Welcome back! Thank you for the messages and shares for last month’s post about how medical professionals like us should be leading the charge to address gun violence as a public health issue. It’s a hot-button topic, but I was really glad to engage in some great conversations. I want to stick with the theme of using data to improve patient outcomes, but this time I’d like to shift focus just a little bit.
This is a longer one but, to me, there’s a lot of interesting stuff I wanted to share with all of you!
(TL;DR Path and Psych aren’t too different, but they are. There are interesting overlaps, and doing research right is really critical.)
The last month of 2018 has me rotating through my psychiatry clerkship in medical school. With that, I’ve had an interesting opportunity to look at pathology from a very distant lens. (Very distant; think diminutive picture of Earth from Mars far…) During one grand rounds session, Dr. Owen Muir, the medical director of Brooklyn Minds said something to the effect of, “[people say] Psychiatry is different, so much so that we’re the most removed from our tissue of concern.” That was pretty poignant. He was talking about the brain; in testing, treatment, and practice, it’s virtually inaccessible without a major neurologic undertaking and almost unreachable between pharmaceutical and external therapeutic interventions. Here’s the same thought another way: a neuropathologist can show you what parts of the brain do what in a particular pathologic process grossly and microscopically, while psychiatry focuses on pharmacologic, cognitive, and comprehensive behavioral therapies. A microscope versus a telescope—but both a way to focus on a problem. When I compared that to some things I heard during my orientations, it became clear that Psychiatry and Pathology might be very different animals.

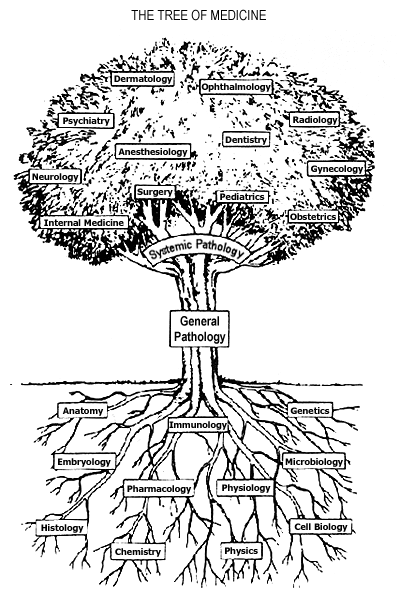
I’ll get back to Dr. Muir and the Brooklyn Minds’ work with cutting-edge deep Transcranial Magnetic Stimulation (dTMS)—yes magnets—in just a minute. First I want to show you that, despite being light-years apart in distance, these two specialties overlap more than people realize. No, not with regard to behavioral stereotypes; read my previous post on stereotypes in lab medicine, and let’s get that out of the way right off the bat. The foundational concept which continues to bring every specialty closer together is translational research. Consider the following, if the field of Medicine was a tree, specialties would be complex branches and basic scientific principles would be the roots of knowledge. And what connects the roots to the branches? All the years of scientific research that translates data gathered from experimentation in fields like physiology, microbiology, or chemistry into specialties like nephrology, infectious disease, or endocrinology. Wait! That’s pretty much our job—duh. Cool, so since we translate the data, we’re all the junk in the trunk! So within the realm of research in medicine, I want to show you examples of cutting edge limitations, intersectional data sharing, and shortcomings in translational research.
Cutting edge or the bleeding edge?
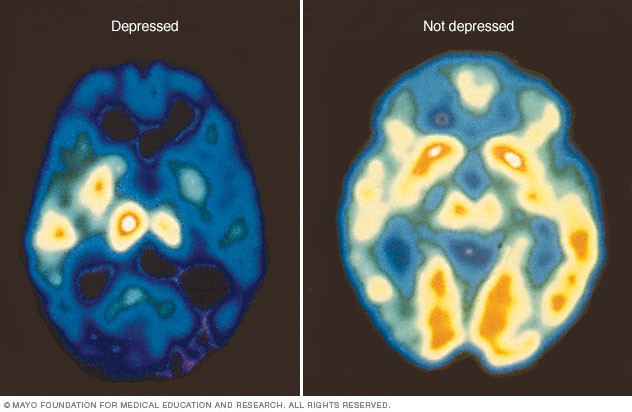
So, I mentioned Brooklyn Minds. Sounds dramatic, like a movie title; but you won’t find any groundbreaking 90’s soundtrack by Coolio or a Michelle Pfeiffer-driven story about inner city youth. Instead, what their webpage outlines very nicely is the important and impactful work they do in psychiatry which includes repetitive or deep therapeutic magnetic stimulation (rTMS/dTMS). I promised I would explain the magnets thing, okay so here goes. Essentially, dTMS is a pulsatile magnet-driven energy wave directed at specific regions of a patient’s head. The energy works like a magnetic field to activate or inhibit (think “polarize” or “depolarize”) small patches of neurons within the brain, penetrating beyond the bony cranial vault and centimeters into the parenchyma of brain tissue. Using a premise which is basically similar to an MRI, patient’s brains are “mapped” for functional region analysis—a new, subtler way of looking into focal deficits. Two major mental illness that dTMS has literature supporting treatment include Major Depressive Disorder (MDD) and Obsessive Compulsive Disorder (OCD). So first, you have to understand one thing: neurons are basically our electrical circuitry, conducting energy potentials as signals back and forth translating and calculating motion, sensory input, and position. If nerves are electrical wires, think of myelin as a conductive insulator for higher signaling strength. The conduction potentials of certain mapped regions of the brain demonstrate decreased activity in particular areas with corresponding anatomical locations where we know disease processes can occur. For example, we understand the changes in brain chemistry to treat it pharmacologically, but depression has visible impacts on the hippocampus and prefrontal cortex. Why not treat this directly, like the way a surgeon would treat a hernia?

This seems like some next-level Doctor Who science, right? So, the biggest question here would be: does this work? Since TMS (of which there are multiple types, with special equipment—not important for this discussion) is a medication-free treatment, doesn’t this sound almost perfect? Combine that with the fact that dTMS treatments often potentiate positive response for follow up treatment since the “rewiring” promotes future effectiveness and this might sound too good to be true. Studies are being published by the pound hailing this type of therapy as a potential life-saver for psychiatry which has been struggling to contribute longitudinal positive outcomes for patients. Evidence is strong for the use of dTMS in a variety of mental health issues, but it’s still early—you might find studies with large number of subjects, but you might not find ones with long-term analyses. So the research today is overwhelmingly positive and there are multiple studies in published literature about the effectiveness of this therapy in depression resistant to medication, or the utility as a maintenance therapy in an outpatient setting, or even potential use for substance use disorders. But, there are skeptics just as vocal as supporters. (Side note: If Dr. Oz does a story on a treatment like TMS, do we have to abandon it and move on completely?) As an emerging therapy, Psychology Today published a consumer report of sorts which discussed issues like access, refractory response, and more proven standard therapy like ECT (electroconvulsive therapy). Although it is FDA approved and non-invasive (minus some potential headaches), questions about TMS address things like how to get insurance to cover it, should it be reserved as a last resort after things like medications/ECT, and since it’s a relatively new treatment should we pursue more longitudinal studies first?

Taking it back to the source
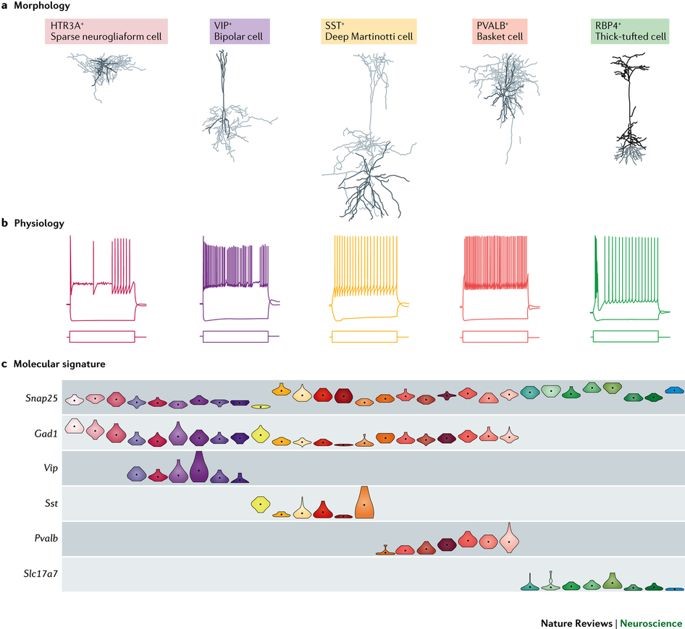
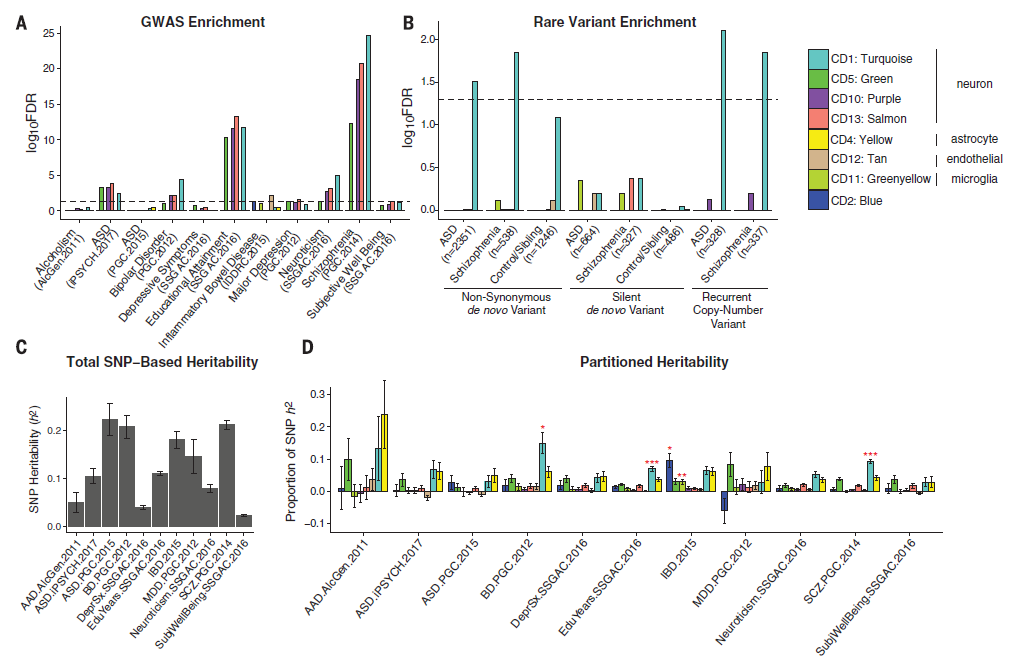
Way back in the beginning of 2018—if you can remember such a time—an article was quietly published in the journal Science. This was a large collaboration funded by the National Institute of Mental Health (NIMH) among many other supporters, with a team that spanned from UCLA, to Denmark, to Chicago (woot!). Printed in the section header “Psychiatric Genomics,” it was called “Shared Molecular Neuropathology Cross Major Psychiatric Disorders Parallels Polygenic Overlap”—wait, what? Yes, among some major psychiatric disorders we all know, love, and read about in the DSM-5, some of them share specific genetic mutations. Full stop. Pivot. Let’s leave our Freudian couch and walk over to the lab…

What these authors suggest is that five major psychiatric disorders—autism spectrum disorders (ASD), schizophrenia (SCZ), bipolar disorder (BD), major depressive disorder (MDD), and alcohol abuse disorder (ADD)—all share specific gene-expression changes which indicate transcriptional dysregulation (i.e. mutations) at single nucleotide polymorphism (SNP) locations which is very consistent with inheritable genetic variants. In short, small, specific mutations seem to be identifying features for those five disorders, which might reveal genetic risk and potential future treatment targets. Even more than this, what we see commonly as overlapping features in patients’ clinical presentations may actually be explained by overlapping genetic expression and penetrance. We’ve long had historical evidence supporting the hypothesis of mental illness as an inheritable disorder. Twin studies have shown the increased probability of expressed diseases like bipolar disorder or schizophrenia in monozygotic twins compared to dizygotic ones—but the twins’ clinical presentations don’t always yield 100% confidence there. Clinicians are acutely aware of the genetic component present in diseases like these, but targetability has proven difficult. According to the National Institute(s) of Health and Mental Health (NIH/NIMH), “strong evidence may exist for genetic susceptibility, but no specific gene has been unambiguously identified for common forms of mental disorders,” and “the estimate of the influence of environmental factors on the disorder provides an index of how difficult the search will be.” (Source: NIH/NIMH Genetics and Mental Disorders: Report of the National Institute of Mental Health’s Genetics Workgroup – Mental Disorders and Genetics: What We Know Today) That was in 1997! A similar paper to this one published in The Lancet in 2013 addressed these same five psychiatric disorders correlating some genetic components to a region on Chromosome 3 against almost 30,000 normal/wild-type patients. The NIH responded then saying that though there were significant correlations presented therein, there isn’t enough evidence to show the risk associated with the mutation and further research is necessary. Fast forward to some further research and we now see evidence of overlap between particular mental illnesses as well as cell-to-cell signaling as a specific neuropathological mechanism of disease. Is it enough for a Nobel Prize? No. But think of it somewhere between a paper titled “We’ve Discovered Insulin!” and “Patients with Diabetes Often Have Elevated Blood Glucose.”


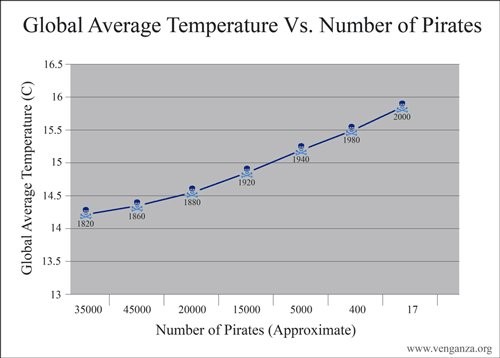
Correlation does NOT imply causation, but isn’t it so tempting!
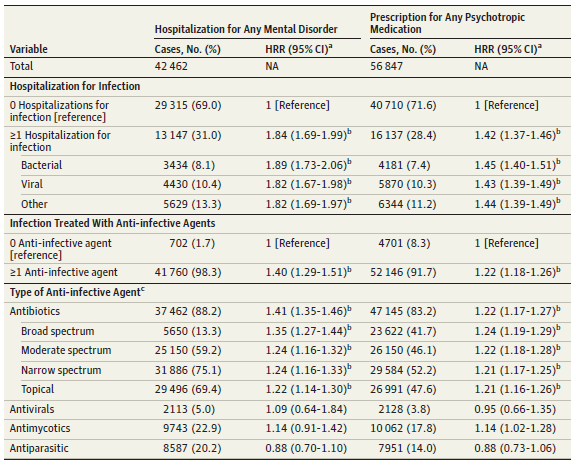
While promising articles like these offer amazing potential insights into a deeper understanding of clinical diagnostics for psychiatry, articles are as numerous and complex as patients. An article published this month from the Journal of the American Medical Association (JAMA) Psychiatry correlated an association between hospitalization and subsequent mental disorders in children. Anything that purports to associate new causality between disease entities and trends is always worth a read. And, like any other experienced clinician, you go straight to the title and design methods to determine your gut feeling about this paper before continuing. The title: “A Nationwide Study in Denmark of the Association between Treated Infections and the Subsequent Risk of Treated Mental Disorders in Children and Adolescents;” the number of patients studied: over 1 million. What? That’s amazing! 1 million cases, what amazing data, what amazing insights, what …a statistical nightmare. Finding results in a million is both exhaustively comprehensive and statistically problematic. Black holes are rare. But if you search the entire universe you’ll find millions. “With a large enough sample size, rare things become common…” this was said with a pregnant pause and the normal gravity delivered by astrophysicist Neil DeGrasse Tyson, PhD, during a live taping of Star Talk my wife and I attended a month ago.

What came up during that show was the same theme I’m discussing today: it’s very important to do research, collect data, and translate that data appropriately. Especially in medicine, where conclusions and results from research can affect patient outcomes, lab professionals like us need to be leaders.
Back to this paper, the authors report a strong significant correlation between hospitalization events requiring antibiotics and the prevalence of mental illness later in life. Analyzing the hazard risk ratio (HRR) for these patients reveals values usually over 1.0 which show that they are above the regular risk when compared to patients not under these conditions. The authors associate treated infections with childhood/adolescent mental disorders, but include a very important remark at the very end which is ever-present in most good research. They address the fact that results and conclusions from their data may be explained by other, non-studied causes directly because of otherwise not understood pathophysiology. And, like 99% of pathology reports I’ve seen end with a dogmatic “suggest clinical correlation,” this paper closes with something similar to “further research is needed.”
So that’s it! Using data is great! It’s the best. Translating direct and clinically relevant findings from the bench to the bedside is what we do best. Consulting with our clinical colleagues, those of us in laboratory medicine have a responsibility to make sure of four main things. First, we have to make sure that the results we obtain are clear. Pre-to-post analytical analysis is paramount to testing efficacy and we’re the experts on standard procedures and accountability. Second, the interpretation of results whether it comes from a research lab or hematology bench must be valid. Protocols and metrics are great, and using them to ensure effective use of information is critical. Third, the conclusions we reach should be meaningful. If it’s a cancer staging diagnosis biopsy report or a groundbreaking publication on shared genetic variants, the implications must provide the best information for patients. Because finally, we do what we do for them. Our work and efforts always go back to improving patient outcomes, and giving each person the best chance at maximum health and quality of life. Pathology and psychiatry might be worlds apart, but only in vocabulary at best. We’re on the same team. And, despite finding each other as great neighbors in most Medscape physician job reports, we both work very hard to lead the charge in protecting, healing, and advocating for our patients.

Thank you, and happy holidays!
