Case History
66 year old man with a past medical history of Sjogren syndrome, hypertension and hypothyroidism presented to an outside hospital with abdominal pain and diarrhea. CT imaging showed extensive lymphadenopathy, splenomegaly, mesenteric thickening and ureteral dilatation, all highly concerning for lymphoma or other malignancy. A needle core biopsy of “mesenteric mass” showed reactive lymphoplasmacytic infiltrate in a sclerotic background. A second needle core biopsy of a retroperitoneal lymph node was performed which showed reactive features and numerous plasma cells. An excisional biopsy of an inguinal lymph node was ultimately performed due to worsening lymphadenopathy with increased PET FDG avidity.
Excisional Biopsy




Diagnosis
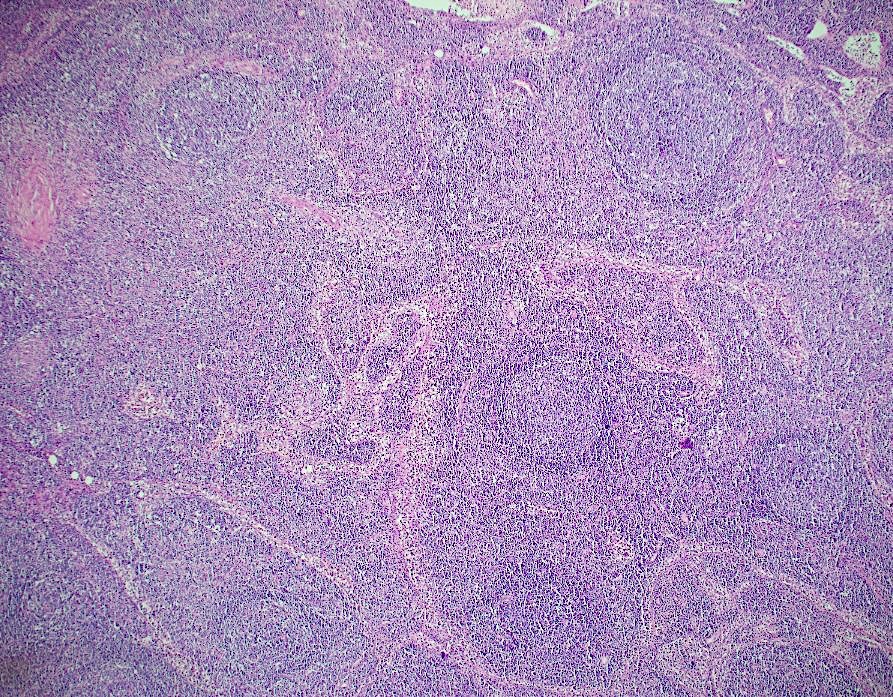
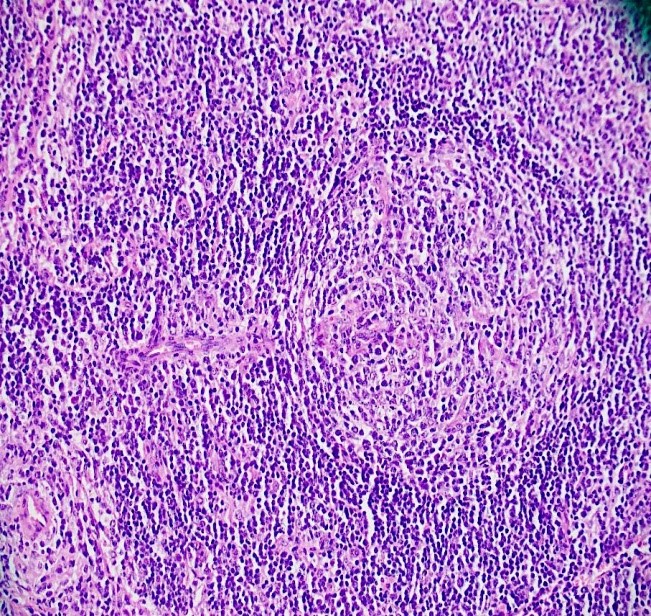
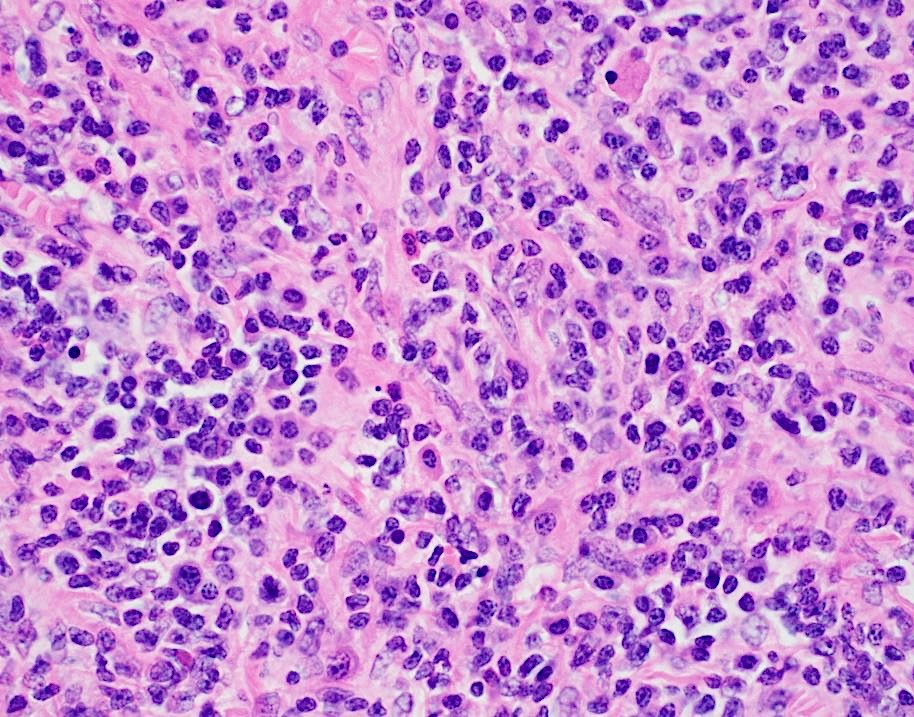
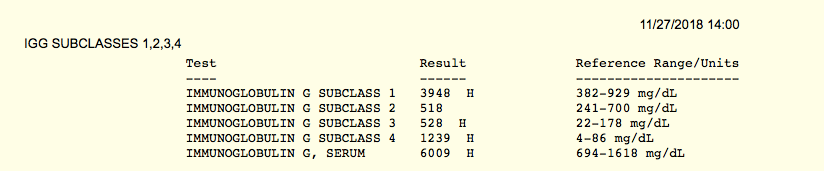
At low power view, there is intact follicular architecture with reactive appearing germinal centers that are polarized and show tingible body macrophages. The higher power view shows a feature that can be seen in Castleman disease called a “lollipop” which has a thickened vessel with hypertrophied endothelial cells penetrating the germinal center. In addition, there are areas with sclerotic remnants of germinal centers, a feature that can be seen in infection or other reactive conditions. Notably, the interfollicular space is expanded by numerous plasma cells and rare scattered eosinophils. Overall, the lymph node shows reactive follicular and paracortical hyperplasia. Stains for IgG and IgG4 showed an elevated IgG:IgG4 ratio with 54% of IgG plasma cells positive for IgG4. These findings raise the possibility of IgG4-related lymphadenopathy (IgG4LAD). In addition to histopathologic findings, the patient was tested for a serum IgG4 level, which is an important diagnostic criterion for the diagnosis of IgG4 disease. Seen above, serum testing on 10/25/18 showed a low/normal IgG subclass 4 of 17 mg/dl. After the excisional biopsy was performed, suspicion of involvement by IgG4-related disease increased. A sample was re-sent on 11/27/18 with instructions to perform serial dilutions in case of the prozone effect (see discussion below). The test came back with an elevated serum IgG subclass 4 of 1239 mg/dl, further supporting the diagnosis of IgG4-related disease.
Discussion
IgG4-related disease is a condition that was originally described in patients with autoimmune pancreatitis. These patients were found to have elevated serum IgG4 concentrations and have large numbers of IgG4-positive plasma cells. IgG4-related disease is now recognized as a fibroinflammatory condition and has been described in almost every organ system. Similar histopathological characteristics can be seen regardless of location and include tumefactive lesions, dense lymphoplasmacytic infiltrate, increased IgG4-positive plasma cells and storiform fibrosis.1
IgG4 normally accounts for less than 5% of the total IgG in healthy people and is the least abundant IgG subclass. IgG4 is also seen to be involved in other immune-mediated conditions such as pemphigus vulgaris, idiopathic membranous glomerulonephritis, and thrombotic thrombocytopenic purpura. The majority of patients with IgG4-related disease have elevated serum IgG4 concentrations, but 30% of patients may have normal IgG4 concentrations.1 When testing IgG4 serum levels, it is important to be aware of the prozone effect. This occurs when very high concentrations of the antibody that is being measured are present. This will prevent appropriate antibody-antigen binding and agglutination from occurring. This will result in a falsely low level of antibody being detected. In a report by Khosroshahi et. al., after identifying the prozone effect in one patient with IgG4-related disease, 38 patients who had previously been tested for serum IgG4 levels were re-tested. The prozone effect was found to affect 26% of patients with IgG4-related disease. The samples were re-tested with serial dilutions and the mean serum concentration rose from 26 mg/dl to 2,008 mg/dl. This could have a large impact on patient care, as elevated serum IgG4 concentrations are very important in making the diagnosis of IgG4-related disease. 2
IgG4-related lymphadenopathy (IgG4LAD) is somewhat distinct from tissue based IgG4-related disease and presents with solitary or multifocal lymph node enlargement. Lymph nodes are involved by a lymphoplasmacytic infiltrate with increased IgG4-positive plasma cells and tissue eosinophils and are not typically involved by storiform fibrosis. Five microscopic subtypes have been described and include multicentric Castleman disease-like changes, follicular hyperplasia, interfollicular lymphoplasmacytic proliferation, progressive transformation of germinal centers, and a variant with the formation of inflammatory pseudotumor-like lesions. The differential diagnosis of this entity is broad and purely reactive lymph nodes as well as multicentric Castleman disease (MCD), in particular needs to be ruled out. The presence of HHV8 infection and elevated IL-6 and CRP can favor MCD, while tissue eosinophilia favors IgG4LAD.3
The diagnostic criteria for the diagnosis of IgG4LAD includes lymph node involvement, a serum IgG4 level greater than 135 mg/dl, and histologic findings of lymphoplasmacytic infiltrates with either >10 IgG4-positive plasma cells per hpf or a ratio of IgG4-positive to IgG-positive plasma cells to be greater than 40%. As seen in this case, patients may undergo multiple biopsies, often with extensive work-ups before a diagnosis is made. Treatment depends on the organ involved and extent of damage/dysfunction. While some cases may only need clinical follow-up, others will require urgent aggressive treatment. Glucocorticoids are typically the first line of therapy and have been shown to be effective in a majority of patients with IgG4-related disease. 3
References
- Stone, J, Zen, Y, Deshpande, V. IgG4-Related Disease. N Engl J Med 2012; 366:359-551.
- Khoroshahi, A, Cheryk, LA, Carruthers, MN, et. al. Brief Report: spuriously low serum IgG4 concentrations caused by the prozone phenomenon in patients with IgG4-related disease. Arthritis Rheumatol 2014; 66(1):213-7.
- Wick, M, O’Malley, D. Lymphadenopathy associated with IgG4-related disease: Diagnosis and differential diagnosis. Seminars in Diagnostic Pathology 2018; 35(1)61-66.

–Chelsea Marcus, MD is a third year resident in anatomic and clinical pathology at Beth Israel Deaconess Medical Center in Boston, MA and will be starting her fellowship in Hematopathology at BIDMC in July. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
