Case History
A 35 year old man presented to the Emergency Department (ED) with intermittent chest pain for 3-4 days, abdominal pain, fatigue, and lightheadedness over the same time period. Additionally, his family reported symptoms of progressive malaise for about a month, worse over the last week. In the ED, he was found to have ST elevations in the inferior leads of the electrocardiogram, which can be indicative of a heart attack. He was given 325 mg of aspirin and was emergently taken to the catheterization lab. He was found to have multiple complete occlusions in the distal left anterior descending artery (LAD), posterior descending artery (PDA), and posterior left ventricular artery (PLV). He underwent aspiration thrombectomy and the resulting clots were thought to be emboli; segments were sent to pathology for histopathologic evaluation and to microbiology for culture. There was no evidence of underlying plaque. He was admitted for management of ST-elevation myocardial infarction (STEMI). While in the ED, he was found to have white blood cell count of 23,000 and tachycardia to 110 beats per minute. A transthoracic echocardiogram demonstrated thickened aortic valve leaflets with evidence of leaflet destruction, severe aortic insufficiency, and right coronary cusp perforation which are consistent with endocarditis. Blood cultures were obtained and he was started on broad spectrum antibiotics (Vancomycin and Cefepime).
He has a past medical history significant for previous shoulder abscess with Methicillin-resistant Staphylococcus aureus (MRSA) and intravenous drug use (IVDU) (heroin, last use ~6 days prior to admission).
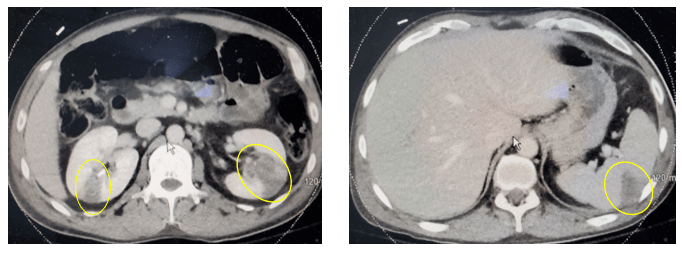
Computed tomography (CT) of his abdomen and pelvis revealed multiple renal infarctions and a splenic infarction (Image 1). In addition, the CT of the brain showed: “Multifocal scattered supratentorial and infratentorial subarachnoid hemorrhages and findings suggestive of evolving ischemic infarct involving the right inferior frontal gyrus, without evidence of hemorrhagic transformation currently. No midline shift or other complication identified.”
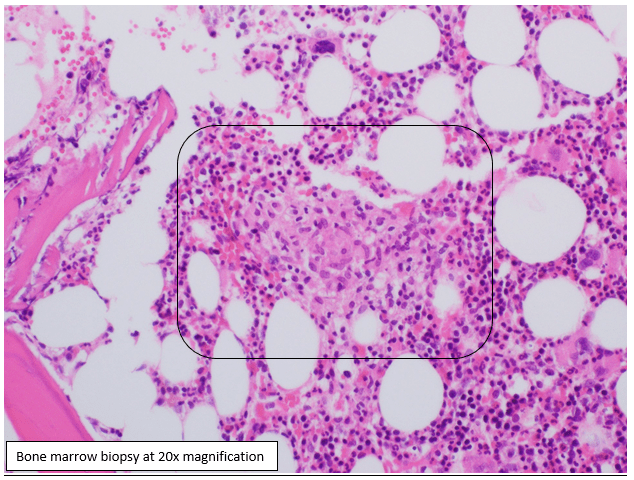
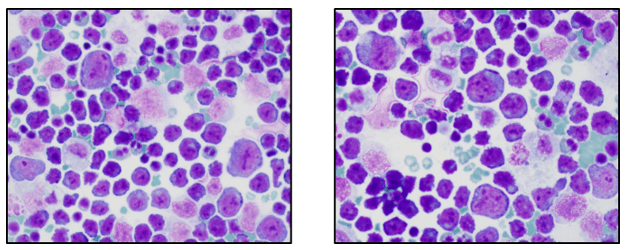
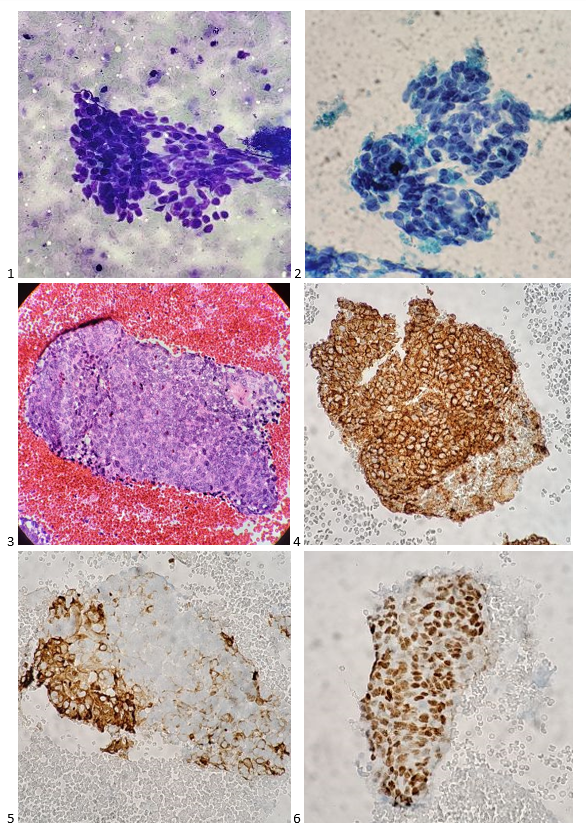
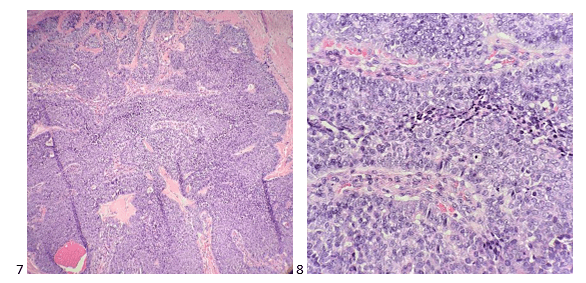
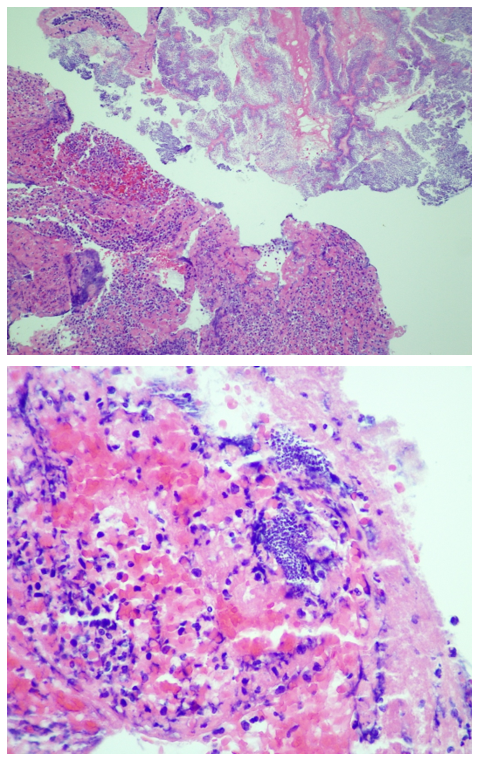
On hospital day 1 (HD1), both sets of initial blood cultures turned positive with gram positive cocci (GPC) in clusters and thrombectomy cultures were also growing GPC in clusters (Image 2). On HD2, the GPC in the thrombectomy culture was identified as Rothia mucilaginosa. GPC growing in the blood cultures were also Rothia mucilaginosa (Image 2). The patient was continued on Vancomycin. Repeat blood cultures were obtained after catheterization on HD0, and HD2, which were negative. On HD2, the pathology of the initial clots showed “fibrinopurulent debris and fibrin plaques with innumerable cocci in clusters” (Image 3).

On HD3, the patient developed 10/10 chest pain with troponin elevation and T-wave inversion. He was taken back to the catheterization lab for another procedure where he was found to have recurrent, complete occlusion of the PDA with unsuccessful recanalization due to the dense thrombus. On HD6, he developed tamponade physiology due to a large pericardial effusion that was drained. Cultures of the pericardial fluid were negative. Given the recurrent embolization events, the patient was transferred to another hospital to undergo aortic valve replacement surgery and coronary artery bypass graft surgery. Cultures taken at the time of the valve replacement surgery were negative and the valve tissue was not sent for pathologic evaluation.
Discussion
We present an uncommon case of extensive Rothia mucilaginosa sepsis with septic emboli and endocarditis. Rothia mucilaginosa has experienced the scientific name-change game over the last several decades. It was first identified as Micrococcus mucilaginosus, then became Stomatococcus mucilaginosus, was also known as Staphylococcus salivarius before finally arriving to today’s name of Rothia mucilaginosa.1,2 R. mucilaginosa is a normal inhabitant of the oropharynx and is often associated with dental caries.3 R. mucilaginosa can cause invasive infections, typically in patients with compromised immune systems, disrupted mucosal barriers or injection drug use.4
R. mucilaginosa is a facultatively anaerobic, gram positive, non-fastidious coccus that is coagulase negative but with variable catalase positivity. Colony morphology is usually white to gray nonhemolytic colonies with a mucoid appearance. Although the variable catalase reaction may point toward a Streptococcus spp., the Gram stain morphology of clusters helps to rule it out. Although not all strains are mucoid, the classic colony morphology is wet and is due to polysaccharide capsule.
The organism is generally susceptible to antibiotics designed to target gram positive bacteria including, penicillin, ampicillin, cefotaxime, rifampin and vancomycin.4 It is important to note that R. mucilaginosa is not predictably susceptible to clindamycin, trimethoprim-sulfamethoxazole or ciprofloxacin.5 The patient presented in this case received intravenous vancomycin in part due to the extensive disease on presentation, but also because he was at risk for methicillin-resistant Staphylococcus aureus (MRSA) sepsis and had a previously documented abscess from MRSA.
References
- Bergan T, Kocur M. 1982. Stomatococcus mucilaginosus gen. nov., sp.nov., ep. Rev., a member of the family Micrococcaceae. Int. J. Syst. Bacteriol. 32:374-377
- Collins MD, Hutson RA, Baverud V, Falsen E. 2000. Characterization of a Rothia-like organism from a mouse: description of Rothia nasimurium sp.nov. and reclassification of Stomatococcus mucilaginosus as Rothia mucilaginosa comb.nov. Int. J. Syst. Evol. Microbiol. 3:1247-1251.
- Trivedi MN, Malhotra P. Rothia prosthetic knee joint infection. 2015. J. Microbiol. Immunol. Infect. 48(4):453-455.
- Bruminhent J, Tokarczyk MJ, Jungkind D, DeSimone JA. Rothia mucilaginosa Prosthetic Device Infections: A Case of Prosthetic Valve Endocarditis. J. Clin. Microbiol. 5;15:1629-1632.
- Kaasch AJ, Saxler G, Seifert H. 2011. Septic arthritis due to Rothia mucilaginosa. Infection. 39:81-82.
-Doreen Palsgrove, MD is a board certified Anatomic and Clinical Pathologist who joined the faculty at UT Southwestern as an Assistant Professor in 2019. She specializes in head and neck and genitourinary pathology.
–Dominick Cavuoti, DO is a professor of AP and CP at UT Southwestern, specializing in infectious disease pathology, cytology and medical microbiology.

-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.