Case History An 83 year old male with bladder cancer was treated with Mycobacterium bovis Bacillus Calmette-Guérin (BCG), his last treatment occurring 1.5 months prior to presentation. He has a past medical history of chronic obstructive pulmonary disease, hypertension, obstructive sleep apnea, obesity, and diabetes. The patient has been hospitalized four times over the last two months and his symptoms include generalized weakness, malaise, shortness of breath and recurrent fever. He was found to have patchy lung infiltrates and he was diagnosed with pneumonia, COPD exacerbation and symptoms of heart filature. He was treated previously with antibiotics, steroids and fluid management which would temporarily relieve his symptoms. He presents to the hospital again, four days after his last hospital discharge, with generalized weakness, malaise, shortness of breath and recurrent fever. On initial evaluation he was found to be pancytopenic.

Laboratory Identification

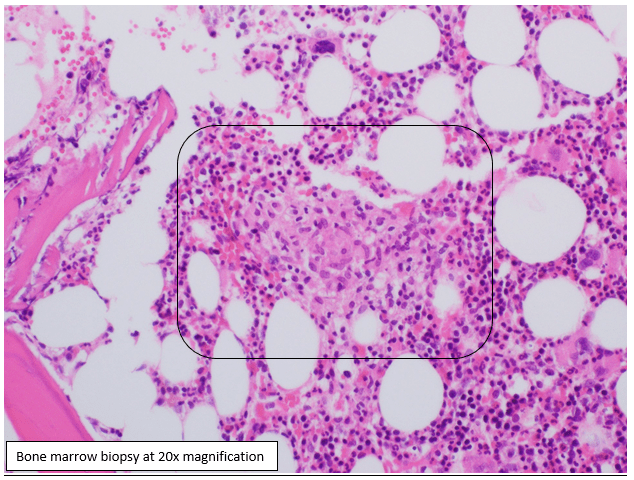
Blood cultures were negative. A bone marrow biopsy was performed for fever of unknown origin and pancytopenia. The biopsy showed non-caseating granulomas which were negative for acid-fast bacilli (AFB) by Ziehl-Neelsen stain and fungal elements by Gomori Methenamine Silver Stain (GMS). A laboratory-develped PCR test for Mycobacterium tuberculosis complex (MTBC) was performed on the bone marrow and was negative. AFB culture of bone marrow was positive for after 30 days of incubation and the organism was confirmed to be acid-fast bacilli by auramine-rhodamine fluorescent dye and Kinyoun stain. A second laboratory-developed test that uses heat shock protein (HSP) 2 and HSP3 to determine species level identification of Mycobacteria identified the organism as M. tuberculosis complex. Due to the patient’s history, further identification was performed at a reference lab using specific oligonucleotides targeting the gyrb DNA sequence polymorphisms which is able to separate different members of the MTBC. The patient’s isolate contained a RD1 deletion which is specific for Mycobacterium bovis bacillus Calmette-Guérin (BCG).
Discussion
Mycobacterium bovis is a slow growing mycobacterium which produces rough, dry colonies on growth solid media. It is one of the species in the MTBC with a natural host of domestic and wild animals. Routine molecular tests will not accurately differentiate between members of the MTBC. For definitive identification of M. bovis, 16S rRNA and gyrB gene sequencing is necessary. Safe handling procedures should be followed prior to molecular testing of MTBC.
Mycobacterium bovis BCG is a live, attenuated strain of Mycobacterium bovis that was created for vaccine and is used in the treatment of superficial bladder cancer. The treatment may cause localized symptoms including hematuria, fever, nausea, and dysuria which are marker of anti-tumor effect. Serious complications occur in <5% of patients with complications including sepsis, pneumonitis, hepatitis, lymphocytic meningitis, bone marrow involvement, and mycotic aneurysms. The cardinal sign of BCG infection is a relapsing fever with drenching night sweats persisting beyond 48 hours. Disseminated infection can occur days to years after the therapy. Clinical suspicion should be high for M. bovis BCG dissemination if there are symptoms and a high grade fever ≥72 hours. Treatment includes a regiment of isoniazid, rifampin and ethambutol. Most isolates of M. bovis are resistant to pyrazinamide.
References
- Lamm DL. Efficacy and safety of bacille Calmette-Guérin immunotherapy in superficial bladder cancer. Clin Infect Dis 2000; 31 Suppl 3:S86.
- Shelley MD, Court JB, Kynaston H, et al. Intravesical Bacillus Calmette-Guerin in Ta and T1 Bladder Cancer. Cochrane Database Syst Rev 2000; :CD001986.
- Richter E, Weizenegger M, Rusch-Gerdes S, Niemann S. Evaluation of Genotype MTBC Assay for Differentiation of Clinical Mycobacterium tuberculosis Complex Isolates. Journal of Clinical Microbiology 2003; 41(6): 2672-2675
- UpToDate
-Crystal Bockoven, MD is a 4th year anatomic pathology resident at University of Chicago (NorthShore). Crystal has an interest in and will be doing a fellowship in pediatric and perinatal pathology. In her spare time, she enjoys reading, hiking and biking.

-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.

I was aware of the use of BCG for TB prophylaxis but was unaware of its use for superficial bladder cancer. Very interesting!