Case History
A 64 year old male presented with a one year history of loose stools, lower abdominal crampy/gassy pain that improved with defection, and an unclear history of melena. A colonoscopy revealed a circumferential, villous, carpet-like lesion extending from 15 cm to the anal verge, with biopsies demonstrating fragments of a villous adenoma. A follow-up CT scan was negative for metastatic disease. The decision was then made to proceed with a low anterior resection with hand-sewn colo-anal anastomosis and diverting loop ileostomy.
Diagnosis
Upon opening the rectum, a 13.8 cm long circumferential, carpet-like lesion is identified, extending to the distal margin (Image 1). Sectioning demonstrated a lesion with a maximum thickness of 1.0 cm, which grossly appears to be confined to the mucosa. Due to the prior biopsy history of a villous adenoma, the entire lesion was completely submitted. This required 116 blocks to be submitted, which were then mapped out to show where each block would have been taken from (Image 2). Although there were many foci of intramucosal carcinoma present, clear cut submucosal invasion was not identified, and the specimen was signed out as a villous adenoma (Image 3).


Discussion
Polyps are an abnormal tissue growth that is a common occurrence within the colon, although they can also be found throughout the small intestine, stomach and esophagus. Polyps can be further classified as being neoplastic or non-neoplastic based on the histological pattern of the cells. The most common types of neoplastic polyps found within the GI tract are colonic adenomas, which are benign polyps that serve as precursors to the majority of colorectal cancers. Nearly half of adults in the Western world will develop adenomas by the age of 50, and there is no gender predilection. It is because of this that it is recommended that all adults get a colonoscopy by the age of 50 (even earlier when there is a family history of developing colorectal cancer).
Most polyps are small, measuring 0.5 cm or less, but can grow to be over 10 cm in size (as seen in this case). When a colonoscopy is performed, these polyps can appear as sessile, meaning flat, or pedunculated, meaning on a stalk. Due to the abnormal epithelial growth of the mucosa, the surface of an adenoma can have a velvety appearance, resembling that of a raspberry. Most patients will not demonstrate any symptoms from their polyps, with the exception of occult bleeding and anemia which are associated with larger polyps.
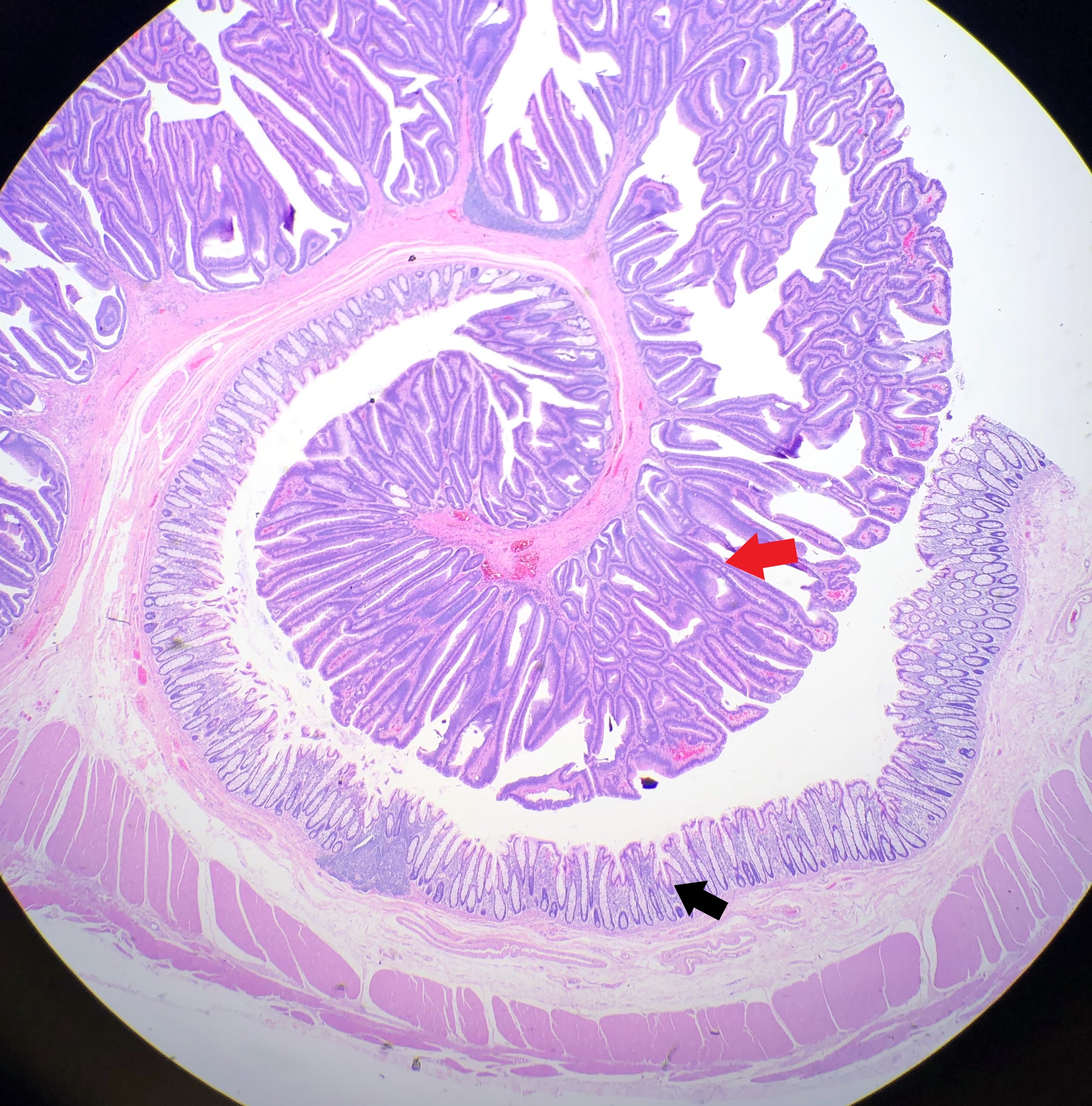
Dysplasia, which literally means “disordered growth”, occurs when the individual cells lose their uniformity and architecture, often resulting in cells with a hyperchromatic nuclei and a high nuclear to cytoplasmic ratio. The presence of dysplasia contained within the epithelium of a polyp is what classifies the polyp as an adenoma (Image 4). Based on their epithelial growth pattern, adenomas can be classified as either tubular adenomas or villous adenomas. Tubular adenomas tend to be smaller polyps, with a smoother surface and rounded glands on histologic examination. Villous adenomas, in contrast, tend to be larger polyps with long, slender villi noted on histology (Image 5). If an adenoma contains a mixture of tubular and villous elements, they are classified as tubulovillous adenomas. When a dysplastic cell is no longer contained within the epithelium, and instead breaches the basement membrane which separates the epithelium from the underlying tissue, it is termed invasive.


What makes this case so interesting is that there is a direct correlation between the size of an adenoma, and the risk of developing colorectal cancer. This is not true with most other cancers, however, as size plays no part in determining whether the tumor is cancerous or not. With colon polyps, the larger the polyp, the greater the chance of developing invasive carcinoma (i.e. cancer). This is why screening colonoscopies are so important. Studies have shown that regular colonoscopies, combined with the removal of the polyps found on the exam, reduce the incidence of colorectal cancer. Why this case is so interesting is that you could assume based on the size of this polypoid lesion, you would find some invasive component. However, after reviewing 116 blocks, not a single focus of invasion could be identified.
It should be stated that although there is a correlation between an adenomas size and the risk of developing cancer, the majority of adenomas will not progress to cancer, and in fact, there are no tools currently available that help to determine why one patient’s adenoma will progress to cancer, while another patient’s adenoma will not.
References
- Association of Directors of Anatomic and Surgical Pathology, adapted with permission by the American Cancer Society. Understanding Your Pathology Report: Colon Polyps (Sessile or Traditional Serrated Adenomas). cancer.org. https://www.cancer.org/treatment/understanding-your-diagnosis/tests/understanding-your-pathology-report/colon-pathology/colon-polyps-sessile-or-traditional-serrated-adenomas.html. Accessed February 14, 2019.
- Colon Polyps. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/colon-polyps/symptoms-causes/syc-20352875. Accessed February 14, 2019.
- Turner JR. Polyps. In: Kumar V, Abbas AK, Fausto N, Aster JC. Robbins and Cotran Pathologic Basis of Disease, 8th edition. Philadelphia, PA: Elsevier, Inc; 2010: 815-820

-Cory Nash is a board certified Pathologists’ Assistant, specializing in surgical and gross pathology. He currently works as a Pathologists’ Assistant at the University of Chicago Medical Center. His job involves the macroscopic examination, dissection and tissue submission of surgical specimens, ranging from biopsies to multi-organ resections. Cory has a special interest in head and neck pathology, as well as bone and soft tissue pathology. Cory can be followed on twitter at @iplaywithorgans.
