Case History
A 65 year old Caucasian male presents with a skin lesion on his right shoulder. Physical examination reveals a 3 .0 cm × 1.5 cm hyperpigmented plaque with mild hyperkeratosis on his right shoulder and multiple scattered erythematous macules and plaques on the trunk and back Skin biopsy reveals involvement by Blastic Plasmacytoid Dendritic Cell Neoplasm (BPDCN). PET scan reveals no extracutaneous involvement.
The patient undergoes CHOP chemotherapy followed by autologous hematopoietic stem cell transplantation. He is subsequently treated systemically with lanolidomide, venetoclax, and idelalisib due to relapses of disease.
The patient returns to clinic three years later for follow-up. While his original cutaneous lesions are completely resolved, new lesions are noted on his back (representative lesion, Image 1). Hematologic evaluation is remarkable for pancytopenia with hemoglobin 8.7gm/dL, white blood cells 1.4 K/uL, and platelets 39 K/uL. A biopsy of the bone marrow is performed.

Biopsy Findings

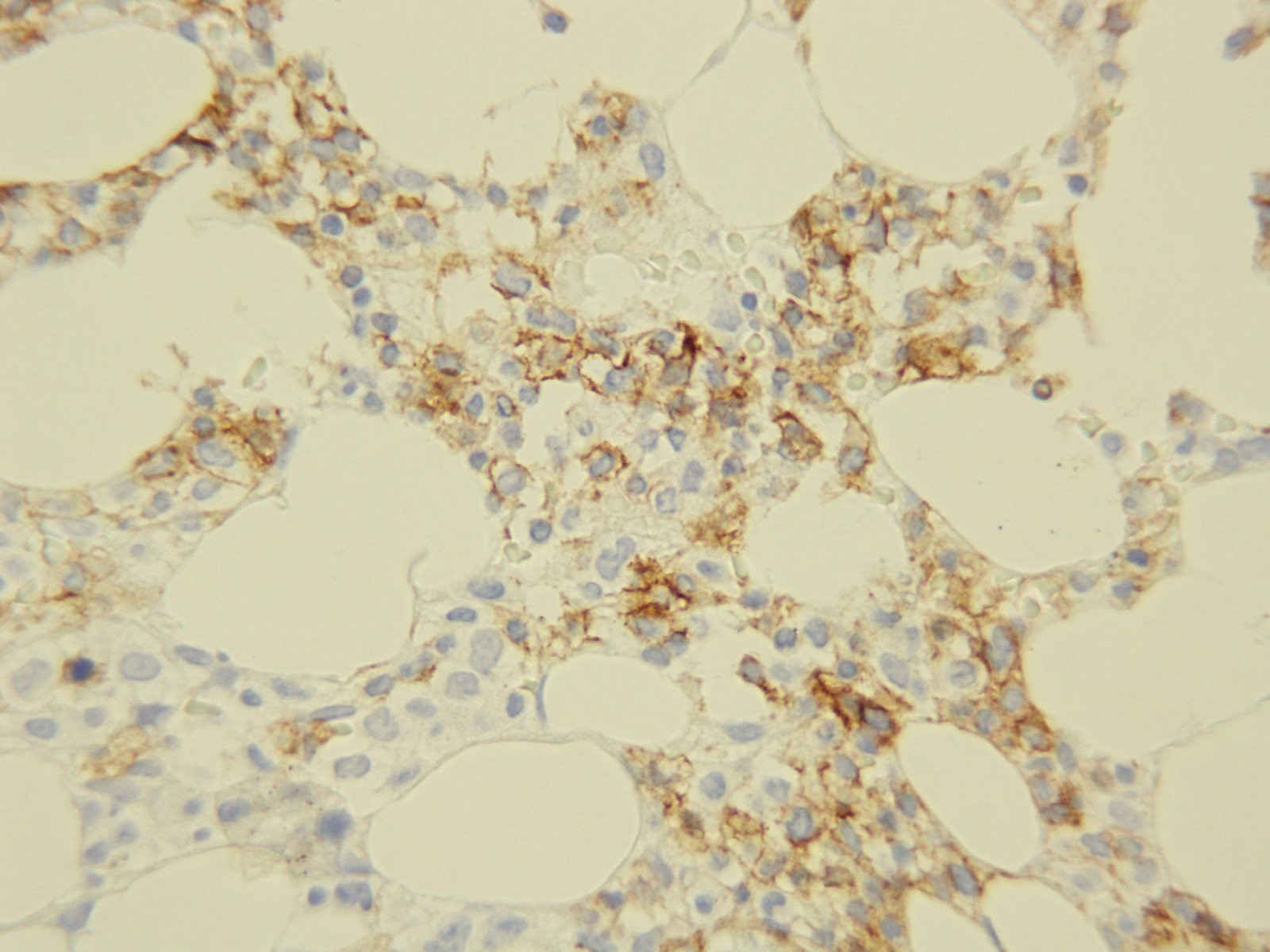
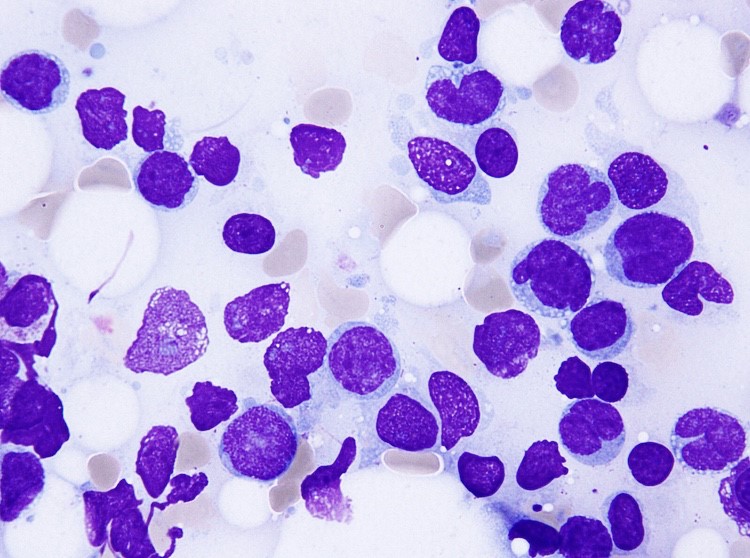
H&E stained sections demonstrate a normocellular bone marrow with diminished trilineage hematopoiesis and sheets of amphophilic, blastoid cells with irregular borders occupying most of the marrow cells. Immunohistochemistry demonstrates a cellular population with CD56. The aspirate smears show similar findings with numerous clustered blastoid cells (92%) with a monocytoid appearance, often with basophilic vacuolated cytoplasm. There is also a decrease in myeloid and erythroid precursors.
Flow cytometric analysis performed on the bone marrow aspirate reveals a dim CD45 population with expression of CD4, CD56, partial CD7, dim and partial CD5, and CD38. The same population lacks expression of immaturity markers such as CD34, MPO, and TdT. The morphologic and phenotypic findings found in the marrow specimen are diagnostic of extensive involvement of the marrow by BPDCN.
Discussion
BPDCN is a rare and highly aggressive malignancy derived from precursors of plasmacytoid dendritic cells. Its nomenclature has constantly changed over years as the understanding of this entity has been improved. It has been variously known as blastic natural killer cell lymphoma/leukemia, agranular CD4+ natural killer cell leukemia, and CD4+CD56+haematodermic neoplasm. It is currently classified under acute myeloid leukemia and related precursor neoplasms in the most recent WHO classification of tumours of haematopoietic and lymphoid organs.
Limited data exist regarding the incidence of BPDCN; however, it is estimated to account for 0.7% of primary cutaneous skin lymphomas and 0.44% of all hematological malignancies. This hematodermic malignancy predominantly affects elderly male patients with mean age ranging from 60 to 70; however, a few cases have also been reported in childhood and infancy. As demonstrated in our case, the patients typically present with multiple violaceous skin lesions, which may be associate with erythema, hyperpigmentation, purpura, or ulceration. Extracutaneous involvement is reported to occur in the bone marrow, peripheral blood, and lymph nodes.
Diagnosis of BPDCN relies on histological and immunophenotypic findings. Histologically, BPDCN may show a monomorphic infiltrate of medium-sized immature blastoid cells with round nuclei, finely dispersed chromatin, and cytoplasmic vacuoles. They typically display immunophenotypic expression of markers CD4, CD56, CD123, and T-cell leukemia/lymphoma 1 (TCL1) without any lineage-specific markers of T cells or B cells. Chromosomal abnormalities involving 5q, 12p,13q, 6q, 15q, and 9p have been reported. The differential diagnosis entails, but is not limited to, mature T-cell lymphoma, nasal-type NK/T-cell lymphoma, myeloid sarcoma/acute myeloid leukemia and T-cell lymphoblastic lymphoma/leukemia
The clinical course of BPDCN is aggressive, with a median survival of 9 to 16 months. The patients with disease limited to the skin may have a better prognosis, while advanced age and advanced clinical stage are indicators of poor prognosis. There is currently no consensus on optimal management and treatment because of low incidence of BPDCN; however, most patients are treated with regimens used for other hematopoietic malignancies (i.e. CHOP and hyperCVAD) followed by allogeneic stem cell transplantation for eligible patients. They often respond well to chemotherapy with complete resolution of skin lesions; however, relapse of disease can occur due to resistance to chemotherapeutic agents, which may have happened in our case.
References
- Lim MS, Lemmert K, Enjeti A. Blastic plasmacytoid dendritic cell neoplasm (BPDCN): a rare entity. BMJ Case Rep. 2016;2016:bcr2015214093.
- Grushchak S, Joy C, Gray A, Opel D, Speiser J, Reserva, Tung R, Smith SE. Novel treatment of blastic plasmactoid dendritic cell neoplasm: a case report. Medicine (Baltimore). 2017 Dec;96(51):e9452.
- Dhariwal S, Gupta M. A case of blastic plasmacytoid dendritic cell neoplasm with unusual presentation. Turk J Haematol. 2018 Jul 24. doi: 10.4274/th.2018.0181.
- Shi Y, Wang E. Blastic plasmacytoid dendritic cell neoplasm: a clinicopathologic review. Arch Pathol Lab Med. 2014 Apr;138(4):564-9.
- Bulbul H, Ozsan N, Hekimgil M, Saydam G, Tobu M. Report on three patients with blastic plasmactoid dendritic cell neoplasm. Turk J Haematol. 2018 Sep;35(3):211-212.
- Kerr D 2nd, Sokol L. The advances in therapy of blastic plasmacytoid dendritic cell neoplasm. Expert Opin Investig Drugs. 2018 Sep;27(9):733-739.
- Pagano L, Valentini CG, Pulsoi A, Fisogni S, Carluccio P, Mannelli F, et al. Blastic plasmactoid dendritic cell neoplasm with leukemic presentation: an Italian multicenter study. Haematologic. 2013 Feb;98(2):239-246.

-Jasmine Saleh, MD MPH is a pathology resident at Loyola University Medical Center with an interest in dermatopathology and hematopathology. Follow Dr. Saleh on Twitter @JasmineSaleh.

-Kamran M. Mirza, MD PhD is an Assistant Professor of Pathology and Medical Director of Molecular Pathology at Loyola University Medical Center. He was a top 5 honoree in ASCP’s Forty Under 40 2017. Follow Dr. Mirza on twitter @kmirza.
