The patient is
a 77 year old woman who presented in late Jan 2019 with severe anemia. In Feb
2017 she was diagnosed with myelodysplastic syndrome with no evidence of
transformation to acute myelogenous leukemia. A bone marrow biopsy at the time showed
5-7% blasts in the bone marrow. She went through 5 rounds of chemotherapy with
Vidaza (azacytidine) over the
course of 9 months, with no significant response. She received one unit of RBCs with her 4th round of chemo and was
given Aranesp (darbepoetin alfa) injections for anemia support. Aranesp is a man-made erythropoiesis stimulating protein which
can be used to treat symptomatic anemia
associated with myelodysplastic syndromes (MDS). After the 5th cycle of chemo, because of the lack of
response, Vidaza was discontinued. Since then she has received several RBC transfusions to
treat anemia and the Aranesp injections have continued.
In Oct 2018,
the patient’s CBC showed leukocytosis, anemia, thrombocytopenia and
neutrophilia. See results below:
Patient results
10/2018 reference ranges
WBC 31.6
4.5-10.5 x 103/μL
RBC 3.0
3.7-5.3 x 106/μL
Hgb 7.0
12.0-15.5 g/dl
Hct 23.6
36.0-46.0 %
MCV 78.4
80-100 fl
Plt 82
150-450 x 103/μL
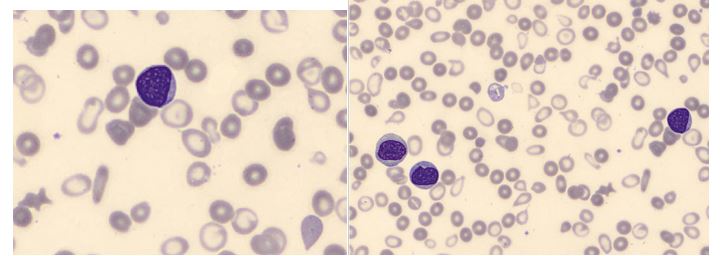
The CBC with automated differential performed at this visit flagged for a smear review. The technologist suspected blasts and the slide was sent for a pathologist’s review. The pathologist’s interpretation was that the differential showed “an aberrant myeloblast population, representing 6% of leukocytes along with an immature appearing monocytic population with phenotypic aberrancies representing 21% of leukocytes.” A leukemia/lymphoma flow cytometry was ordered. Results of the flow cytometry commented that an acute myeloid leukemia could not be excluded, however the differential diagnosis could also include chronic myelomonocytic leukemia.
By Jan 2018,
the patient was receiving blood transfusions every 6-8 weeks. CBC results from
this visit shown below:
Patient results
1/2019 reference ranges
WBC 36.5
4.5-10.5 x 103/μL
RBC 2.7
3.7-5.3 x 106/μL
Hgb 6.2
12.0-15.5 g/dL
Plt 65
150-450 x 103/μL
Unfortunately
the differential on this visit showed over 25% myeloblasts, confirmed by
pathologist’s review. This sample was sent out for a second leukemia/lymphoma
panel. A myeloblast phenotype was detected representing 27% of the leukocytes.
Diagnosis:
Acute monoblastic/monocytic leukemia, no remission.
Image 1. Blasts, RBC morphology consistent with severe anemia
Image 2. Blasts seen on slide.
Myelodysplastic
syndrome is a disorder of hematopoietic cell production involving clonal
proliferation of an abnormal hematopoietic stem cell. It is most commonly diagnosed in patients in their 70s. Failure
of the bone marrow to produce mature healthy cells is a gradual process, and
therefore MDS is not necessarily a terminal disease. However, pancytopenia is a
hallmark of MDS, and when pancytopenia is accompanied by the loss of the body’s
ability to fight infections and control bleeding, MDS can be fatal. In
addition, patients with MDS have a high risk of conversion to AML. About 30% of
patients diagnosed with MDS will progress to acute myeloid leukemia (AML).
This patient was exhibiting
pancytopenia, with accompanying anemia and infections, until her WBC began
climbing several months ago. This was accompanied by the left shift and blasts
seen on the peripheral smear, and prompted the flow cytometry studies.
Acute monoblastic/monocytic
leukemia is considered a type of acute myeloid leukemia. In order to fulfill
World Health Organization (WHO) criteria for AML-M5, a patient must have
greater than 20% blasts in the bone marrow, and of these, greater than 80% must
be of the monocytic lineage. AML-M5 can further be classified as M5a or M5b
depending on whether the monocytic cells are predominantly monoblasts (>80%)
or a mixture of monoblasts and promonocytes (<80% blasts).
The patient’s situation was discussed with the patient and her family. The patient chose more conservative and palliative treatment options over further chemotherapy.
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
There are several potential safety indicators that can be
used to help someone assess the effectiveness of a laboratory safety program. The
results of a properly performed safety audit can be one of those indicators,
and it can provide useful information to a lab safety professional whether he
or she is new to the role or has been there for years. You’ll note, however,
that the term “properly performed” was inserted, and that was no mistake. Safety
audits are performed in laboratories across the world, but in some of these locations
the environment remains very unsafe, and performing the audits hasn’t made any
difference. Mistakes can be made when performing a laboratory audit, and those
errors can lead to dangerous situations. While all audit errors need attention,
there are three that can cause the most damage to your lab.
Probably the most common safety audit gaffe is a practice
known as “pencil whipping.” This happens when someone quickly marks “yes” on
every single item of the safety checklist without really checking for
compliance. Pencil whipping occurs for many different reasons. The person
performing the audit may be in a hurry, they may feel like they have performed
the audit often and just know the answers, or they may just not care about the audit
results. Perhaps there is no lab leadership oversight as to how the audit is
performed, or maybe the person performing the audit doesn’t understand what the
checklist items mean. No matter the reason, this pencil whipping of answers is
dangerous. It provides false results, and it masks real safety issues in the
department that will likely not have resolution. In an environment where this
occurs, a preventable lab injury or exposure is likely to occur, and it could
have lasting or even career-altering repercussions for the victims.
Another safety inspection misstep occurs when the person
performing the audit begins going down the checklist with pre-conceived assumptions
or a specific focus in mind. Some auditors have their minds made up about a lab
safety culture before they start, and their version of what they see while
inspecting may be skewed. That may cause them to cite a lab falsely and without
enough investigation into a particular issue. Some inspectors might be so focused
on one thing- chemical labeling, for example – that they miss other obvious
safety issues such as trip hazards on the floor. This narrow focus or mindset
can limit the effectiveness of a safety audit as it can prevent the auditor
from noticing other real hazards in the laboratory.
The third safety audit blunder (and probably the one with the worst consequences) is a failure to follow up on the audit results. In a larger laboratory, a complete lab safety audit can take several hours. It may involve a procedure review, an employee file review, and a look through lab drawers and cabinets as well as a walk-through. However, even if all of the findings from that work is well-documented, it won’t mean anything if there is no follow-up. A failure to review and act upon audit results negates the entire process, no matter how well it was performed. Make sure your lab inspection method includes that final step – someone should review all results and ensure that any safety issues are addressed or resolved as soon as possible. A healthy lab safety cycle will include that review as well as repeat audits to make sure safety compliance is maintained on an on-going basis.
A properly performed audit can speak volumes about the overall lab safety program. If your audit form remains constant, it can be a good idea to train multiple people to perform the audit so the lab can be viewed with fresh eyes each time. Regardless of who performs the safety audit, make sure they refrain from pencil whipping, that their focus is not narrow, and that the person responsible handles the follow up of any safety issues discovered. By avoiding common audit blunders, a positive improvement of the lab safety culture can be assured.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years
experience as a certified medical technologist. Today he is the
Laboratory Safety Officer for Sentara Healthcare, a system of seven
hospitals and over 20 laboratories and draw sites in the Tidewater area
of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
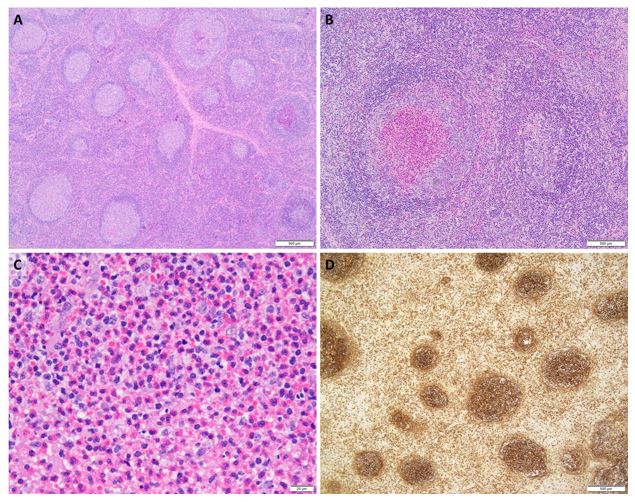
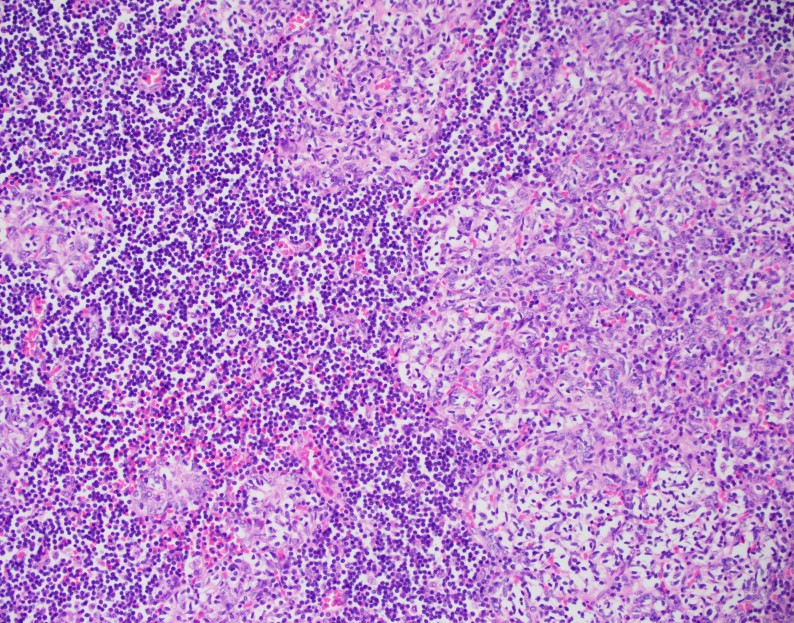
A 33 year old man of Japanese ethnicity presents with a 2 month history of a mass behind the right ear. Examination reveals a non-tender local with no other local or generalized adenopathy or hepatosplenomegaly. Laboratory investigations reveal an elevated ESR, serum IgE and peripheral blood eosinophilia. The lesion is excised.
Biopsy Findings
H&E stained sections
demonstrate a follicular hyperplasia. The germinal centers demonstrate polarity
and tingible body macrophages (A). Focally, follicular centers reveal
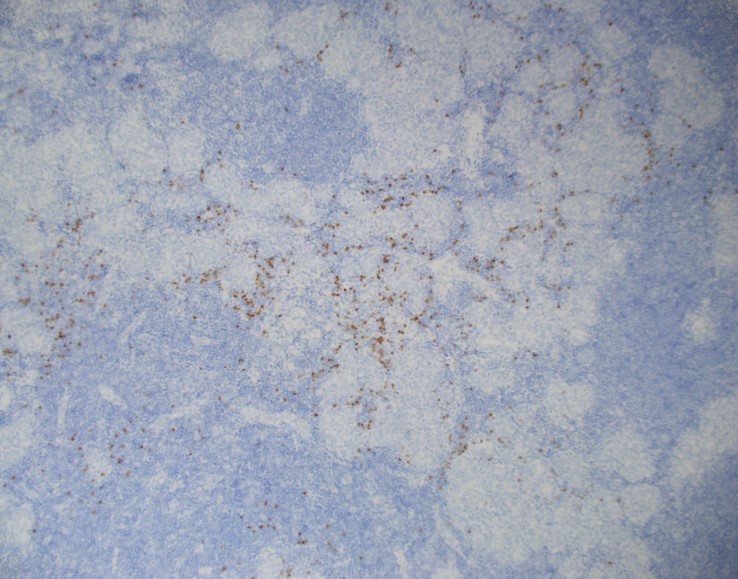
eosinophilic microabscesses (B, C). Immunohistochemical analysis with an IgE
stain reveals deposition in germinal centers (D). A diagnosis of Kimura disease
is rendered.
Discussion
Kimura
disease, also known as eosinophilic lymphoid follicular hyperplasia is a rare,
chronic inflammatory disorder of unknown etiology. While an infectious etiology
has been suggested, no pathogen has been identified to be causal, to date.
Historically, Kimura disease was considered to be the same as Angiolymphoid Hyperplasia
with Eosinophilia (ALHE); however, these entities are not the same.
Generally
occurring in Asian males, Kimura disease is most common in the 3rd decade of
life and in a head/neck site. It presents as painless, slow-growing adenopathy.
An association with nephrotic syndrome has been reported. Peripheral blood
eosinophilia, elevated ESR, and serum IgE are common findings. Histologically,
nodes reveal hyperplastic follicles with well-formed germinal centers and
mantle zones with deposition of IgE and eosinophilic microabscesses, as seen in
this case. Perinodal soft tissue may be involved. Necrosis may be present, but
is not extensive. Cytologically, FNA material may reveal polymorphous cell
population with many eosinophils.
Prognosis is
indolent; however, most cases recur after excision and radiation therapy
usually yields best outcome.
References:
Zhou P. et al. Kimura disease. Dermatol Online J. 2017 Oct 15;23(10).
García Carretero R et al. Eosinophilia and multiple lymphadenopathy: Kimura disease, a rare, but benign condition. BMJ Case Rep. 2016 Aug 31;2016. pii: bcr2015214211. doi: 10.1136/bcr-2015-214211.
Sun QF et al. Kimura disease: review of the literature. Intern Med J 2008;38:668–72.
–Kamran M. Mirza, MD, PhD, MLS(ASCP)CM is an Assistant Professor of Pathology and Medical Education at Loyola University Health System. A past top 5 honoree in ASCP’s Forty Under 40, Dr. Mirza was named to The Pathologist’s Power List of 2018. Follow him on twitter @kmirza
For transgender women, taking pills of estradiol is
insufficient to counteract the endogenous levels of testosterone produced by
their bodies. To counteract the undesired testosterone, anti-androgens are
employed. These include cyproterone acetate (approved only in Europe) or
spironolactone. Spironolactone is a potassium sparing diuretic that could have
unintended consequences like gynecomastia.1 This effect comes from
off-target binding of spironolactone to the androgen receptor. Like the
intended spironolactone target (mineralocorticoid receptor), the androgen receptor
localizes to the nucleus when activated and acts as a transcription factor.
Taking daily high doses of spironolactone
(100mg- 300mg daily) has been shown to be safe,1 but can increase
Potassium levels. In a cohort of 55 transgender women, potassium was actually
not higher (Figure 1).2 This was the first time a study had
rigorously measured electrolytes like potassium in transgender patients.
Current guidelines recommended checking electrolyte levels in transgender women
taking spironolactone.3 Full electrolytes were included for 126 TW
in our study and what we found was not what we were expecting.4
Figure 1.
We found no increased potassium levels in TW who had taken
hormone therapy for at least 6 months (p>0.05). However, we did see a
decrease in sodium which is consistent with the diuretic effect (p<0.0001, Figure
2).
Figure 2.
We wondered if variability in spironolactone dosing could explain why no significant potassium change was found. Luckily, we had a large number of patients who were taking various doses of spironolactone for comparison. One-way ANOVA with Tukey post-hoc tests revealed no difference in potassium levels (p>0.05)- even between the lowest (0mg daily) and highest dose (200-300 mg daily) (Figure 3). While the sodium level trended to decrease with higher spironolactone, it was not statistically significant.
Figure 3.
One reason that potassium levels did not increase is a
difference in study populations. The original population studied for
spironolactone involved patients with heart failure and hypertension whereas
our study’s population was mostly in their 20’s and 30’s with very few
co-morbid conditions.
Although sodium levels are decreased, they did not fall
below the lower limit of normal (135 mmol/L). Low sodium would put transgender
women at risk of dizziness and syncope (passing out) from low blood pressure.
Thus, the takeaway is: sodium should be clinically monitored as it can decrease
in transgender women.
References
Clark E. Spironolactone Therapy and
Gynecomastia. JAMA. 1965;193(2):163-164.
Roberts
TK et al. Interpreting Laboratory
Results in Transgender Patients on Hormone Therapy. The American Journal of Medicine. 2014; 127(2): 159-162.
Hembree WC, Cohen-Kettenis PT,
Gooren L, Hannema SE, Meyer WJ, Murad MH, et al. Endocrine Treatment of
Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society* Clinical
Practice Guideline. J Clin Endocrinol
Metab. 2017
SoRelle
JA, Jiao R, Gao E et al. Impact of Hormone Therapy on Laboratory Values in
Transgender Patients. Clin Chem.
2019; 65(1): 170-179.
-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and advancing quality in molecular diagnostics.
Anti-nuclear
antibody (ANA) test is commonly used to screen for systemic rheumatic disease. Indirect
immunofluorescence assay using HEp-2 cells as substrate, containing
approximately 100-150 autoantigens, is still the gold standard for ANA testing
(1). Although the test name refers to only anti-nuclear antibody, there are
often cytoplasmic staining patterns overserved in this assay. Cytoplasmic
patterns result from antibodies against cytoplasmic components, like Jo-1 or
Ribosomal P, and have clinical association with various systemic autoimmune
disease, like polymyositis, systemic lupus erythematosus or primary biliary
cirrhosis.
There is no
standardized recommendation regarding how to report cytoplasmic pattern on ANA
IFA, and laboratories independently decides whether to indicate cytoplasmic
pattern in their result. The
International Consensus on ANA Patterns (ICAP) workshop discussed this topic in
2015 and proposed two approaches for reporting ANA cytoplasmic patterns (2).
Either to regard cytoplasmic pattern as positive or negative, both approaches
recommended to include a statement of cytoplasmic staining.
We
encountered cases in our laboratory in which reporting cytoplasmic staining had
significant clinical values, and our laboratory started to report cytoplasmic
staining as an additional comment in the test result a few years ago. Here is
one of these cases:
Case: 35 year old woman with a
history of hypertension complained about increasing muscle pain, weakness, and
swelling. She had difficulties to raise her arms and had multiple falls, and
was admitted to hospital three time for rhabdomyolysis. Her initial laboratory assessment
were, CK >11,196 U/L, lactic acid 2.5 mmol/L, ALT 152 U/L, AST 416 U/L, and ALKP
42 U/L. Her ANA IFA test didn’t shown any nuclear staining, but there is very
strong cytoplasmic staining observed. The clinician was suspecting inflammatory
myositis and ordered myositis autoantibody panel to follow up. This panel detects
numerous antibodies that are either specific or associated with inflammatory
mycosis.
Her myositis autoantibody test result
was positive for antibodies against signal recognition particle (SRP). SRP is
an abundant, cytosolic, universally conserved ribonucleoprotein that targets
specific proteins to the endoplasmic reticulum in eukaryotes and the plasma
membrane in prokaryotes. Antibodies against SRP have been found in 5-8% of
adult idiopathic inflammatory myopathies and <1% juvenile myopathies. It is
closely associated with necrotizing myositis. Clinically it presents with acute
onset, rapidly progressive, severe weakness, with high CK levels and commonly
has cardiac and lung involvement.
Clinically
significant antibodies can be present in patients with connective tissue
disease that may appear as strong cytoplasmic staining on screening ANA test.
It would be helpful to add a comment in these cases to aid the clinician in
pursuing further work-up with a strong clinical suspicious of connective tissue
disease.
References:
1. Position Statement: Methodology of
Testing for Antinuclear. Antibodies American College of Rheumatology. 2009.
2. Damoiseaux
J, et al. International consensus on ANA patterns (ICAP): the bumpy road
towards a consensus on reporting ANA results. Auto
Immun Highlights. 2016 Dec;7(1):1. doi: 10.1007/s13317-016-0075-0. Epub
2016 Jan 30.
-Xin Yi, PhD, DABCC, FACB, is a board-certified clinical chemist,
currently serving as the Co-director of Clinical Chemistry at Houston
Methodist Hospital in Houston, TX and an Assistant Professor of Clinical
Pathology and Laboratory Medicine at Weill Cornell Medical College.
Last month, I discussed some really interesting topics at
the intersection between psychiatry and pathology—two
fields that aren’t exactly the closest; more so “diverged” in the hospital
milieu as if in a poem by Robert Frost. This month I’d like to bring the
conversation back to a topic I’ve addressed before: improving multidisciplinary
medicine and creating a Just Culture in medicine.
Not exactly culture with a swab or agar dish, a Just Culture
is an all-encompassing term for system-based thinking and process improvement
not at the expense of individuals. In a post I made last
July, the topic of high reliability organizations (or HROs) is one
that addresses communication and accountability in high stakes
environments—like healthcare!
Just Culture isn’t a stranger to lab medicine. The American
Society of Clinical Laboratory Science (ASCLS) published a position paper in
2015 utilizing this trending healthcare buzzword. On the subject of patient
safety, ASCLS believes “Medical Laboratory Professionals must adopt a ‘fair and
just culture’ philosophy, recognizing that humans make errors, and
understanding the science of safety and error prevention.” (Source: ASCLS 2015,
https://www.ascls.org/position-papers/185-patient-safety-clinical-laboratory-science)
We all know how we maintain patient safety in the lab, right? We do that
through quality control, QA measures, competencies (both internal and from
accrediting bodies like CAP), and continuing education. Raise your hand if your
lab is getting inspected, just finished getting inspected, will be inspected
soon, or if you’ve recently done competency/proficiency testing yourself, CE
courses for credentialing, or are reading this blog right now! We’re all
“continuing” our education in health care ad
infinitum because that’s how it works—we keep learning, adjusting, and
ensuring best practices concurrent with the latest knowledge. And, instead of
punishing lab professionals when we make errors, we try to be transparent so
that each error is a learning opportunity moving forward.
Image 1. I’d panic too if my lab was being inspected by 007. What, you wouldn’t?
I’m currently in my OB/GYN rotation at Bronx-Care and during
the most recent Grand Rounds we had someone talk about “Just Culture”—a sort of
continuation on the themes of the same lecture series that inspired my article
on HROs. Essentially, the theme is that disciplining employees for violating
rules or causing error(s) in their work is less effective than counseling,
educating, and system-oriented and best-practice-informed care. In this talk,
we watched a short video (embedded below) which walked us through approaching
faults or errors in medicine in a way that empowers and educates. A story from
MedStar Health, a Maryland-based health system, demonstrates how systems-based
thinking can be the best way to solve problems in healthcare.
Video 1. “Annie’s Story” has become a widespread example of Just Culture for nearly twenty years. Being serious about high reliability and just culture means adopting a system’s approach to analyzing near misses and harm events—shame and discipline are becoming antiques. Learn more about Quality and Patient Safety (http://ow.ly/M1aZk) and Human Factors Engineering in Healthcare (http://MedicalHumanFactors.net)
Annie, a nurse in the MedStar Hospital system, is the
spotlight story in this video. She came across an error message on a glucometer
after checking someone who was acutely symptomatic. She double checked it and
made clinical decisions, with her providing team, to give insulin. This sent
the patient into a hypoglycemic event which required ICU support. In the story,
she was actually suspended and reprimanded for her “neglect”—other nurses made
the same error just days later. This prompted some action, inciting nursing
managers and other administrators to investigate further, ultimately involving
the biomedical engineers from the company to weigh in on this systemic fault in
glucose POCT. Annie returned to work, and the problem was recognized as not
user-error, but system error; she went on to talk about how she felt unsure of
her clinical competency after being reprimanded. Imagine if you accidentally
reported the presence of blast cells in a manual differential in a pediatric
CBC while you were alone on a night shift only to find out from the manager on
days that you made a pretty big mistake with clinical implications. Then
imagine you were suspended for a few weeks instead of simply asked to explain
and identify opportunities to increase your knowledge. Pretty harsh, right? I’m
glad the MLS who did that didn’t lose his job and only had to do a few more
competency trainings…yep.
Image 2 (a, b). Take a look at that glucometer. Would you have caught the error? Did you catch the “LO” value in the background vs. the out-of-range foreground prompt? Or was the screen prompt as distracting for you as it was for Annie? Who was responsible for this error: nurse, lab, or engineer?
Anyone else notice a stark absence of professional
laboratory input in the video? I assume many of you sharp-sighted lab
automation veterans didn’t miss the glaring “LO” behind the dialogue box on the
glucometer. And, to me, that begs the question: was there any lab input on this
instrument, its training, or its users? Nurse Annie made a mistake—but she’s
not alone, according
to a Joint Commission study from November last year, close to 11% of
users make mistakes when prompted with error messages compared to 0% of users
misinterpreting normal values on screens of a particular model of glucometer.
And that’s just one type of instrument. Imagine 1 in 10 nurses, medical
assistants, or patients misinterpreting their glucose readings. (Source: The
Joint Commission Journal on Quality and Patient Safety 2018; 44:683–694
Reducing Treatment Errors Through Point-of-Care Glucometer Configuration) This
should also be a good opportunity to remind us all of CLIA subpart
M, the law that outlines who can accredit, use, and report
point-of-care results. Herein lies another problem, stated well by the American
Association for Clinical Chemistry (AACC) in 2016, “… another criteria for
defining POCT—and possibly the most satisfactory definition from a regulatory
perspective—is who performs the test. If laboratory personnel perform a test,
then this test typically falls under the laboratory license, certificate, and
accreditation, even if it is performed outside of the physical laboratory
space, and regardless of whether the test is waived or nonwaived. On the other
hand, waived or nonwaived laboratory tests performed by non-laboratory
personnel are nearly always subject to a different set of regulatory and
accreditation standards, and these can neatly be grouped under the POCT
umbrella,” and that can mean trouble when we’re all trying to be on the same
clinical page.
In previous posts, I’ve mentioned
the excellent knowledge contained within the Lab Management University (LMU)
program. One of the modules I went through discussed this topic
exactly: Empowerment as a Function of
Leadership and Peak Performance. In short, if we want to be good leaders in
the lab, we have to set expectations for positive patient outcomes, including
safety. Good leadership should empower their staff with education, support, and
resources. Poor management can create toxic environments with staff that can be
prone to mistakes. If we can be dynamic leaders, who adapt to ever-improving
best practices and respond with understanding and compassion to mistakes, then
our colleagues become just as reliable as your favorite analyzer during that
CAP inspection I mentioned.
Image 3. LMU class module for promoting Just Culture and inciting positive behavior in your department.
I often get clinician input about how the processes between
the bedside and the lab can be improved. Often, they include comments about the
need to share relevant clinical data for improving diagnostic reporting or
improving a process between specimen collection and processing. But what often
gets left out is the human element: the scientist behind the microscope, the
manager behind the protocol, and the pathologist behind the official sign out
report. Let’s continue to incorporate all of the feedback our colleagues
provide while maintaining a safe and empowered culture for ourselves, our
staff, and our patients.
What do you think? How does your lab, hospital, clinic, etc.
address POCT safety or patient safety at large? Do you operate within a Just
Culture? Share and comment!
Thanks and see you next time!
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student actively involved in public health and laboratory medicine, conducting clinicals at Bronx-Care Hospital Center in New York City.
Baby Boomers were for a long time to largest working
generation in the workplace. They are slowly retiring and the next largest
generation, Generation Y, is becoming the largest. However, Baby Boomers’
impact on the workplace is still profound and most organizations, if not all,
are currently employing many Boomers. They are likely to be working in
leadership roles and exert influence on many policies, procedures, systems, and
organizational cultures.
Similar to Traditionalists, Baby boomers also appreciate
face-to-face meetings. However, their preference for leaving and receiving
voicemails is a lot higher than Traditionalists. They also appreciate social
media more, especially as their children and grandchildren are using it. Baby
Boomers utilize the internet more than Traditionalists and send text messages,
even if they still prefer to talk over the phone instead of texting.
Working with Baby Boomers is all about the relationship.
Establishing interpersonal connection should therefore be one of your main
priorities when collaborating with someone from this generation. Because of the
personal nature of their working style, it can sometimes take a few weeks (or
longer) for decisions to be made. Calculate that in when working on a proposal
or project. Baby Boomers appreciate formal presentations and a consensus-based
process.
A Baby Boomers’ approach to leadership centers on
incentives, data-driven decisions, and a democratic process. They typically are
open to input from peers and their leadership style is friendly. They value
receiving recognition, so any award or reward is appreciated and they will
often display them publically. Because of their focus on interpersonal
relationships, they do not respond to people who are not friendly and who
indicate their hierarchy. Instead, make sure that they feel you are listening
to them and including them. One way to do this is by taking notes and asking
follow up questions.
Baby Boomers’ professional dream is continuing to be useful
and productive in the workplace while feeling they are wanted and rewarded. If
you want to increase your working relationship with Baby Boomers, connect with
them on an interpersonal level by inviting them out to lunch and get to know
who they are outside of the workplace. Provide them with positive affirmations,
recognitions, and awards to make them feel they are a valued members of the
organization and that they input and work is essential to producing results.
Baby Boomers bring a lot of patients, experience, and knowledge and they help
create and foster a team environment when they feel they are contributing
members of the organization. Do not show impatience and question their ways of
doing things openly. If you do need them to change something, include them in
the process to make it a consensual and democratic process. Adding a Baby
Boomer to a team can greatly improve the outcomes and success of that team.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
I’d like to tell you a story that happened at the ASCP Annual
Meeting last October, 2018 in Baltimore.
Lotte Mulder and I presented a course on “Discovering Your
Diversity Strengths” to about fifty people. Lotte is a Millennial and I am a
Baby Boomer, and we’ve been working closely together for over three years on a
daily basis. The presentation went really well and the audience was very
participative and interactive. We talked about how different we were, how we
complimented each other, and the value of human diversity in the workplace.
At noon that day, we both participated in a Lunch Roundtable
where the topic was Diversity in the laboratory. We quickly learned that those
at our table had a strong interest and frustration about working with people
from different generations. The focus was primarily on Millennials and Boomers.
There were eight other people at our table and they each shared their
frustration about working in the lab with either older or younger people.
This was a real opportunity for us to share the generational strengths
and differences with each of these people. The Boomers seemed to think that the
Millennials didn’t have a good work ethic. The more I asked questions of those
in both generational groups, the more I was able to help them to share their
opinions and/or frustrations. Most importantly, I made a point of asking each
person what was important to them in the workplace.
The Millennials learned that the Boomers were “bred” to work
beyond the expectations of their job. Most importantly, they found their
identity in their work. This is one reason the “Boomer co-worker” delayed their
retirement because of the fear of losing their identity.
The Boomers learned that the Millennials had a very good work
ethic, they just valued work-life balance. It was actually Generation X that
introduced work life balance to the workplace and the Millennials bought into
the concept. The other strength of the Millennial is their passion for finding
a purpose in their job.
By the time our hour was up, you could see the difference in
how they related to each other. It’s amazing what education and awareness can
do for people.
As a final note, the next day we co-taught a course on Stress
Management. Wouldn’t you know it, we experienced the same situation at our
“Stress Management Roundtable” lunch! It was fun to see how people began to see
their co-workers through a different lens.
-Catherine Stakenas, MA, is the Senior Director of Organizational Leadership and Development and Performance Management at ASCP. She is certified in the use and interpretation of 28 self-assessment instruments and has designed and taught masters and doctoral level students.
60 year old man with recurrent bronchitis and extensive
smoking history underwent CT scan. The CT scan showed an incidental finding of
a 2.2 x 1.4 cm anterior mediastinal mass.
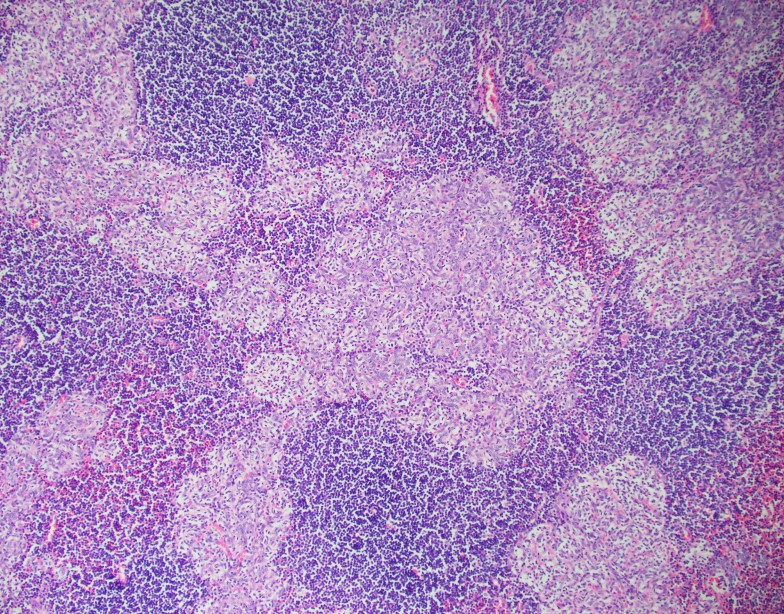
The tissue shows nodules of epithelial cells in a
lymphocyte-rich background. The epithelial cells have round to somewhat spindle
shaped nuclei, vesicular chromatin and small mostly inconspicuous nucleoli.
There is no high grade cytologic atypia, mitotic figures or necrosis seen. The
nodules contain very few interspersed lymphocytes, but are surrounded by
abundant lymphocytes which are small and mature appearing. A cytokeratin
cocktail highlights the epithelial nodules and shows an absence of epithelial
cells in the lymphocyte-rich areas. CD20 highlights stromal B-lymphocytes
around the epithelial nodules which are arranged in follicles. CD3 highlights
stromal T-lymphocytes, which surround the B-cell follicles and the epithelial
nodules. TdT highlights only a very small subset of immature T-cells which are
found scattered around the rim of the epithelial cell nodules. Overall, the
findings are consistent with a micronodular thymoma with lymphoid stroma.
Discussion
The differential diagnosis for an anterior mediastinal mass
includes thymoma, lymphoma, germ cell tumors, neurogenic tumors and benign
cysts among other less common entities. Patients usually present with cough,
chest pain, fever/chills or dyspnea and localizing symptoms are generally
secondary to local tumor invasion. Typically, CT scans are the best modality to
evaluate the mediastinum. Thymomas are the most common primary neoplasm of the
anterior mediastinum, but are less than 1% of all adult malignancies. Patients
are generally over 40 years old and between 30-50% of patients with a thymoma
have myasthenia gravis, which occurs more frequently in women.1
The WHO has classified thymomas into 5 categories based on
the morphology of the neoplastic epithelial cells along with the lymphocyte to
epithelial cell ratio. Type A thymomas are composed of bland spindle/oval tumor
cells with few or no admixed immature lymphocytes. Type B1 thymoma resembles
normal thymus and has scattered epithelial cells in a dense background of
immature T-cells. Type B2 thymoma is composed of epithelial cells in small
clusters with a lymphocyte-rich background. Type B3 thymoma is primarily
composed of mild to moderately atypical epithelial tumor cells in a solid
growth pattern with few intermingled immature T-cells. Type AB thymomas are
composed of lymphocyte-poor spindle cell (Type A) components as well as
lymphocyte-rich (Type B) components.2
Micronodular thymoma with lymphoid stroma (MTWLS) is a rare
type of thymoma and accounts for only 1% of all cases. Patients tend to be
asymptomatic and the finding is usually incidental. The tumor tends to be well
circumscribed and encapsulated with a tan cut surface. The histopathology is
characterized by solid nests or nodules of epithelial tumor cells in a
background of abundant lymphoid stroma. The tumor cells are bland spindle or
oval cells without significant atypia or mitotic activity. The epithelial tumor
cells are positive for pancytokeratins. The lymphoid stroma typically lacks
keratin positive cells and consists of predominantly CD20 positive mature
B-cells in follicles with admixed CD3 positive and TdT negative mature T-cells.
There is typically a population of rare TdT positive immature T-cells that
surrounds the epithelial nodules, as seen in this case. 2
Due to the rarity of MTWLS with only 74 cases reported since
the first case described in 1999, there is limited data on its pathophysiology
and prognosis. However, most cases are diagnosed as stage I/II disease
according to the Masaoka-Koga staging criteria, involving only micro or
macroscopic invasion into thymic or surrounding fatty tissue without invasion
into neighboring organs. Patients tend
to have a very favorable prognosis with most patients alive without recurrence or
metastasis many years after diagnosis.3
References
Juanpere S, Cañete N, Ortuño P, Martínez S,
Sanchez G, Bernado L. A diagnostic approach to the mediastinal masses. Insights
Imaging. 2012;4(1):29-52.
Travis WD, Brambilla E, Burke AP, et al. WHO
Classification of Tumours of the Lung, Pleura, Thymus and Heart (Revised 4th
edition). IARC: Lyon 2015.
Qu L, Xiong Y, Yao Q, Zhang B, Li T.
Micronodular thymoma with lymphoid stroma: Two cases, one in a multilocular
thymic cyst, and literature review. Thorac Cancer.
2017;8(6):734-740.
–Chelsea Marcus, MD is a Hematopathology Fellow at Beth Israel Deaconess Medical Center in Boston, MA. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
An 8-month-old female presented to the pediatric emergency department
(ED) due to vomiting and diarrhea for the past 10 days. Per mother, the baby has had a fever and 6-8
episodes of diarrhea & 2-3 episodes of vomiting each day. On the day of
admission, the mother noted the diarrhea was like mucous and contained blood
and the baby was unable to tolerate anything by mouth. Past medical history was
not significant and sick contacts included a sibling with a recent viral
illness. In the ED, the baby had a fever of 103.1°F and was tachycardic. On
physical exam, the baby was weak & lethargic with dry mucous membranes and
a capillary refill of 2-3 seconds. Mom noted the baby did not produce tears
when she cried and had decreased urinary output for the past 24 hours,
consistent with dehydration. Initial labs revealed an elevated white count of
20.0 TH/cm2 and a C-reactive protein of 6.60 mg/dL, suggestive of an
infectious process. Blood, urine, and stool cultures were sent to the
microbiology laboratory and the baby was received IV fluids and
ceftriaxone.
Laboratory Identification
Blood culture signaled positive after 36 hours of incubation on the
automated instrument and revealed gram negative rods.
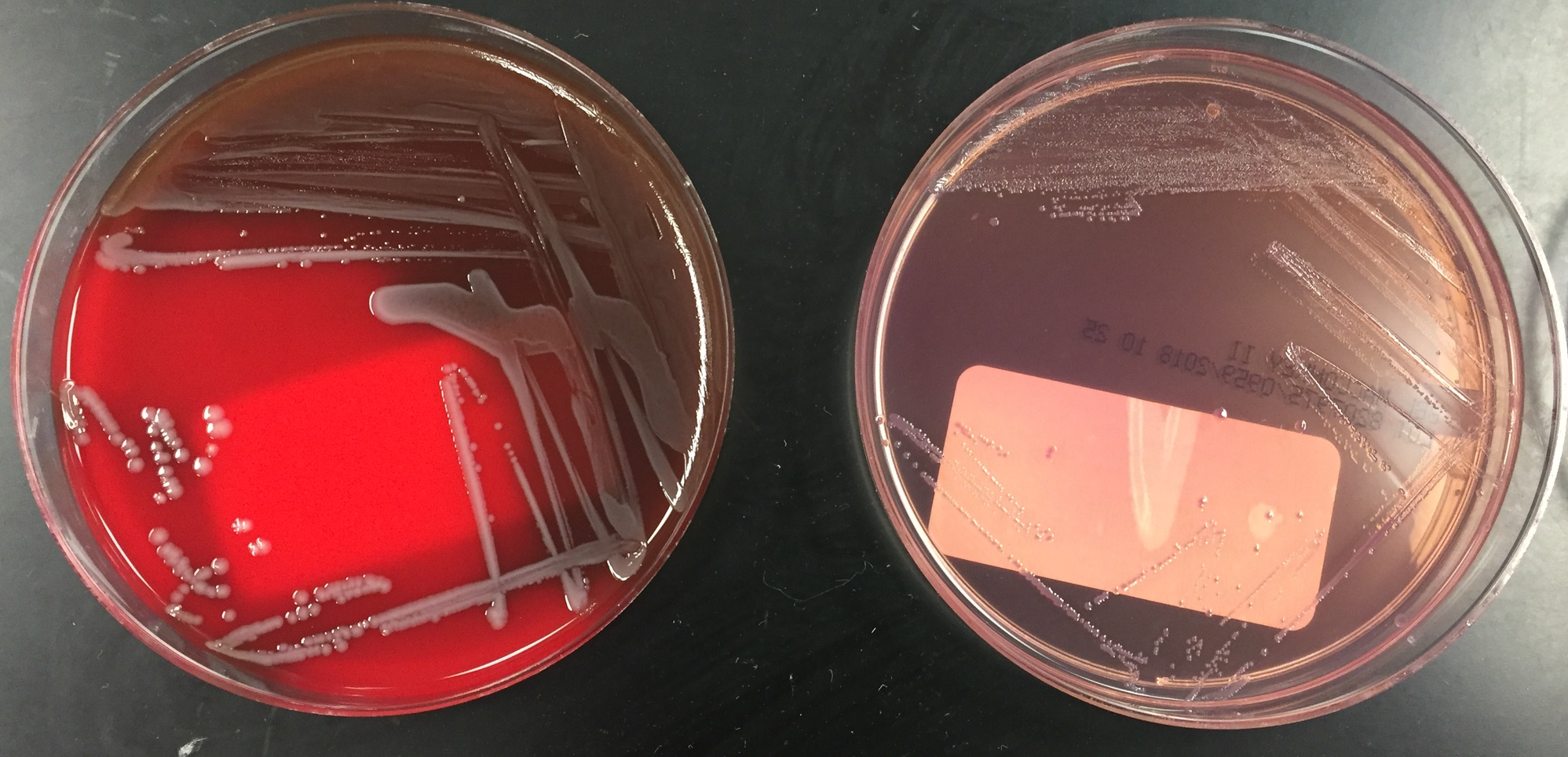
Image 1. Whitish gray colonies on sheep blood and MacConkey agars after 48 hours of incubation at 35°C in ambient air. Image 2. “Bull’s eye” colonies with a pink center and white outer edge on cefsulodin-Irgasan-novobiocin (CIN) agar after 48 hours of incubation at 22°C in ambient air.
MALDI-TOF mass spectrometry identified the isolate as Yersinia enterocolitica. The urinalysis
was positive and the urine culture grew >100,000 CFU/ml of Escherichia coli. Stool culture was
negative for Salmonella, Shigella, E. coli O157:H7, Aeromonas,
and Plesiomonas. Antigens for Shiga
toxin and Campylobacter jejuni were
both negative. Stool culture for Y.
enterocolitica was not ordered. A multiplex PCR panel for gastrointestinal
pathogens also identified Y.
enterocolitica.
Discussion
Yersinia enterocolitica is a
member of the Enterobactericeae
family and when transferred via the fecal oral route, can cause
gastroenteritis, terminal ileitis, and mesenteric lymphadenitis, particularly
in young children, the elderly, and immunocompromised patients, who consume raw
or undercooked pork, chitterlings, or drink unpasteurized milk products.
Because Y. enterocolitica can survive
and multiple at refrigerated temperatures, prepackaged lunchmeats and packed
red blood cells can be common sources for infection as well. Rarely, septicemia
can result from migration of the organisms into the lymph nodes and then the
blood.
Stool, blood, and lymph node cultures are often submitted to the
microbiology laboratory for the detection of Y. enterocolitica. The organism is a gram-negative rod that can
grow well on routine media such as sheep blood, chocolate, and MacConkey agars
at 22°C
and 35°C in ambient air. When there is a clinical concern for
gastroenteritis caused by Y.
enterocolitica, a selective media such as cefsulodin-Irgasan-novobiocin
(CIN) agar should be added to the stool culture to enhance isolation. Y. enterocolitica grows as “bull’s eye”
colonies with a pink center and surrounding clear to white border on CIN agar.
The organism ferments glucose & sucrose, is positive for catalase
& urease, and is oxidase negative. Y.
enterocolitica is able to be identified by manual and automated biochemical
systems, such as API 20E and Vitek as well as MALDI-TOF mass spectrometry.
Culture independent multiplex PCR panels for the diagnosis of gastrointestinal
syndromes are gaining popularity due to sensitivity & improved turnaround
times; however, reimbursement and the necessity for the isolated organism for
susceptibility testing and typing the in the case of outbreak investigations
continue to be items of concern.
The majority of cases of Y.
enterocolitica gastroenteritis do not require antimicrobial treatment. In
the case of severe disease and those that are immunocompromised or with
systemic disease should receive treatment with a fluorquinolone or trimethoprim
sulfamethoxazole. While Y. enterocolitica
produces beta lactamases, it is still uniformly susceptible to extended
spectrum cephalosporins as well.
In the case of our patient, she received 8 days of ceftriaxone and was
transitioned to oral trimethoprim sulfamethoxazole and discharged home to
finish the 21-day course of antibiotics due to bacteremia from Y. enterocolitica. Mother was counseled
to fully cook pork products before feeding to the baby.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the Director of Clinical Pathology as well as the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement, and resident education.
ASCP has led the way in bringing
pathology and laboratory medicine to the forefront of the discussion about
global health. Through their many international partnerships, they have been working
to bring high quality pathology services to patient populations in need worldwide.
In an effort to engage and enrich
the next generation of pathologists, ASCP created the Global Health Trainee
Fellowship in which those in a residency or fellowship (in the US or Canada)
have the opportunity to apply for a minimum of a four-week rotation at one of
ASCP’s global partner sites. This serves as an opportunity for trainees to gain
hands-on laboratory medicine experience in low resource settings and to broaden
their knowledge of pathology outside of the scope found in the typical western
demographic. As a recipient of the inaugural American Society of Clinical Pathology
Global Health Trainee Fellowship, I chose to go to Addis Ababa, Ethiopia for
the month of December 2018. I knew that laboratory services were actively advancing,
and I hoped that this would help me understand the challenges faced by an expanding
laboratory working with constrained resources. Ethiopian people are known to be
warm-natured, welcoming, and hospitable. Reputable also for their love of good
food and coffee (both of which are near and dear to my own heart!), I knew I
would be heading to a vibrant community of kindred spirits.
Ethiopia
Known as the birthplace of
humanity, Ethiopia is a country that is rich in culture, ancient traditions,
and beautiful scenery. In the last 100 years, Ethiopians have faced attempts at
invasion and occupation, severe famine, drought, ongoing water shortages, and
challenges most in the western world would never need to even think about. Despite
these challenges, Ethiopia has shown to be a resilient nation, constantly
moving forward, and is now considered to be the fastest growing economy in East
Africa.1
Ethiopia’s Cancer
Problem
Worldwide, cancer incidence is increasing each year. Developing
countries are no exception; not only do they bear the burden of communicable diseases;
they are also faced with an increase in non-communicable diseases, creating a
‘double burden of disease’. One estimate of the growing cancer epidemic in
Ethiopia demonstrated that death from cancer accounts for nearly 6% of total
national mortality with 80% of reported cases diagnosed at advanced stages.2 The Ethiopian Federal Ministry of Health has composed a
national cancer control plan to address the growing threat of cancer. In it,
issues such as lack of expertise on cancer diagnosis and treatment as well as
lack of diagnostic and treatment facilities are cited as major obstacles to
achieving cancer control. Addressing these factors is an enormous task, as
there are currently only approximately 40 pathologists in Ethiopia to serve a population
of over 100 million.3 Training enough pathologists in sub-Saharan Africa at the
current rate of matriculation is a major barrier to developing a rapid solution.
It is estimated that it would take over 400 years to match the number of pathologists
to the population to reflect the ratio found in the USA or UK.4 Therefore, those in higher resource settings have a unique
opportunity to help close this gap by joining in the effort to improve access
to pathology services.
My work with ASCP
in Ethiopia
In Ethiopia, ASCP has partnered with the two largest hospitals – Black Lion and St. Paul’s Hospital Millennial Medical College (SPHMMC). They are working to improve the quality management systems, introduce immunohistochemistry into the testing menu, and provide mentorship.
SPHMMC-Future Cardiac and Cancer Center
I had the privilege of spending a month with the remarkable
anatomic pathology team at St. Paul’s; here, there is an impressive staff of
pathologists, a residency program, a busy fine needle aspiration biopsy (FNAB) clinic,
and a histopathology laboratory. They average around 600 surgical specimens
monthly and perform between 40-50 fine needle aspiration biopsies daily. This
volume will only increase in the future, as a major cancer treatment center is
in construction now. I was fortunate to attend daily sign-outs where I saw
innumerable cases of tuberculosis- and HIV-related pathology, massive thyroid
goiters and malignancies, breast lesions that were sampled by both FNAB and
surgical methods, and a spectrum of tumors with the majority presenting in
advanced stage. I was so impressed by the diagnostic ability of both the
pathologists and the residents, and they were eager to share and teach the
cases that were rare to me. This was very valuable to me as a third-year
resident, as I do not see nearly as many infectious disease related specimens
and was exposed to an abundance of very advanced cases with unusual
presentations. In addition to these sign-outs, I had the opportunity to help
with frozen section diagnostics, which was quite challenging, but an extremely rewarding
experience.
One of my favorite experiences was working with the
talented and committed laboratory staff. I had the pleasure of working with
George Okbazgi, the anatomic laboratory manager, and Eshetu Lemme, the ASCP
local representative – both of whom are extremely passionate about quality
standards in the laboratory. We accomplished many things together, including
conducting a thorough mock inspection of the cytopathology department that
concluded with a detailed written report, and plan for improvements. We also
went through all the laboratory standard operating procedures as well as the AP
quality manual – we spent many hours going through these documents revising and
editing, identifying missing portions, and comparing to current laboratory
procedures. This was tedious work, but fortunately, we had an abundance of delicious
Ethiopian coffee to carry us through!
George Okbazgi and I discussing laboratory quality improvement plans (over coffee, of course!)
I reached out to the residents and attendings to see where
else I could be of use. I was excited that they asked for my help with editing
and revising several research reports, proposals, and grant applications. I was
delighted with this task because, in my residency, we’ve had ample opportunity
to participate in research and I’ve been fortunate enough to receive training
in manuscript writing. This was an area that the team at St. Paul’s felt that
they could improve, so it was a fantastic opportunity for me to be able to
share the benefits of my training.
I’m excited that my departure from the lab back to the US
did not mark the end of the relationship, as I was asked by the department to
be involved in their endeavor to develop a fellowship program in gynecologic
pathology – which will make this the first pathology fellowship program for the
nation! I am thrilled to be a partner in such a monumental venture and hope
that this will be the first of many long-term collaborative projects with the
wonderful pathology group at St. Paul’s.
The wonderful pathology team at St. Paul’s! (From left to right): Back Row: Drs. Addishiwot Tadesse; Aisha Jibril; Dawit Solomon; Eyerusalem Fekade; Amanuel Yeneneh. Middle Row: Drs. Eskindir Redwan; Nebiat Zerabruk; Melat Debebe; Hewan Hailemariam; Mersha Mekonnen; Menal Hassen. Front Row: Drs. Taye Jemberu; Dana Razzano; Samrawit Goshu; Abinet Admas. Pathologists and Residents missing from photo: Drs. Bereket Berhane (Chairperson); Mesfin Asefa (Program Director); Zewditu Chayalew; Selamawit Tadesse; Kirubel Girma; Tsion Betremariam; Zemen Asmare; Mahlet Guu’sh; Tadesse Musie; Azeb Gezahegn; and Ashenafi Getachew.
Conclusion
My time in Ethiopia was time truly
well spent – together, we were able to make significant gains in improving the
quality of the laboratory, engaging in research, and began laying the
foundation for future collaborations.
I highly encourage all residents
and fellows to apply to participate in this trainee fellowship with ASCP. It is
an invaluable opportunity to exchange knowledge, build new collegial
relationships, and help develop solutions to problems unique to these settings.
And for the pathologists out of training, ASCP offers many ways to get involved
in global health – please visit the ASCP Center for Global Health Website for
more information about the changes they are making worldwide and how you can
play a role: https://www.ascp.org/content/get-involved/center-for-global-health
Federal Ministry of Heatlh Ethiopia. National Cancer Control Plan of Ethiopia. 2015.
Adesina A, Chumba D, Nelson AM, et al. Improvement of pathology in sub-Saharan Africa. Lancet Oncol. 2013;14(4):e152-e157. doi:10.1016/S1470-2045(12)70598-3
Wilson ML, Fleming KA, Kuti MA, Looi LM, Lago N, Ru K. Access to pathology and laboratory medicine services: a crucial gap. The Lancet. 2018;391(10133):1927-1938.
-Dana Razzano, MD is a Chief Resident in her third year in anatomic and clinical pathology at New York Medical College at Westchester Medical Center and will be starting her fellowship in Cytopathology at Yale University in 2020. She was a top 5 honoree in ASCP’s Forty Under 40 2018 and was named to The Pathologist’s Power List of 2018. Follow Dr. Razzano on twitter @Dr_DR_Cells.