The correct answer is the last option. G3 PNETs (or high grade PNETs) have a well-differentiated morphology but an elevated proliferation rate. G3 PNETs are more likely to be diffusely positive for neuroendocrine markers, are not as aggressive as poorly differentiated NECs, and do not have the same genetic abnormalities as NECs. G3 PNETs are less responsive to platinum-based therapy than are poorly differentiated NECs. Please also see Case 2 discussion for additional information about PNECs.
Standard staging evaluation of patients with WD PNETs:
- Recommended:
- Abdominal multiphasic CT or MRI
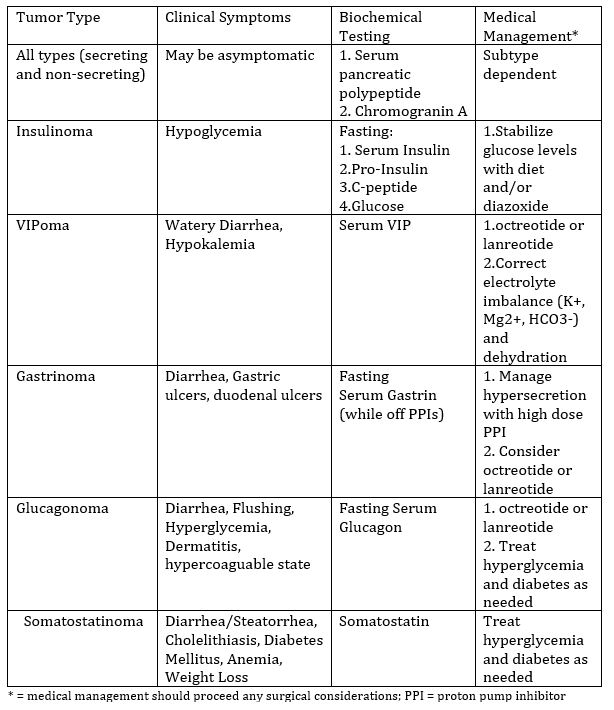
- Biochemical evaluation if functional tumor (see Table 1, highlighted is our case presentation of insulinoma)
- As appropriate:
- Somatostatin receptor-based imaging (i.e. 68Ga-dotatate PET/CT [preferred] or somatostatin receptor scintigraphy)
- Chest CT +/- contrast (may be omitted for non-functional)
- Endoscopic ultrasound (EUS)
- Further biochemical evaluations
- Consider testing for inherited genetic syndromes