Authors: Dr. Maryam Zenali (Department of Pathology), Dr. Eric Ganguly (Department of Gastroenterology), and Dr. Christopher J. Anker (Division of Radiation Oncology), University of Vermont Medical Center
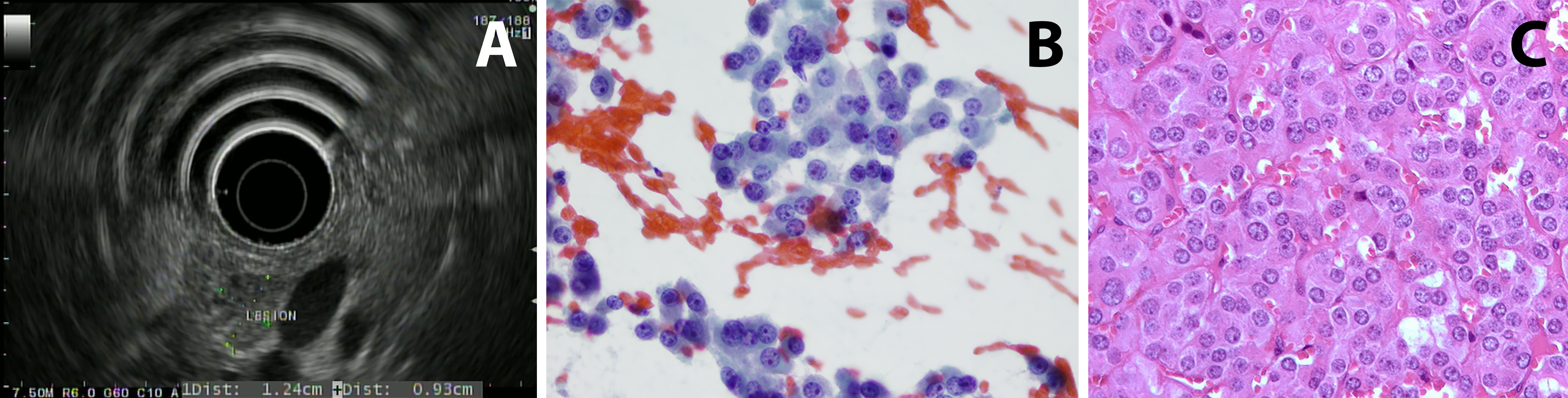
Case 1: Patient 1 is a 75 year old man with a history of gastroesophageal reflux disease (treated with a proton-pump inhibitor) who had an episode of diaphoresis and altered mental status at 3:30 am. He was found to have a glucose of 20 when rescue arrived. He was brought to the ED and symptoms resolved after glucose administration. Work-up showed fasting C-peptide of 3.5 (normal range: 1.1-4.4 ng/mL) ruling out excess insulin use; proinsulin was elevated at 300 (normal range: 3-20 pmol/L). Serum chromogranin A was noted to be mildly elevated. He had a CT scan of the abdomen that did not show any abnormal enhancement or concerning lesion. Endoscopic ultrasound (EUS) imaging demonstrated a slightly hypoechoic mass in the pancreatic head with a hyperechoic halo margin. The mass was adjacent to, although not invading, the portal vein. The remainder of the pancreatic head had a normal echotexture (figure 1A). Fine needle aspiration and biopsy of the lesion were performed; microscopic images are provided (figures 1B and 1C).
Histology: A relatively monotonous, well-differentiated tumor with regular, round salt-and-pepper chromatin and eosinophilic cytoplasm. There were only rare apoptotic cells and no mitosis. 1% of tumor nuclei were immunoreactive with MIB-1 (Ki67 K2 Leica). Tumors cells were diffusely and strongly positive for synaptophysin (27G12, Leica), chromogranin (LK2H10, Ventana) and keratin (AE1-AE3, Biocare) but negative for makers such as TTF1, CK7, Beta-catenin and GATA-3.
What is most likely the diagnosis?
