Case History
60 year old man with recurrent bronchitis and extensive smoking history underwent CT scan. The CT scan showed an incidental finding of a 2.2 x 1.4 cm anterior mediastinal mass.
Excision




Diagnosis
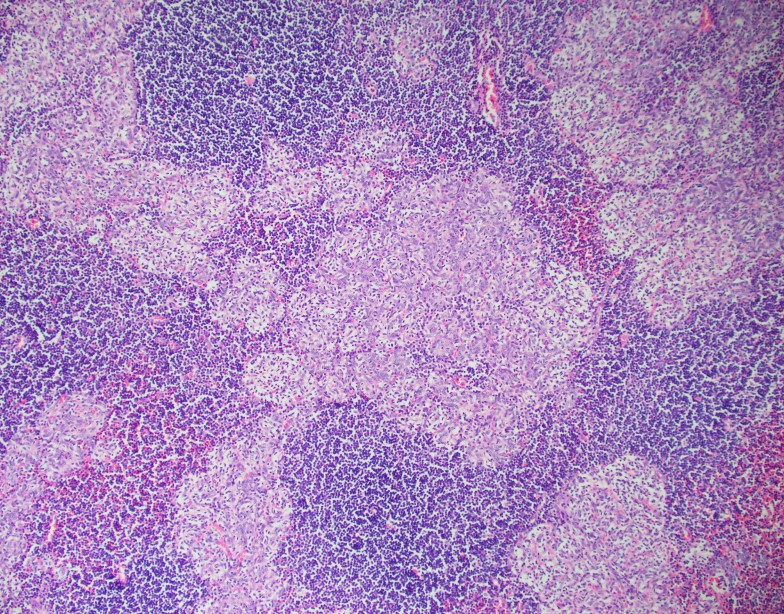
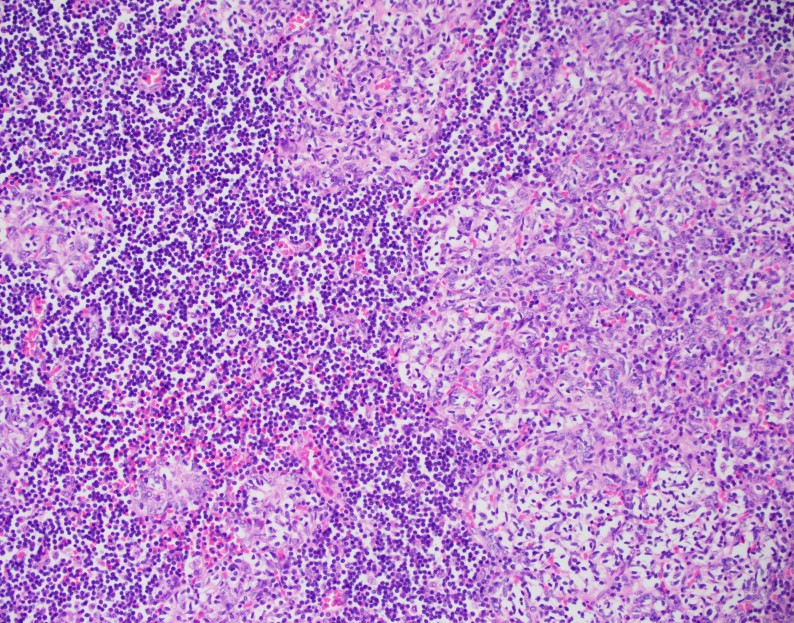
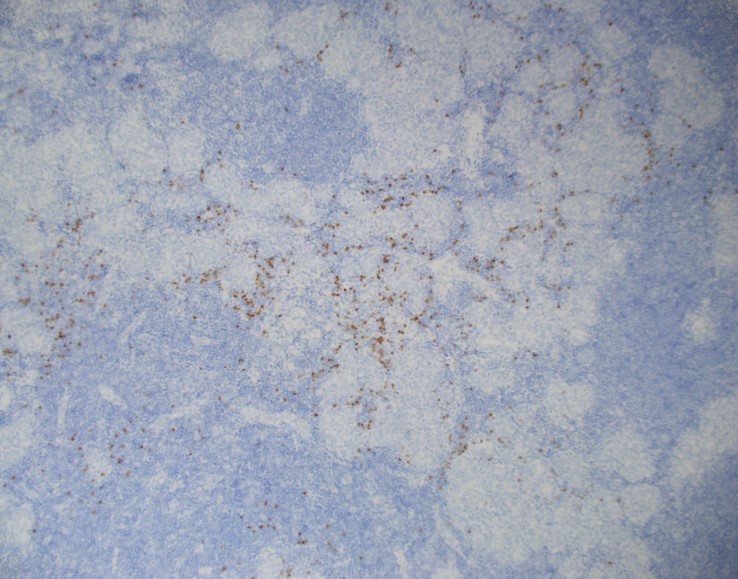
The tissue shows nodules of epithelial cells in a lymphocyte-rich background. The epithelial cells have round to somewhat spindle shaped nuclei, vesicular chromatin and small mostly inconspicuous nucleoli. There is no high grade cytologic atypia, mitotic figures or necrosis seen. The nodules contain very few interspersed lymphocytes, but are surrounded by abundant lymphocytes which are small and mature appearing. A cytokeratin cocktail highlights the epithelial nodules and shows an absence of epithelial cells in the lymphocyte-rich areas. CD20 highlights stromal B-lymphocytes around the epithelial nodules which are arranged in follicles. CD3 highlights stromal T-lymphocytes, which surround the B-cell follicles and the epithelial nodules. TdT highlights only a very small subset of immature T-cells which are found scattered around the rim of the epithelial cell nodules. Overall, the findings are consistent with a micronodular thymoma with lymphoid stroma.
Discussion
The differential diagnosis for an anterior mediastinal mass includes thymoma, lymphoma, germ cell tumors, neurogenic tumors and benign cysts among other less common entities. Patients usually present with cough, chest pain, fever/chills or dyspnea and localizing symptoms are generally secondary to local tumor invasion. Typically, CT scans are the best modality to evaluate the mediastinum. Thymomas are the most common primary neoplasm of the anterior mediastinum, but are less than 1% of all adult malignancies. Patients are generally over 40 years old and between 30-50% of patients with a thymoma have myasthenia gravis, which occurs more frequently in women.1
The WHO has classified thymomas into 5 categories based on the morphology of the neoplastic epithelial cells along with the lymphocyte to epithelial cell ratio. Type A thymomas are composed of bland spindle/oval tumor cells with few or no admixed immature lymphocytes. Type B1 thymoma resembles normal thymus and has scattered epithelial cells in a dense background of immature T-cells. Type B2 thymoma is composed of epithelial cells in small clusters with a lymphocyte-rich background. Type B3 thymoma is primarily composed of mild to moderately atypical epithelial tumor cells in a solid growth pattern with few intermingled immature T-cells. Type AB thymomas are composed of lymphocyte-poor spindle cell (Type A) components as well as lymphocyte-rich (Type B) components.2
Micronodular thymoma with lymphoid stroma (MTWLS) is a rare type of thymoma and accounts for only 1% of all cases. Patients tend to be asymptomatic and the finding is usually incidental. The tumor tends to be well circumscribed and encapsulated with a tan cut surface. The histopathology is characterized by solid nests or nodules of epithelial tumor cells in a background of abundant lymphoid stroma. The tumor cells are bland spindle or oval cells without significant atypia or mitotic activity. The epithelial tumor cells are positive for pancytokeratins. The lymphoid stroma typically lacks keratin positive cells and consists of predominantly CD20 positive mature B-cells in follicles with admixed CD3 positive and TdT negative mature T-cells. There is typically a population of rare TdT positive immature T-cells that surrounds the epithelial nodules, as seen in this case. 2
Due to the rarity of MTWLS with only 74 cases reported since the first case described in 1999, there is limited data on its pathophysiology and prognosis. However, most cases are diagnosed as stage I/II disease according to the Masaoka-Koga staging criteria, involving only micro or macroscopic invasion into thymic or surrounding fatty tissue without invasion into neighboring organs. Patients tend to have a very favorable prognosis with most patients alive without recurrence or metastasis many years after diagnosis.3
References
- Juanpere S, Cañete N, Ortuño P, Martínez S, Sanchez G, Bernado L. A diagnostic approach to the mediastinal masses. Insights Imaging. 2012;4(1):29-52.
- Travis WD, Brambilla E, Burke AP, et al. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart (Revised 4th edition). IARC: Lyon 2015.
- Qu L, Xiong Y, Yao Q, Zhang B, Li T. Micronodular thymoma with lymphoid stroma: Two cases, one in a multilocular thymic cyst, and literature review. Thorac Cancer. 2017;8(6):734-740.

–Chelsea Marcus, MD is a Hematopathology Fellow at Beth Israel Deaconess Medical Center in Boston, MA. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
