side note: If Dr. Oz does a story on a treatment like TMS, do we have to abandon it and move on completely?) As an emerging therapy, Psychology Today published a consumer report of sorts which discussed issues like access, refractory response, and more proven standard therapy like ECT (electroconvulsive therapy). Although it is FDA approved and non-invasive (minus some potential headaches), questions about TMS address things like how to get insurance to cover it, should it be reserved as a last resort after things like medications/ECT, and since it’s a relatively new treatment should we pursue more longitudinal studies first?
Image 5: Have a seat! This instrument has the potential to treat a myriad of psychiatric illnesses by using magnetic fields aimed at “adjusting” improperly firing neurons in the brain. Research still remains outstanding as to whether dTMS can affect someone’s …magnetic personality. (Source, except for my pun: Cognitive Psychiatry of Chapel Hill)
Taking it back to the
source
Way back in the beginning of 2018—if you can remember such a time—an article was quietly published in the journal Science. This was a large collaboration funded by the National Institute of Mental Health (NIMH) among many other supporters, with a team that spanned from UCLA, to Denmark, to Chicago (woot!). Printed in the section header “Psychiatric Genomics,” it was called “Shared Molecular Neuropathology Cross Major Psychiatric Disorders Parallels Polygenic Overlap”—wait, what? Yes, among some major psychiatric disorders we all know, love, and read about in the DSM-5, some of them share specific genetic mutations. Full stop. Pivot. Let’s leave our Freudian couch and walk over to the lab…
Image 6: Experimental rationale and design where section (A) illustrates the model of proposed psychiatric disease pathogenesis and the authors’ (B) experimental process which they concluded was “highly suggestive of a causative genetic component” (Source: Gandal et al. 2018, Science 359, 693–697)
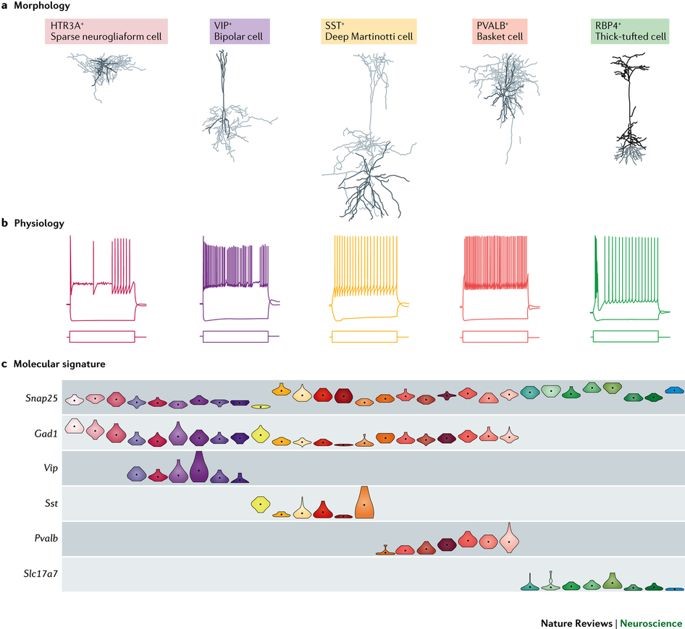
What these authors suggest is that five major psychiatric disorders—autism spectrum disorders (ASD), schizophrenia (SCZ), bipolar disorder (BD), major depressive disorder (MDD), and alcohol abuse disorder (ADD)—all share specific gene-expression changes which indicate transcriptional dysregulation (i.e. mutations) at single nucleotide polymorphism (SNP) locations which is very consistent with inheritable genetic variants. In short, small, specific mutations seem to be identifying features for those five disorders, which might reveal genetic risk and potential future treatment targets. Even more than this, what we see commonly as overlapping features in patients’ clinical presentations may actually be explained by overlapping genetic expression and penetrance. We’ve long had historical evidence supporting the hypothesis of mental illness as an inheritable disorder. Twin studies have shown the increased probability of expressed diseases like bipolar disorder or schizophrenia in monozygotic twins compared to dizygotic ones—but the twins’ clinical presentations don’t always yield 100% confidence there. Clinicians are acutely aware of the genetic component present in diseases like these, but targetability has proven difficult. According to the National Institute(s) of Health and Mental Health (NIH/NIMH), “strong evidence may exist for genetic susceptibility, but no specific gene has been unambiguously identified for common forms of mental disorders,” and “the estimate of the influence of environmental factors on the disorder provides an index of how difficult the search will be.” (Source: NIH/NIMH Genetics and Mental Disorders: Report of the National Institute of Mental Health’s Genetics Workgroup – Mental Disorders and Genetics: What We Know Today) That was in 1997! A similar paper to this one published in The Lancet in 2013 addressed these same five psychiatric disorders correlating some genetic components to a region on Chromosome 3 against almost 30,000 normal/wild-type patients. The NIH responded then saying that though there were significant correlations presented therein, there isn’t enough evidence to show the risk associated with the mutation and further research is necessary. Fast forward to some further research and we now see evidence of overlap between particular mental illnesses as well as cell-to-cell signaling as a specific neuropathological mechanism of disease. Is it enough for a Nobel Prize? No. But think of it somewhere between a paper titled “We’ve Discovered Insulin!” and “Patients with Diabetes Often Have Elevated Blood Glucose.”
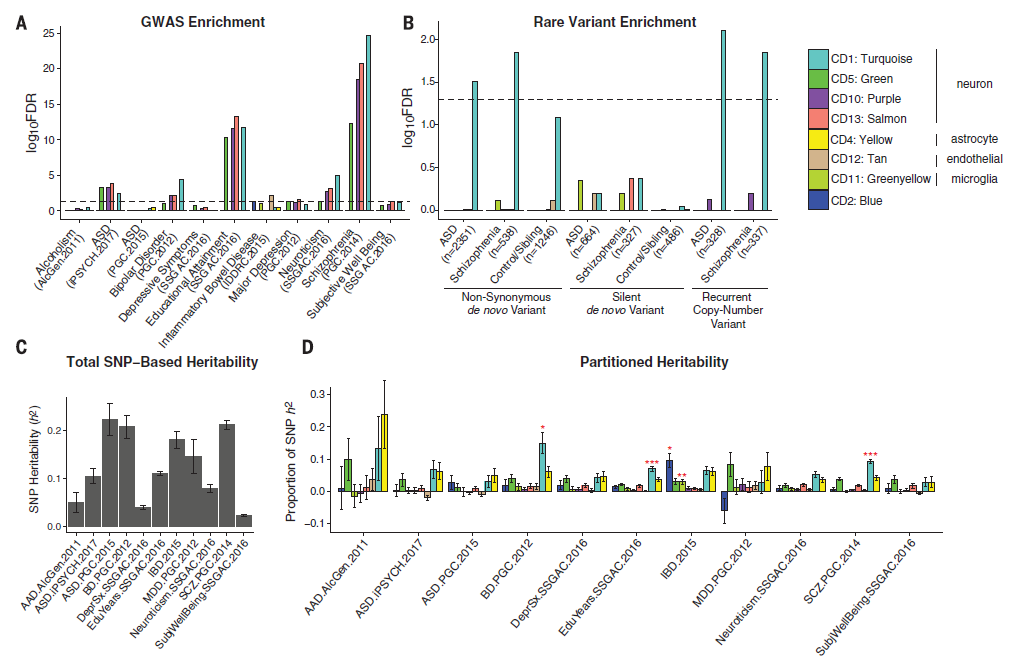
Image 7: Evidence to suggest that certain gene expression patterns overlap which demonstrates transcriptosome similarity between various two-disease combinations/overlaps (A) and that there seems to be a spectrum or progression of disease intensity relating to a gene’s mutability (B). However, gene expression can both show that normal biologic function can be associated with these variants (C) and that, even though disease overlap implies correlation, ASD seems to mutate independent from the rest (D). (Source: Gandal et al. 2018, Science 359, 693–697)Image 8: Hub genes are targets of research because of they are modeled as functionally significant markers of genetic variation and/or mutability. In this abbreviated data infographic, the top 20 gene hubs were collected for their association with gene activity in each of the five diseases. The functional aspects represent mutations (colored circles) in various aspects of neuronal cells including receptor activity (dark blue), mitochondrial structure (green), immune response/regulation (yellow-green), mitochondrial metabolism (purple), neuronal activity (pink and light blue), cellular architecture and growth (tan), and other neuronal metabolism (yellow). The lines connecting these mutations are a representation of Eigengene networking, which illustrate gene co-expression and functional relationships. (Source: Gandal et al. 2018, Science 359, 693–697)Image 9: What’s the take-home message here? Basically, the final conclusion is this: take all these demonstrated mutations as functional pieces of mental health and down-regulated neuronal expressions of genes highlight potential risk stratification. Genome-wide association studies (GWAS) shows high concentrations for SCZ, ASD, and BD variants (A) and those variants presence in the neuronal model for various nerve cell types is shown (B). The main lesson here is the projected diagnostic liability and risk assessments for patients who have these specific mutations (C & D) which may be correlated to this research’s co-expression models. (Source: Gandal et al. 2018, Science 359, 693–697)
Correlation does NOT
imply causation, but isn’t it so tempting!
While promising articles like these offer amazing potential insights into a deeper understanding of clinical diagnostics for psychiatry, articles are as numerous and complex as patients. An article published this month from the Journal of the American Medical Association (JAMA)Psychiatry correlated an association between hospitalization and subsequent mental disorders in children. Anything that purports to associate new causality between disease entities and trends is always worth a read. And, like any other experienced clinician, you go straight to the title and design methods to determine your gut feeling about this paper before continuing. The title: “A Nationwide Study in Denmark of the Association between Treated Infections and the Subsequent Risk of Treated Mental Disorders in Children and Adolescents;” the number of patients studied: over 1 million. What? That’s amazing! 1 million cases, what amazing data, what amazing insights, what …a statistical nightmare. Finding results in a million is both exhaustively comprehensive and statistically problematic. Black holes are rare. But if you search the entire universe you’ll find millions. “With a large enough sample size, rare things become common…” this was said with a pregnant pause and the normal gravity delivered by astrophysicist Neil DeGrasse Tyson, PhD, during a live taping of Star Talk my wife and I attended a month ago.
Image 10: From Star Talk, November 14th at the Beacon Theatre in NYC, left to right: co-host and comedian Eugene Mirman, actress Ellie Kemper, comedian John Mulaney, scientist Julie Huber from Woods Hole Oceanic Institution, scientist Kevin Hand from the NASA Jet Propulsion Lab, and co-host and astrophysicist Neil DeGrasse Tyson. The show discussed life on other worlds, and the realistic expectations of research and what to look for when you’re looking for life in space. The most poignant point of the night came during Dr. Tyson’s conclusion where he talked about different specialties growing apart and coming together over the last few hundreds of years—we used to have an isolated biologist and astronomer, where today astro-biology is a new exciting front!
What came up during that show was the same theme I’m
discussing today: it’s very important to do research, collect data, and
translate that data appropriately. Especially in medicine, where conclusions
and results from research can affect patient outcomes, lab professionals like
us need to be leaders.
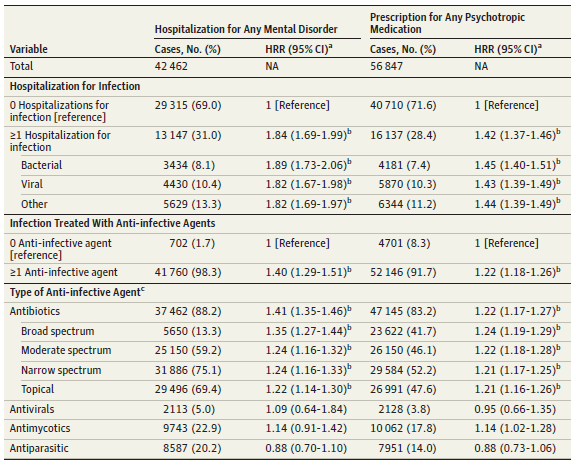
Back to this paper, the authors report a strong significant correlation between hospitalization events requiring antibiotics and the prevalence of mental illness later in life. Analyzing the hazard risk ratio (HRR) for these patients reveals values usually over 1.0 which show that they are above the regular risk when compared to patients not under these conditions. The authors associate treated infections with childhood/adolescent mental disorders, but include a very important remark at the very end which is ever-present in most good research. They address the fact that results and conclusions from their data may be explained by other, non-studied causes directly because of otherwise not understood pathophysiology. And, like 99% of pathology reports I’ve seen end with a dogmatic “suggest clinical correlation,” this paper closes with something similar to “further research is needed.”
Image 11: Hazard risk ratios (HRRs) here demonstrate that individuals requiring hospitalization for infection were increased (with high confidence analysis) for having a hospitalization for any mental disorder and for redeeming a prescription for any psychotropic medication. (Source: JAMA Psychiatry 2018. doi:10.1001/jamapsychiatry.2018.3428)Image 12: You can find tons of funny causation-correlation infographs on the internet. They prove a great point: we have to be careful how we translate our data. Without arguing that because higher global temperatures melt the icecaps pushing more sailors to a life of pillage and plunder, these two findings are assuredly non-related.
So that’s it! Using data is great! It’s the best. Translating direct and clinically relevant findings from the bench to the bedside is what we do best. Consulting with our clinical colleagues, those of us in laboratory medicine have a responsibility to make sure of four main things. First, we have to make sure that the results we obtain are clear. Pre-to-post analytical analysis is paramount to testing efficacy and we’re the experts on standard procedures and accountability. Second, the interpretation of results whether it comes from a research lab or hematology bench must be valid. Protocols and metrics are great, and using them to ensure effective use of information is critical. Third, the conclusions we reach should be meaningful. If it’s a cancer staging diagnosis biopsy report or a groundbreaking publication on shared genetic variants, the implications must provide the best information for patients. Because finally, we do what we do for them. Our work and efforts always go back to improving patient outcomes, and giving each person the best chance at maximum health and quality of life. Pathology and psychiatry might be worlds apart, but only in vocabulary at best. We’re on the same team. And, despite finding each other as great neighbors in most Medscape physician job reports, we both work very hard to lead the charge in protecting, healing, and advocating for our patients.
Wishing you good mental health! Even outside the Seattle area, fictional Dr. Frasier Crane’s “I’m listening” catch phrase is great advice toward patients, colleagues, and generally everyone. Leadership is a great responsibility, but it’s worth nothing if you don’t pay attention to what needs to get done.
For our next edition of transgender laboratory medicine, we will explore how transgender women use hormone therapy to physically transition to their affirmed female gender. While transgender men just take testosterone, transgender women take both estradiol and an anti-androgen. In the United States, that anti-androgen is spironolactone.
Figure 1. I was amazed in freshman biology by how structurally similar these hormones were and how they lead to such dramatically different phenotypes. Spironolactone is quite a bit different with the same cholesterol backbone. Credit Wikipedia
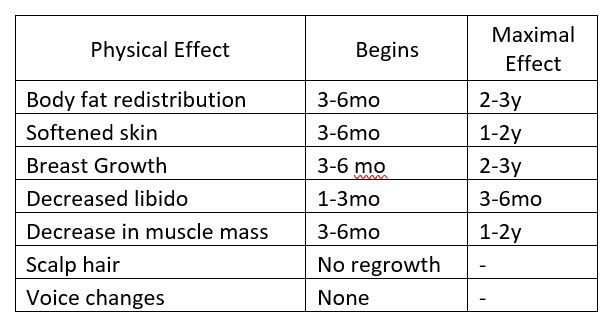
Estradiol is administered either as an oral pill, an injectable liquid or a transdermal patch. The estradiol pills are the cheapest option as they have been made generic for use as birth control. The transdermal can be the easiest to use, but is also the most expensive version and may not deliver as much estradiol as the other routes. Oral estradiol usually starts in adults at a low-dose (2 mg) then is titrated up to 4-6 mg and rarely up to 8mg. The end-point of estradiol titration is not to reach a certain hormone level, but to achieve desired physical traits. Endocrine guidelines do suggest keeping estradiol levels below peak physiologic levels (200 pg/mL).1 While little evidence currently exists for side effects of supraphysiologic estradiol, blood clots are a serious known side effect.
Part of the reason for anti-androgens in treating transgender women, is that even in women, testosterone levels are orders of magnitude higher. Spironolactone is primarily used as a glucocorticoid analog to block the mineralocorticoid receptor in the kidney to induce diuresis while retaining potassium. The structure of spironolactone is similar enough totestosterone that it also binds the androgen receptor and blocks the effect of testosterone. While enlarged breasts are considered a side effect in heart failure patients, it is an intended effect of spironolactone in transgender women. While hyperkalemia (high potassium) is a well known adverse effect of spironolactone, it seems to manifest more in patients with co-morbid conditions such as heart or kidney failure rather than in healthy patients.2
Table 1. This table describes the time frame of physical traits that manifest in transgender women while taking feminizing hormone therapy. Based on Hembree et al. 2017 (1).
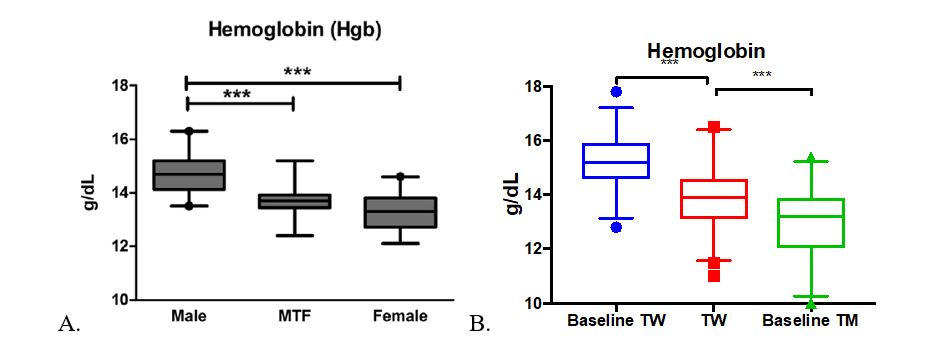
For feminizing hormone therapy, red blood cell indices are the one of the most responsive laboratory parameters. The hemoglobin, hematocrit, and RBC number are all seen to decrease during hormone therapy in transgender women. A previous study of 55 transgender women3 showed that hemoglobin levels decreased significantly from cis-gender male levels to be not significantly different from cis-gender female hemoglobin. With a larger patient group, we were able to confirm this previous finding of decreased hemoglobin, but transgender women’s hemoglobin levels are still significantly different from individuals with sex-assigned female at birth (Figure 2).
Figure 2. A. Figure from Roberts et al 2014. B. TW= Transgender women, Baseline TW= TW with no history of hormone therapy, Baseline TM= transgender men with no history of hormone therapy. ***p<0.0001 Data expressed as interquartile range with median (box) and 2.5th to 97.5th percentile (whiskers).
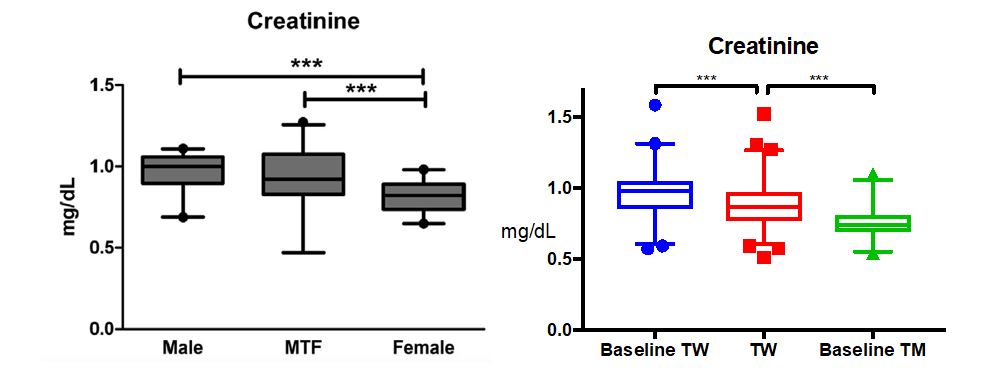
Roberts et al also found that creatinine levels remain closer to cisgender male levels compared to cisgender female creatinine values3. This brought up the concept that not all lab values change predictably to the reference interval of the opposite gender. We further confirmed this finding in our larger cohort, but we further found a significant difference in transgender women from their baseline levels (Figure 3).
Figure 3. A. Figure from Roberts et al 2014. B. TW= Transgender women, Baseline TW= TW with no history of hormone therapy, Baseline TM= transgender men with no history of hormone therapy. ***p<0.0001 Data expressed as interquartile range with median (box) and 2.5th to 97.5th percentile (whiskers).
Overall, red blood cell and creatinine levels change the most in transgender women taking hormone therapy, but they don’t go as far as being comparable to lab values of individuals of the opposite sex assigned at birth. Our summary of this data will be published soon and interested labs can note what we found to be the central 95th percentile of common lab values including those presented here. I will go into greater detail about some unexpected effects of hormone therapy in following blog posts. I hope you’re looking forward to it as much as I am!
References
Hembree WC,Cohen-Kettenis PT, Gooren L, Hannema SE, Meyer WJ, Murad MH, et al. Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society*Clinical Practice Guideline. J Clin Endocrinol Metab. 2017
Roberts TK, Kraft CS,French D, Ji W, Wu AHBB, Tangpricha V, et al. Interpreting Laboratory Results in Transgender Patients on Hormone Therapy. Am J Med. 2014;127:159–62.
Plovanich M, Weng QY,Mostaghimi A (2015). “Low Usefulness of Potassium Monitoring Among Healthy Young Women Taking Spironolactone for Acne”. JAMA Dermatol. 151 (9):941–4.
-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and advancing quality in molecular diagnostics.