Case History
A 14 year old Caucasian female was transferred to the pediatric emergency department from an outside hospital due to a 3 day history of abdominal pain. The pain was concentrated in the right lower quadrant and was accompanied by nausea and two episodes of vomiting. Her vital signs were normal and physical exam demonstrated tenderness and guarding upon palpation of the right lower quadrant of the abdomen. Her white blood cell count was elevated at 21.1 TH/cm2 and showed 91% neutrophils. Abdominal ultrasound was unremarkable and CT scan was inconclusive for appendicitis. The patient was taken to surgery for an exploratory laparotomy and her appendix was removed.
Laboratory Identification
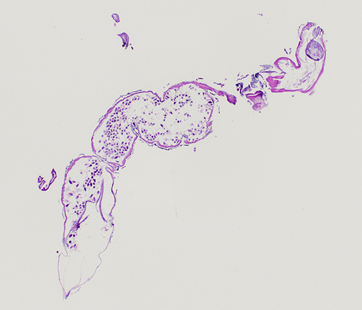
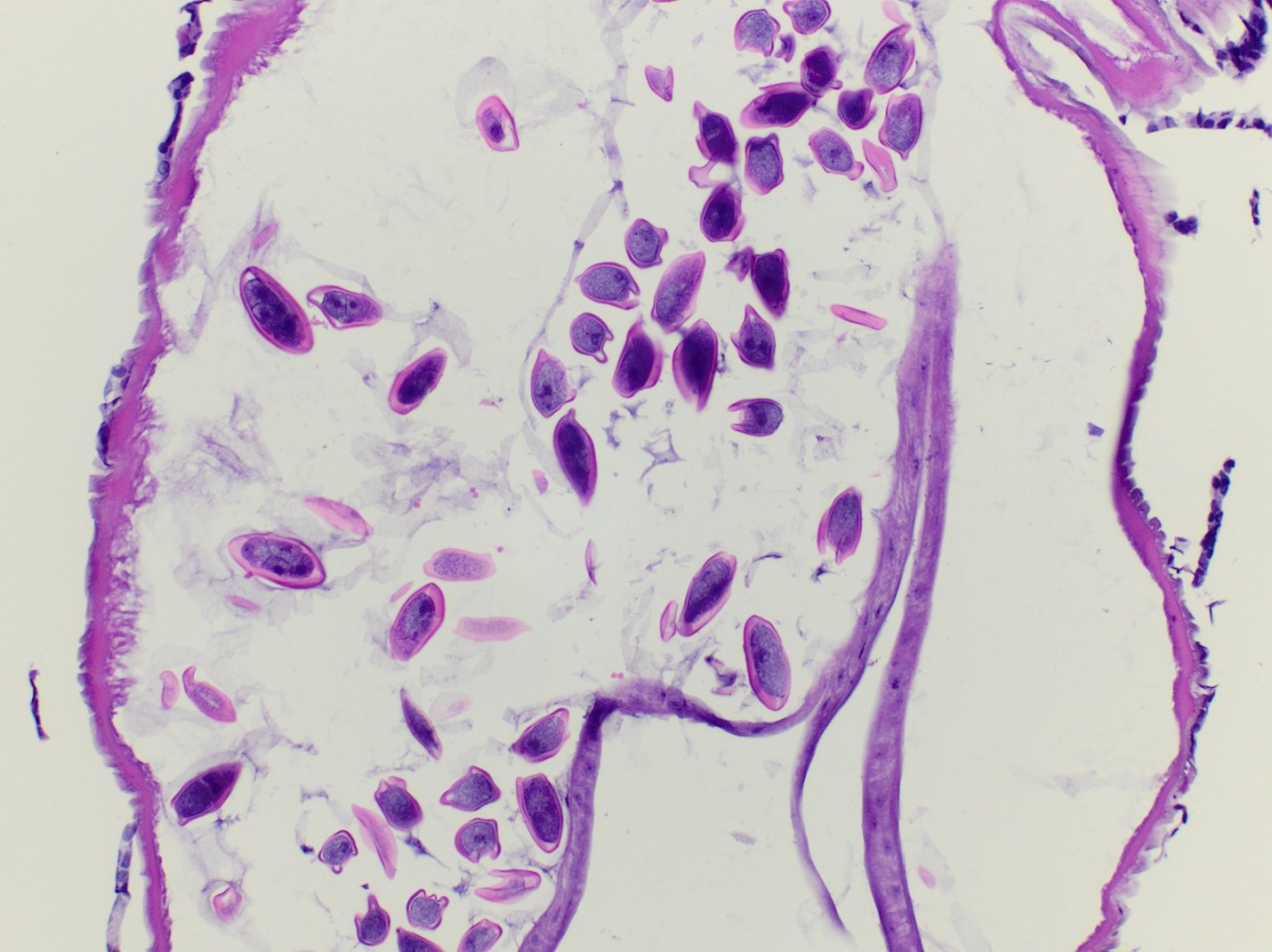
Gross examination of the appendectomy specimen showed an unremarkable appendix that measured 5.7 cm in length by 0.7 cm in diameter. There was no evidence of perforation. On sectioning, a small, white, “worm-like” structure (0.6 x 0.1 cm) was identified at the tip of the appendix and submitted for histologic examination. Microscopic review identified a female nematode with many eggs characteristic of Enterobius vermicularis. There was no acute inflammatory process identified upon microscopic review of the appendix.
Discussion
Enterobius vermicularis, commonly referred to as pinworm, is a nematode infection that frequently presents as perianal itching in young children or those living in crowded settings, with symptoms most prominent in the evening and night time. Adult female worms reside in the cecum of the large intestine and migrate to the perianal area during the night to lay eggs, resulting in irritation. Often, infections can be asymptomatic as well. E. vermicularis is one of the most common helminthic infections in the United States.
Humans are the only known host of E. vermicularis and become infected by ingesting embryonated eggs from feces or handling contaminated materials such as clothing, bed linens or from bathroom surfaces. Pinworm has a direct lifecycle and the larvae hatch in the small intestines and develop into adult worms that occupy the colon. It takes about one month from ingestion of infective eggs for E. vermicularis eggs then to be shed on the perianal folds.
Laboratory identification of E. vermicularis is usually made by using a piece of scotch tape or an adhesive paddle applied to the perianal skin in the morning and then visualizing the eggs microscopically. The eggs of pinworm are oval in shape & are flattened on one side with a thick capsule and measure between 50-60 x 20-30 um in size.On occasion, the eggs can be seen on pap smears as well. E. vermicularis worms can sometimes be visualized during colonoscopy, gastrointestinal & pelvic surgeries, and are capable of being identified by histology. Histologic sections of adult E. vermicularis worms usually show prominent lateral alae on the outer surface, testis or ovaries depending on the sex of the worm, and the intestinal tract. In gravid female worms, the characteristic eggs are numerous and can be helpful in the identification.
Treatment options of an E. vermicularis infection include an initial dose of albendazole, mebendazole,or pyrantel pamoate followed by a second dose two weeks later to prevent possible reinfection. Family members and other close contacts may be treated as well ensure eradication. In the case of our patient, her post-surgical course was uneventful and her white blood cell count trended down to 7.0 TH/cm2 after surgery. She was discharged home the following day.

-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the Director of Clinical Pathology as well as the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement, and resident education.

Ivermectin 200 micrograms per Kg of body weight for adults is also included in the pharmacotherapy of E. vermicularis.
It acts by selectively binding to glutamate-gated chloride ion channels of nerves and muscles of parasites causing hyperpolarisation of cells due to heavy influx of chloride ions of cells and death.