Traditionalists make up the smallest percentage involved in the current workforce, but they are the organizational historians as they know and remember the organization’s past and founding goals. Traditionalists are typically born between 1927 and 1945 and grew up during the Great Depression, which was from 1933 to 1938. After that, the second World War started and the U.S.A got involved after the attack on Pearl Harbor in 1941.
These years had a significant effect on this generation. Traditionalists are known to work collaboratively, know how to do more with less, and are task-oriented. They typically have a strong sense of what is right and wrong, which was fueled by the historical events in their childhood and early adulthood. They have a strong sense of patriotism and respect for authority figures.
This generation is also one of the first major innovators; they created space travel, vaccination programs, and the foundation for modern-day technological innovations. They were the driving force of the civil rights movement of the 50s and 60s and were also the ones that started moving to suburbs. Currently, the are serving on many Board of Directors, as Presidents of organizations or as executive leaders. They have generally moved up in the hierarchy of organizations that they have spent years working for. They are loyal employees who require little feedback from their managers.
Because this is the era of pre-feminism women, the majority of women raised children and only had a job before marriage as teachers, nurses, or secretaries. This generation is self-disciplined, cautious, and self-sacrificing.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
This generation was born before 1945 and is the oldest generation in the American culture. However, not all of those born before 1945 are alike. They either fought in WWII or were children through those war years. The Traditionalist generation are really the first strong innovators and if they are still working they act as the historians of the organization because they have been there for a long time. They often serve on Board of Directors and are Presidents because of their organizational knowledge and expertise. They are typically very disciplined, consistent in their behavior and opinions, and are known for their loyalty.
The majority of Traditionalists are retirees and are the largest lobbyist group, which is the AARP. If your parents or grandparents were of the Traditionalist Generation, you might have experienced a “waste not, want not” attitude with strong family values, conformity, and team players.
The Traditionalists are often referred to as the “Silent Generation.” This term came from the fact that during this era, the children were often expected to be seen and not heard.
As I pondered this generational topic, I found myself searching for an example of an “Active Working Traditionalist” that I could talk about because they might not have yet retired! To my surprise I found myself thinking about my Uncle Tom. This man has taken care of me and his family of five children with my Aunt Pat my whole life. He is a strong family man and then realized he is still working! Uncle Tom (he prefers to remain nameless) turned 83 year’s old this past April 16th. He is still the principle owner of his own CPA firm and worked those long and hard CPA hours during this 2018 tax season. As I mentioned early in this blog, all Traditionalists are not alike, and Uncle Tom never expected children to be “silent.” He valued their opinions, and my Aunt Pat was both a stay home mom and a partner in their CPA firm.
Uncle Tom values the old-time morals of family first, safety, conservatism, patience and financial security. I encourage you to look around for your Traditionalist at home, or maybe even in the workplace. Let’s appreciate our Traditionalists while we still have the opportunity to learn from them!
-Catherine Stakenas, MA, is the Senior Director of Organizational Leadership and Development and Performance Management at ASCP. She is certified in the use and interpretation of 28 self-assessment instruments and has designed and taught masters and doctoral level students.
Hi everyone! Back with another piece about the life between the lab and medical school. This time, I’d like to take a minute to talk about some new and exciting developments in laboratory diagnostics happening right now: immunoassays for critical troponins are undergoing an evolution. Fourth generation testing is slowly developing into its fifth-generation upgrade. Labs across the country are starting to discuss the relatively new FDA approved fifth-gen cardiac troponin T assay which has been shown to be a high-sensitivity test. But what does this mean for labs? Specifically, what does it mean between the bench and the bedside? The hospital I’m currently on service at is rolling out the first beta-test of this assay in New York City right now, and as it turns out—it’s going to change a lot. Not only will the new understanding of cardiac enzyme reference ranges need a complete overhaul but tailoring appropriate clinical responses to those values will need to be looked at as well. I’m not a sales rep and this isn’t going to be an adventure in comparative statistical analytics, but I think it’s a great time to have a conversation early on about what these new generation assays could mean for us in the lab.
A Whole New World
When I was in graduate school, doing my MLS training we were taught the same cardiac enzyme assay history that was developed over the last 50 or so years. Early acute markers of inflammation relating to acute myocardial infarctions (AMIs) with respect to acute phase reactants AST, LDH, CRP, etc. As more technology advanced, specific biomarker analyses of individual detection of things like CK or myoglobin became useful. The WHO criteria for AMI then established (and re-established since the 1970s) the laboratory requirements for CK-MB and detectable levels of troponin to correlate with clinical findings. Further sensitivity and specificity developments, and clinical research like the GUSTO and APACE trials, showed us just how sensitive newer (then troponin T and I) cardiac assays could be. Not to mention, instead of rule-in/rule-out criteria, we had the development of risk stratification. And as instrumentation developed so did our testing—CK and LDH replaced with CK-MB and its isoforms, AST went the way of Myoglobin, and LD ratios became reliable troponins!
Table 1. In each stage of acute coronary syndrome (ACS) various biomarkers are available and detectable in peripheral blood. The challenge has been to find the most reliable and time-sensitive cardiac enzyme(s) to reflect appropriate staging and risk stratification. Research is helpful, but clinical intervention required critical timing.
Ask most clinicians today about cardiac enzyme, cardiac injury studies, or other related markers and you’ll hear about CPK, CK-MB 1, 2, 3 and other isoenzymes, LDH electrophoresis, and of course troponins T and I. What’s more is that the reference ranges for most of these tests haven’t really changed much either. If I called you and said your patient in 706-W has a Troponin of <0.03 you might be relieved for now. If I said that same patient’s troponin was 0.560—we might have a different story unfold. But what if I told you your patient’s troponin was 13, and was trending down from 15? What do you do with that? What if I only called to report a troponin-DELTA which was 0.0? Was there an in-service you missed? Possibly. Sounds like your institution might have 5th-gen on board.
What was wrong with the old troponin?
In a word: nothing, really. This really isn’t about buy-in for a “better” test or a better detection method. This is about creating a dialogue about improving risk stratification for our patients with coronary disease. Let’s go back to Chicago, specifically the last hospital I worked in before starting medical school: Swedish Covenant Hospital. Having been through a few hospitals in my time, I can say you’d be hard pressed to find a more streamlined, albeit small community hospital, laboratory service. Running a full gamut of SIEMENS instrumentation and critical middleware-software, the management there ran a tight ship—which included critical troponins. We ran the TnI-Ultra assay on the ADVIA Centaur/XP platform. It was your standard three-part immunoassay sandwich test with a biotin-streptavidin antigen-antibody detection. It was fast, used little reagents, was relatively stable, had a great system of QC, and was calculably-flexible between heparinized and ETDA plasma samples. Two-point calibration kept it tight between (and this is from memory, loosely) 0.006 and 0.50 ng/mL, and I believe we called our critical values at 0.40 ng/mL. This was a good test, and it’s used in many labs today still. It’s got great stability and has room to interpret ACS risk stratification based on population data in each location. People understand those results, too. But exactly how much room between, let’s say 0.10 ng/mL and >0.50 ng/mL, is there to stratify that risk? Complex decision algorithms then become hybrids of institutional cardiology recommendations, American College of Cardiology (ACC) recommendations, emergency department input, and, of course, laboratory management recommendations.
Here at Bronx Care Hospital Center (BCHC), I spoke with a laboratory manager about rolling out this brand new high-sensivity troponin (hs-cTn), and we discussed their vaildation and policies. Along with this new project, the hospital has been a vocal part of American College of Cardiology ACC17 Acute and Stable Ischemic Heart Disease program addressing topics including marijuana use and ACS, stable angina risk stratification, NSTEMI sex differences in revascularization and outcomes, treating cocaine related ACS with beta blockers, and research Anticoagulation Therapy After Anterior Wall ST-Elevation Myocardial Infraction in Preventing LV Thrombi. So, it seems fitting that this is as good as any a pilot location for cardiology departments city-wide to watch and learn from the hs-cTn roll-out!
Tell me more about this new test…
This hs-cTn assay is an electrochemiluminescence immunoassay (ECLIA) that uses two monoclonal antibodies against human cardiac troponin T. At this institution, they are using this immune sandwich assay on a Roche Cobas E with a similar biotin-streptavidin coated microparticle complex as with the previous generation testing. This is a short test with similar reagent use and stability as before, and only for lithium heparinized samples. With a relatively quick turn-around in less than 10 minutes, the new hs-cTn offers critical information for clinical correlations on the fly from potential STEMI codes coming into the ED.
Without going into horrific details about validating data on old and new troponins across patient populations, there is something interesting to note here which came up in discussion with the lab manager: new reference ranges. Now, with testing sensitivity, cross-reactivity, ranges, and interfering substances, the ranges are no longer the decimal-place values reported that we’re all used to. The ranges we work with now at BCHC are cutoff between <12 ng/L for positives and >52 ng/L for critical values suggestive of acute coronary syndrome. The analytical measuring range is much larger now between 6-10,000 ng/L. With the adjustments for limits of detection and blanks on instrumentation, the specificities of these values are normalized on a larger index for reflecting differences in male and female cardiac enzyme activity to a common cutoff of that <12 ng/L value. But more so than just a value, a new part of trending troponins becomes much more important: the delta values. These are more acutely indicative of the cardiac necrosis and/or condition of other non-specific heart tissue damage en vivo occurring in patients. Taking all this into account, you now have a much wider and broader range of values to interpret and incorporate into your clinical decision making, which brought up a few questions when I spoke with lab staff as well as cardiologists.
So, what’s wrong with the new troponin?
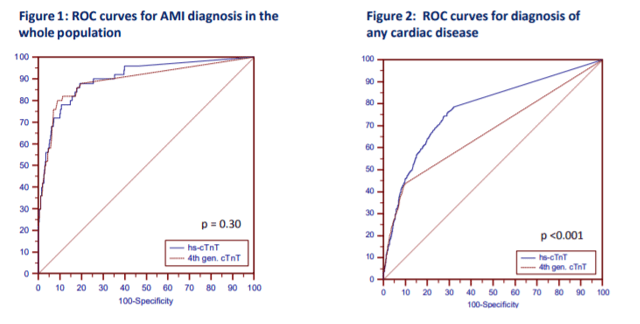
Okay, that’s a fair question at this point. And my answer is still: probably nothing. Sorry to be so inconclusive, but it’s still early days. There is a lot of data to support moving toward newer generation hs-cTn testing since it has been available outside of FDA-approval in Europe before January 2017. Research done in the Department of Internal Medicine and Central Institute for Medical Laboratory Diagnostics at Innsbruck Medical University in Austria show that new troponins might not be that different (read: better) than their 4th generation counterparts, at least with regard to emergency room visits. T. Ploner, et. al, argue that diagnosing AMI in the ED doesn’t really benefit from the heightened sensitivity offered by the new Roche 5th gen assay (Figure 1, Figure 1). But, when they compared the detection of other cardiac disease including AMI, unstable angina, heart failure, arrythmias, pulmonary emboli, pulmonary disease, anemia, renal disease, and several other entities, the 5th generation assay could more readily detect changes early and provide clinicians with critical data quickly (Figure 1, Figure 2).
Figure 1. Ploner et al. demonstrate here that there isn’t really any difference in the sensitivity of 4th generation vs. 5th generation troponins for detecting acute MI in the emergency room. However, there is a significant advantage in the detection of any cardiac disease, generally. (Source: Ploner et al. (2017) High-Sensitivity cardiac tropnonin assay is not superior to its previous 4th cTnT assay generation for the diagnosis of acute MI in a real-world emergency department, link: http://spo.escardio.org/eslides/view.aspx?eevtid=48&fp=P4177)
Finally, I think a review paper from the American Journal of Medicine last year summarized it best. Coming from the Department of Cardiovascular Diseases and Department of Laboratory Medicine and Pathology at Mayo Clinic in Rochester, MN, the authors discussed concern over the troubling over-sensitivity and potential pitfalls of reaching too far with hs-cTn testing. Their bottom line: collaborating on data and accuracy between cardiology, laboratory medicine, and emergency medicine, there is a great potential for this super sensitive test to provide clinicians with very useful data in the near future. We just have to process that data correctly. As always, results should be interpreted in conjunction with clinical presentation including medical history and laboratory data. But in the case of new and coming advances in critical care, there seem to be some common themes between my conversations here at BCHC and in what I read in the literature regarding how to ensure we move forward appropriately.
Multidisciplinary educational efforts are critical. The ER, the lab, and the cardiology department at each institution utilizing 5th gen troponins need to understand the new ranges, the new triaging cutoffs, the clinical correlations for consulting the ICU/CCU, and how to understand the deltas for their patient populations.
Create clear communications for your laboratory values. Will you normalize for gender or provide sex-specific confidence interval reporting? Will you provide tables for suggested value correlations with AMI/ACS protocols?
Order sets and in-service training. You’d be surprised how much the nitty gritty details of lab draws and ordering appropriate tests/tubes could slow down your institution’s advancement.
Figure 2. How the authors at Mayo Clinic establish the use of new hs-cTn assays in diagnosing and triaging potential AMI patients. (Source: Sandoval, Jaffe (2017) Using High-Sensitivity Cardiac Troponin T for Acute Cardiac Care, The American Journal of Medicine (2017) 130, 1358–1365, doi:10.1016/j.amjmed.2017.07.033)
At the very end of the day, it’s up to the institution. Clinical centers have to follow their own guidelines for cardiac pathology. ACC/ESC/AHA guidelines and Universal MI definitions are for clinical correlation across locations, but a single roll-out of a fancy new test can’t make a better ER. It really does take communication, collaboration, and accountability. We all have to push the envelope and practice at the top of our scopes in order to make health care better every day. One of the ways we might be able to do that now is by considering these new high-sensitivity troponins as a useful new clinical tool to improve patient outcomes.
Thanks for reading! See you next time!
Disclosure: I am no longer affiliated with Swedish Covenant Hospital in Chicago as an employee, and any recount of policy and/or procedure(s) specifically regarding their cardiology protocols and troponin resulting are a historical and anecdotal account of my time working there in the past. I have no affiliations with SIEMENS, Advia, Roche, or any other medical laboratory instrumentation institution. I am only affiliated with Bronx Care Hospital System as a current rotating medical student and my account of their transition to 5th gen testing is anecdotal from discussions with in-house staff, cardiologists, and laboratory management.
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student at the American University of the Caribbean and actively involved with local public health.
Last month we celebrated Lab Week, to recognize and show appreciation for Medical Laboratory Scientists and Technicians. Lab week is also a time to reminisce, and tell stories of the lab “in the old days.” I have worked with many technologists who have now been in the field for more than 50 years, and some who have worked in the same hospital all that time! Lab techs love to share stories about their experiences over the years, the days without computers, old methodologies, ancient lab equipment and manual testing. Listening to these stories always makes me think about just how far we have come in the field in the last 50- 60 years, and gives me a true appreciation for modern technology. It causes me to reflect on all the changes and developments that enable us to give physicians a wealth of knowledge that was previously unavailable.
During the first half of the 20th century, the complete blood count (CBC) was performed using exclusively manual techniques. Blood cell counts (erythrocytes, leukocytes, thrombocytes) were performed under the microscope using diluted blood samples and a hemocytometer. For each specimen, a technologist spent about 30 minutes at a microscope manually counting the cells and calculating the total count using a mathematical formula. A spectrophotometer was used to perform the hemoglobin by the cyanmethemoglobin method, and a spun hematocrit was performed. Indicies were calculated. A manual smear was made, stained, and cells were counted and differentiated under the microscope. To complete a CBC, all these procedures had to be performed individually, with duplicate testing and applying mathematical calculations, and could take over 2 hours. After all these tests were performed, results were reported on paper and sent to the patient’s doctor or the nursing floor.
In 1953 Wallace Coulter patented the Coulter Principle for counting and sizing microscopic particles. The Coulter Principle can be used for measuring any particles that can be suspended in an electrolyte solution, and has been used in the food and drug industry, in beer making, in the manufacture of construction materials and thousands of other applications. However, probably the most important application has been in the medical field where it has revolutionized the science of hematology. Coulter suspended red blood cells in a solution and, with an electrical current flowing, passed the solution through an aperture. As the cells pass through the current, the impedance between the terminals changes, and this change can be measured as a pulse. The first Coulter Counter measured the number of cells by counting the number of these pulses. The first Model A Coulter Counter was sold in 1956, manufactured in Coulter’s basement in Chicago. The Model A counted red blood cells in a sample in 10 minutes, a marked improvement over manual counting! The Coulter Counter was hailed for its speed, accuracy, and opportunities for reducing human error, tedium and eye strain.
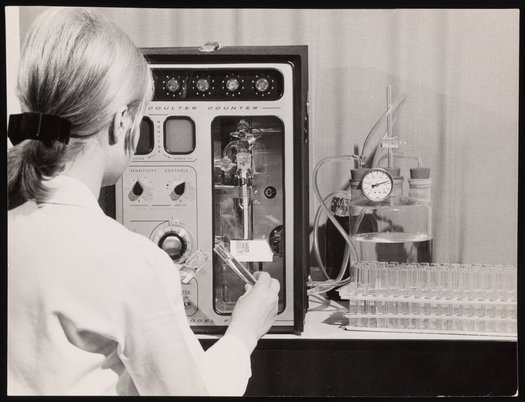
During the 1960’s, an improved Model B Coulter Counter was developed and Model A and Model B were used to count both leukocytes and erythrocytes. Other Coulter Counter models soon followed, and competitors entered the market with their versions of cell counters. Within a decade, nearly every hospital in the United States had a Coulter Counter, and the new, advanced Coulter Model F was widely used. In 1968 the first fully automated hematology analyzer, The Coulter Counter Model S was introduced, and could perform a seven-parameter CBC. The Model S could perform not only WBC and RBC counts, but also reported Hemoglobin, Hematocrit, Mean Corpuscular Volume (MCV), Mean Corpuscular Hemoglobin (MCH) and Mean Corpuscular Hemoglobin Concentration (MCHC). In 1955 it took one or several technologists 2 hours to perform a CBC, and in 1969 an automated hematology analyzer could analyze a sample in under 2 minutes.
Image 2. “Woman Using a Model F Coulter Counter Cell Counter,” 1969. Beckman Historical Collection, Box 58, Folder 94. Science History Institute. Philadelphia. https://digital.sciencehistory.org/works/736664585.
Image 2. “Woman Using a Model F Coulter Counter Cell Counter,” 1969. Beckman Historical Collection, Box 58, Folder 94. Science History Institute. Philadelphia. https://digital.sciencehistory.org/works/736664585.
As these improvements and advancements continued, and Coulter patents expired, new manufacturers entered the field. Technicon Instruments Corporation, Ortho Diagnostics, Instrumentation Laboratories and Toa Medical Electronics, (presently Sysmex Corporation) were among the first Coulter competitors. From a simple automated blood cell count, to the first seven-parameter CBC, we saw hematology changing before our eyes. More reliable automated platelet counts were added in the 1970s. In the 1980s we saw the first hematology analyzers that could perform automated differentials and the first automated reticulocyte analyzers. In the late 1990’s, we saw the advent of digital cell images and automated manual differentials.
Today, modern automated cell counters sample blood, and quantify, classify, and describe cell populations. These instruments use optical light scatter, impedance methods based on the Coulter principle or a combination of both optical and impedance methods. Progressive improvement in these instruments has allowed the enumeration and evaluation of blood cells with great accuracy, precision, and speed, at a very low cost per test. The latest descendant of the Model A Coulter Counter, the LH 750, can determine 26 reportable hematological parameters. The Sysmex XN-9100 with four XN analyzers reports 30 parameters and has a throughput of up to 400 CBCs and 75 smears per hour. Today’s analyzers can accomplish more and more routine diagnostics, and the role of the hematology technologist continues to evolve and expand.
This is not your grandmother’s hematology! We’ve truly come a very long way in 60 years. Modern hematology instruments not only perform a CBC, but they give us next generation diagnostics as well. Many give us advanced clinical parameters and other new parameters which provide physicians with additional information about the state of blood cells. We can report out immature granulocytes with every differential, automated nucleated red blood cell counts, immature platelet fractions and fluorescent platelet counts, and report the amount of hemoglobin in reticulocytes and the immature reticulocyte fraction. Future directions of hematology instrumentation include the addition of even more new parameters. In upcoming Hematology blogs I will be presenting case studies that highlight each of these advanced clinical parameters and discuss how physicians can use this new information in making diagnoses.
SLAS TECHNOLOGY: Translating Life Sciences Innovation. The Coulter Principle: Foundation of an Industry. Marshall Don, Ph.D., Beckman Coulter, Inc.. Volume: 8 issue: 6, page(s): 72-81. Issue published: December 1, 2003 https://doi.org/10.1016/s1535-5535(03)00023-6
Medical Electronic Laboratory Equipment 1967-1968. G.W.A Dummer and J. MacKenzie Robertson. 1967 Pergamon Press
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
In the “old days” in the clinical laboratory, the main sources of potential radioactive substances were found in the Radioimmunoassay (RIA) department. Techs who worked in this specialized testing area handled reagents which often were radioactive isotopes. The materials were used to label specific antigens which would compete with unlabeled antigen from patient samples. This method would allow the determination of high-quality quantitative diagnostic values. In the early 1990s, radio-immunoassays were commonly used to perform thyroid testing, narcotics assays, and a variety of hormone level analyses. Unfortunately, the use of such isotopes for testing was costly, difficult to automate, and their use was potentially hazardous to staff. Eventually this major testing method was replaced by ELISA testing, chemiluminescence, and other techniques, but some labs still do utilize RIA analysis today.
In the Anatomical Pathology areas, there has been potential radiation exposure from certain specimens in the past, and newer techniques have introduced other sources into the lab as well. Tissues (such as thyroid gland sections) are not typically removed from patients when treated with radioactive dyes, but it can occur. Good communication to the lab from surgery staff is important so that no one is unnecessarily exposed. Sentinel lymph node biopsies are sometimes infused with radioactive tracer dyes. Pathology staff may also receive radioactive seeds used to treat prostate cancer. Usually these seeds have decayed sufficiently and are inert, but that may not always be true. Again, clear communication about these samples is important. Other radioactive seeds are now used for breast tumor localization, and these do arrive in the lab while radioactive, and they must be handled and stored with care.
The best protection from radiation exposure is distance, duration, and barriers. Being away from a radiation sources isn’t always possible, but working with them for short periods and using some form of barrier protection will help. The types of radioactive material handled in labs today generally emit low levels of energy, and the use of Standard Precautions offers sufficient protection. Gloves, lab coats and face protection will provide the necessary protective barriers when handling these standard materials (Note: items like thyroid tissue that have been infused with Iodine-125 contain above-normal levels of energy and should be treated with extra care).
The College of American Pathologists (CAP) updated its regulations last year regarding radiation safety in the laboratory. Some of the standards were moved from the Anatomic Pathology checklist, and some are new. When asked, the CAP has stated that these standards do not apply to laboratories that handle low-level radiation samples such as sentinel lymph node biopsies.
First, the regulations require radiation safety handling policies and procedures which are maintained in a radiation safety manual. This manual can be paper or electronic, and it does not need to be separate from other lab safety policies. The policies should need to spell out who in the lab is authorized and restricted from handling radionuclides. Specific procedures should also be maintained to describe what actions to follow in the event of a radionuclide leak or damage to radioactive seeds. All radioactive materials and supplies should be inspected to ensure that there is no leakage or compromise that could expose staff unnecessarily.
The updated standards also require workplace radiation decontamination procedures, and labs that perform this type of work must keep records that document the effectiveness of the decontamination processes. Laboratories that handle radioactive substances must post radiation warning signs to communicate to others the potential dangers present, and all laboratory and medical staff must have comprehensive training prior to handling radioactive substances. Lastly, the CAP checklist now requires that if radioactive substances are handled in the lab, a laboratory representative must participate as a member of an institutional radiation safety committee.
Many things have changed in the laboratory setting over the past decades, and the regulations keep changing in an effort to stay current. The bottom line for radiation safety regulations in the lab is that staff need to be aware of what radioactive substances they may become exposed to, so they need to know safe handling processes as well as emergency response procedures. In the real world of lab medicine, radioactive substances do not glow, so lab staff may not be aware of the dangers when they enter the department. If the proper communication and practices are in place, however, everyone can maintain the minimum radiation exposure levels needed to live long and safe lives.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
History plays a significant part in the development of any person; we are changed and altered by big historical events that take place during our life time. Understanding history is therefore an essential aspect of understanding people, communities, cultures, and generations.
The oldest generation living today is the GI Generation. This generation was born between circa 1901-1926 and have gone through significant changes in life and work environments during their lifetimes. The term GI Generation stems from the fact that a lot of soldiers from both WWI and WWII came from this generation. This generation came of age during the First World War and the Great Depression and most grew up without electricity, refrigerators, and credit cards.
The Traditionalist Generation was born around 1927-1945, so during the Great Depression and at the end of WWII. This is the era of pre-feminism, so women generally stayed at home to raise children. If women had jobs, it was typically until they were married and in professions such as secretary, nurse, and teacher.
This started to change during the next generation, the Baby Boomers, who were born between 1946 and 1964. The timeframe for this generation is so large that there are essentially two main groups: the revolutionaries from the ‘60s and ‘70s and the yuppies of the ‘70s and ‘80s. Women began working outside the home in record numbers, which created double-income households. Divorce also became more accepted and people starting buying things on credit.
The following generation is Generation X, who are born circa 1965-1980. Because most of their parents both worked, this generation is known as the “latch-key kids”, because they would walk home after school themselves as both their parents were working or divorced. This generation experienced the transition to digital knowledge, but remembers a time without computers.
The Millennial Generation, also known as Generation Y, was born around 1981-2000. This generation grew up in a world of technology and they have experiences some significant technological advances, which typically are very natural to them. They also grew up with enormous academic pressure and also the notion that you might not be save at school due to school shootings.
The newest generation is Generation Z who are born after 2001. People born during this time have never known a world without cell phones or computer and they are very technological savvy. Growing up during the great recession of the late 2000s, Z’ers feel unsettled and a level of professional insecurity.
The events mentioned above are all focused on events that took place in the United States of America, with some worldwide events included. To understand generations from other countries, it is important to learn about important historical events that occurred, while there are also some events that overlap. For instance, internet and cell phone are more widely available worldwide and there might be some similarities across nations in terms of the effect on generational understanding.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
The GI generation experienced events that impacted their assertive characteristics. If you know someone in this generation, they probably worked until they couldn’t work anymore instead of retiring. This work ethic comes from growing up during the deprivation of the Great Depression and are often referred to as the “Greatest Generation.” This term was coined by the NBC Nightly News anchor, Tom Brokaw in his book by the same name.
The Traditionalist generation are, well, traditional. The value old-time morals, safety, security and may try your patience, especially in the work place. They are still working and act as the historians of the organization and/or the family because they have been there for a long time. You still might see them serve on Board of Directors and are Presidents because of their organizational knowledge and expertise. They are also known as the Silent Generation for an interesting reason. It was this generation that coined the phrase, “Children are to be seen, and not heard!”
Did you know there are two groups of Baby Boomers? The first group was born between 1946 and 1964. They are often called the “Leading-edge Boomers.” Those born between 1955 and 1964 are often called the “Shadow Boomers or Generation Jones.” The Baby Boomers are the largest generation in the US today, but they are slowly overpowered by the Millennial Generation. The have a team-oriented attitude and take their self-worth from their job. They are driven and optimistic and are often willing to learn how to use technology, but it takes a process as it doesn’t come as natural to them as to younger generations.
The Generation X are often referred to as the “middle child.” This generation is street smart because most grew up in homes where both parents worked or were divorced. They started school without computers, but are experienced with them. They change careers often and are independent, flexible, and can easily adapt to new circumstances. They have an entrepreneurial spirit.
The Millennial Generation is our fastest growing generation in the U.S. workforce. They are the most diverse and are also known as the “Echo Boomers, Millenials, or Generation Y. Millenials understand the world of technology and it comes natural to them. They are resilient, optimistic, and creative because they experienced enormous academic pressure. They are very focused on professional development and to learn and improve what they do.
Generation Z is just starting to enter the workforce and they are independent, open-minded, and determined. They also have an entrepreneurial spirit, like Generation X, and they are loyal and compassionate. This emerging generation will be our new teachers because their minds work in so many directions because of their technology skills and aptitude.
It is easy to see how working with multiple generations in one department offers a full range of experiences, work styles, ideas, as well as, challenges. How can you improve the generational diversity of your personal or professional life?
-Catherine Stakenas, MA, is the Senior Director of Organizational Leadership and Development and Performance Management at ASCP. She is certified in the use and interpretation of 28 self-assessment instruments and has designed and taught masters and doctoral level students.
Labs: the final frontier. These are the voyages of lab-techs everywhere. Our continuing mission: to explore strange new orders, to seek out new tests and new sero-preparations, to boldly notify floor clinicians about sample hemolysis for redraw…
Or at least that’s close enough to Gene Roddenberry’s vision for futurism in exploration—except instead of starships, we’re talking Star Labs. Happy 2018 Lab Week everybody, and thanks for checking back in!
Okay, so here’s something a little bit different. Different from my usual Zika or medical school posts, this piece is a celebration of several lab “truths” which I know many of us share. It seems like one of the overarching themes I’ve encountered regarding laboratory operation (and appreciation) is communication. Expectations and needs aren’t always communicated effectively across different medical disciplines and scopes. A while back I thought of 40 things every lab professional should know, but I’d like to expand on that a bit.
How many times have you said or encountered any of the following:
Why does the blue top have to be full, if the other ones weren’t as full?
I just put some blood from the lavender top into the tiger top—patient is a hard stick…
I’m checking on results for the patient in room 123…no, I don’t have their MRN…
There’s a trauma patient coming in via helicopter, I need crossmatched units before they’re here.
Can you please add on a serum lactic acid, there was a BMP from yesterday?
This C. Diff sample is solid…
Why are some hospitals’ rapid flu-tests done with just the swab of a swab kit, a little aliquot of saline from an IV push syringe, and a wasted no gel SST?
Are the results ready for the biopsy we did just now?
Do we have a critical value range for ESR?
We haven’t had an in-service on running POCT Glucose controls, so we haven’t done them yet
I didn’t want the tubes to leak in transit, so I used the labels as tape to keep the caps on!
In order to get SUPER GOLD STAR STROKE AND GOUT CENTER accreditation, we have to slash TATs by 40%
Captain Hematologist Jean Luc Picard (front) pleads with a clinician that only wants the WBC and H/H from a clotted CBC. Second Officer Riker (bottom left) smiles because he knows clots are dangerous for most analyzers. Lt. Operations Officer Worf (top right) agrees firmly for the sake of honor and quality assurance. An ensign trains on urinalysis (top left). [Source: StarTrekTNG]I’m sure by now you realize I could go on, and on, and on…There are always issues in laboratory medicine that don’t always translate well between floor clinicians and laboratory staff. It’s a tale as old as time. And, until we do develop universal translator technology, it will remain somewhat of a barrier to improving workflow. So how to we fix it? I argue it starts with Lab Week.
Lab Week is supposed to celebrate the clinicians, laboratory professionals, and ancillary staff that work diligently to produce results. Hundreds of thousands of laboratorians work throughout the country and are highly-trained, well educated professionals who use their expertise to diagnose and monitor treatments. Quality medical testing and exceptional care are part of the core values that each of us are celebrated for every year in April! Let me be clear, we are not support services for other clinical professionals—we’re all on the same team. Don’t be angered by the misinformed questions above, or by the stereotypes you might encounter in pathology, try and use them as teaching platforms within our community.
Capt. Hematologist Jean Luc Picard (right) takes endorsement from Chief Instrument Engineer Geordi LaForge (left) and while examining active Laboratory Data (center) speaks with clinical staff regarding temporary procedural changes for sending and holding PTT mixing studies while maintenance is being completed. [Source: Star TrekTNG]The whole point is that we’re in this together. Not just interdisciplinary teamwork that makes this year’s Star Lab theme so poignant, but teamwork across scopes. Those calls and messages we get in our managers’ offices or various bench top phones are part of our team too. It’s about the patients. We already know we contribute over 70% of clinical relevant information in every patient’s chart—some diagnoses like cancer rely completely on pathologist interpretation for screening, diagnosis, staging, and treatment recommendations.
While EMH Drs. Mark I and Mark II receive their “bad” results, it’s all part of a larger picture. As a note, “panic results” rarely illicit the expected reaction in the nurses and physicians we report them to. These doctors would think our current medical practice standards medieval, anyway… [Source: Star Trek Voyager]Here are a few examples of effective communication you could keep in mind.
For any Laboratory Professionals reading:
Instead of this: “Our policy is to reject clotted CBCs, we need a redraw, sorry.”
Try this: “While policy says to reject clotted CBCs, it’s not just because it could affect your PLT count. Other cell counts may be affected, and micro-clots can jam up the sensitive lines in the analyzers shutting them down for a while and affecting other patients’ results.” Try and realize that clinicians really do rely on those results! First and foremost, many clinical decisions are made on that last pending result for the next step of treatment. Whether it’s a PLT count or an acetone level, every result matters.
Instead of: “Room numbers aren’t adequate for patient and sample identification, sorry.”
Try this: “Because room numbers can change so quickly, we can’t use them to properly identify a specimen or patient. Do you have any of the following information…?” Understand that doctors, nurses, etc. aren’t always calling the laboratory from a private area. Thus, with so many people walking around a medical unit, a name might not be an option for them to use—room numbers are a sort of code for HIPAA compliance.
For any Clinicians reading:
Instead of this: “I really need you to rush that type and cross, quickly.”
Try this: “What can I do to help facilitate quicker turn-around for getting these units available for my patient?” Not only will you have started a conversation with the bench tech working on crossmatches, but you’ll demonstrate awareness of the complex process of safety/reportability blood bank goes through. Understand that Blood Bank is one of the more highly regulated aspects of laboratory medicine; FDA guidelines treat blood products as both a controlled substance and a tissue transplant, effectively.
Instead of this: “You have to run these samples because the patient is a hard stick.”
Try this: “What would be the minimum amount sufficient to run a particular test?” and if you need more information, simply ask! You’d be surprised how much the lab scientist on the phone would know about a particular testing method. Understand that QNS guidelines for specimens are not arbitrary amounts for the sake of covering repeats or mistakes in analysis. They are there to ensure quality results based on research and efficacy for a given instrument or method.
We all get angry. Especially at work, when our labs might be understaffed, overloaded, and dealing with instrument failures or evil advanced genetically modified arch-nemeses on the floors like Laboratory Manager Capt. Kirk (pictured). [Source: Star Trek the Wrath of Khan]So, it’s okay to get frustrated. It’s human. But I’ve got to tell you, I have been on both sides of this now—as a laboratorian and a clinician—and what I see time after time are simple gaps in communication. If we want to get better, not just for us, but for our patients, we should play an active part in helping close that gap.
I gave a few examples above, but how do we really change anything? My answer: interdisciplinary collaboration—and that’s not just a buzz word from my finishing LMU! If we want to really change anything, we should start it. If you’re a bench tech, start a discussion with your senior staff, supervisors, and managers about what you feel could be improved. If you’re a manager, seek out those barriers and be an active advocate for your staff—you’re already an advocate for the lab. If you’re a clinical pathologist, coordinate with your colleagues on the floor, develop more relationships, reach out for more than just consults on sign-outs.
Don’t be afraid to be a voice for change. Staff meetings, in-services, and self-aware improvement can be facilitated with good leadership, organization, and clear goals! Even if things look grim and you’re on downtime with a full ER, or stuck in the middle of a volatile asteroid field, noted barriers to improved communication will always GET RESULTS. [Source: Star Trek TNG]Want to change the knowledge gaps between clinical staff and laboratory staff? Hold an in-service or distribute messages with the missing information. When I was at Northwestern Medicine’s Blood Bank, I was an instructor once a month for nursing staff regarding blood products and transfusion protocols. We walked through the process with new nurses from proper phlebotomy and labeling, to order sets, to transfusion, to dealing with transfusion reactions. It was excellent! It was a great time to answer many questions and also gain insight into the clinical side of transfusion medicine.
Want to make sure no more sideways or crooked labels get sent to your specimen receiving stations? Instead of relying on the shear number of rejections to speak for themselves, discuss policy changes with your management, find the barriers to this change of specimen labeling, even send flyers out with “best dressed” tube images—it’s worked, I’ve seen it!
Want to make sure pathology stereotypes aren’t continued into the future? Change them! I plan to! Everyday I think of new ways to facilitate a new model of inclusion for pathologists into clinical healthcare teams. They’re an integral member already, why not reach past that tumor board, or biopsy report?
It takes a village to run a lab, or a space station. An interdisciplinary team is the only way healthcare can continue to improve. Shapeshifting flexibility, shrewd business deals, passion for quality assurance, creative license, and scientific knowledge are only as good as the teamwork they are a part of—even if you have religious emissaries on your staff. Sharing knowledge and effective communication are critical for labs, clinicians, and our patients. [Source: Star Trek DS9]The bottom line: if laboratorians want to grow and advance into the changing fronts within healthcare, we should take this opportunity during Lab Week 2018 and really embrace our profession as part of an interdisciplinary team. We deliver exceptional care and advocate for patients through our quality work in detecting, reporting, and preventing illnesses. I recommended laboratory professionals become more actively involved with fellow clinicians to directly improve patient outcomes. Let’s teach, let’s change policies, let’s have interdisciplinary rounds, let’s have roundtable discussions, let’s advocate together.
Because, after all, aren’t we advocating for the same thing: our patients.
Thank you! See you next time, and Happy Lab Week!
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student at the American University of the Caribbean and actively involved with local public health.
A 26 year old African American female with sickle cell anemia presented to a New York emergency room with cough, chest pain, fever and shortness of breath. Laboratory results showed an increased white blood cell count, slightly decreased platelet count and a hemoglobin of 6.2 g/dl. Her reticulocyte count was 7%, considerably below her baseline of 13%. Consulting the patient’s medical records revealed history of stroke as a child and subsequent treatment with chronic blood transfusions. She was admitted to the hospital for acute chest syndrome and aplastic crisis and care was transferred to her hematologist. Two units of RBCs were ordered for transfusion.
The blood bank technologists checked the patient’s blood bank history and noted her blood type was A, Rh(D) positive, with a history of a warm autoantibody and anti-E. The current blood bank sample confirmed the patient was blood type A, RH(D) positive with a negative DAT but the antibody screen was positive. Anti-E was identified. Per request of the hematologist, phenotypically similar units were found and the patient was transfused with 2 units of A RH(negative), C/E/K negative, HgS negative, irradiated blood. The patient’s hemoglobin rose to 8g/dl and she was discharged from the hospital 3 days after transfusion.
Ten days after discharge the patient returned to the emergency room with symptoms including aching muscles, fever and chills. A delayed transfusion reaction was suspected. A type and screen was immediately sent to the blood bank. The post transfusion type and screen remained positive for anti-E, DAT was negative. No additional antibodies were identified. However, a CBC sent to the lab at the same time revealed malarial parasites on the peripheral smear. The patient was consulted for a more complete medical history and reported that she had never traveled outside of the country. A pathology review was ordered and the patient was started on treatment for Plasmodium falciparum.
Discussion
Red Blood cell transfusions can be life saving for patients with sickle cells anemia. These patients are frequently transfused by either simple transfusion of red cell units or by exchange transfusion. Because of this, alloimmunization is reported to occur in 20% to 40% of sickle cell patients.1 Blood bank technologists are very diligent in adhering to strict procedures and follow a standard of practice aimed to prevent transfusion reactions. While preventing immune transfusion reactions may be the most forefront in our minds when transfusing the alloimmunized patient, it is important to consider transfusion transmitted diseases as a potential complication of blood transfusions.
Malaria is caused by a red blood cell parasite of any of the Plasmodium species. Mosquito transmitted infection is transmitted to humans through the bite of an infected mosquito. Transfusion-transmitted malaria is an accidental Plasmodium infection caused by a blood transfusion from a malaria infected donor to a recipient.
Donors, especially those from malarial endemic countries who may have partial immunity, may have very low subclinical levels of Plasmodium in their blood for years. Even these very low levels of parasites are sufficient to transmit malaria to a recipient of a blood donation. Though very rare, transfusion-transmitted malaria remains a serious concern for transfusion recipients. These transfusion-transmitted malaria cases can cause high percent parisitemia because the transfused blood releases malarial parasites directly into the recipient’s blood stream.
Blood is considered a medication in the United States, and, as such, is closely regulated by the FDA. Blood banks test a sample of blood from each donation to identify any potential infectious agents. Blood donations in the US are carefully screened for 8 infectious diseases, but malaria remains one infectious disease for which there is no FDA-approved screening test available. For this reason, screening is accomplished solely by donor questioning.2 A donor is deferred from donating if they have had possible exposure to malaria or have had a malarial infection. Deferral is 12 months after travel to an endemic region, and 3 years after living in an endemic region. In addition, a donor is deferred from donating for 3 years after recovering from malaria. It is important, therefore, for careful screening to take place by questionnaire and in person, to make sure that the potential donor understands and responds appropriately to questions concerning travel and past infection.
Malaria was eliminated from the United States in the early 1950’s. Currently, about 1700 cases of malaria are reported in the US each year, almost all of them in recent travelers to endemic areas. From 1963-2015, there have been 97 cases of accidental transfusion-transmitted malaria reported in the United States. The estimated incidence of transfusion-transmitted malaria is less than 1 case in 1 million units.4 Approximately two thirds of these cases could have been prevented if the implicated donors had been deferred according to the above established guidelines.3 While the risk of catching a virus or any other blood-borne infection from a blood transfusion is very low, a blood supply with zero risk of transmitting infectious disease may be unattainable. With that being said, the blood supply in the United Sates today is the safest it has ever been and continues to become safer as screening tests are added and improved. Careful screening of donors according to the recommended exclusion guidelines remains the best way to prevent transfusion-transmitted malaria.
References
LabQ, Clinical laboratory 2014 No.8, Transfusion Medicine. Jeanne E. Hendrickson, MD, Christopher Tormey, MD, Department of Laboratory Medicine, Yale University School of Medicine
Technical Manual, editor Mark K. Fung-18th edition, AABB. 2014. P 201-202
The New England Journal of Medicine. Transfusion-Transmitted Malaria in the United States from 1963 through 1999. Mary Mungai, MD, Gary Tegtmeier, Ph.D., Mary Chamberland, M.D., M.P.H., June 28, 2001. Accessed April 2018
Malaria Journal. A systematic review of transfusion-transmitted malaria in non-endemic areas. 2018; 17: 36. Published online 2018 Jan 16. doi: 1186/s12936-018-2181-0. Accessed April 2018
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
Hepatitis B surface antigen (HBsAg) is the serologic hallmark of acute Hepatitis B virus (HBV) infection. It can be detected in serum using immunoassays a few weeks after HBV infection, and normally disappears after 4-6 months in recovered patients (1). Antibodies against HBsAg (anti-HBs) appears as a response from the host immune system, and these antibodies neutralize HBV infectivity and clear circulating HBsAg (2). Anti-HBs generally persist in life, indicating recovery and immunity from HBV infection.
Some of us may simply assume that the presence of anti-HBs should always associated with the loss of HBsAg. However, it is possible to see concurrent anti-HBs and HBsAg in patients. In fact, coexistence of HBsAg and anti-HBs is not rare, and has been reported in 10 to 25 percent of HBV chronic carriers in previous studies (3-4). The underlying mechanism is not fully understood but several reports explained it as HBsAg mutants escaping the immune system (2-4). HBsAg mutants are believed to arise under the selective pressure from the host immune system, or from vaccinations (4-6).
“a” determinant in HBsAg is one of the main target of anti-HBs. It has been reported that mutations in the “a” determinant of the surface gene (S-gene) result in amino acid substitutions in HBsAg, and reduce the binding of anti-HBs to HBsAg, leading to immune escape (4). The first HBV mutant was reported by Zanetti et al in 1988 as G145R mutation. In their report, infants born to HBsAg carrier mothers developed breakthrough infections despite receiving HBIG and HBV vaccine at birth (5). Since this report, several other HBsAg mutations have been reported (4, 6).
Currently, there is no easily available assay to diagnose individuals who are suspected of harboring HBsAg escape mutants. Moreover, mutated HBsAg may leads to false negativity in some serologic assays, leading to a missed diagnosis of chronic HBV infection (6). Another concern is the potential risk of transmission to others, as vaccination does not provide protection from these mutated viruses (8); this is especially important in liver transplant recipient and newborns from HBsAg positive mothers.
Liu W, Hu T, Wang X, Chen Y, Huang M, Yuan C, Guan M. Coexistence of hepatitis B surface antigen and anti-HBs in Chinese chronic hepatitis B virus patients relating to genotype C and mutations in the S and P gene reverse transcriptase region. Arch Virol 2012;157:627–34.
Colson P, Borentain P, Motte A, Henry M, Moal V, Botta-Fridlund D, Tamalet C, Gérolami R. Clinical and virological significance of the co-existence of HBsAg and anti-HBs antibodies in hepatitis B chronic carriers. Virology 2007;367:30–40.
Lada O, Benhamou Y, Poynard T, Thibault V. Coexistence of hepatitis B surface antigen (HBs Ag) and anti-HBs antibodies in chronic hepatitis B virus carriers: influence of “a” determinant variants. J Virol. 2006 Mar;80(6):2968-75.
Zanetti AR, Tanzi E, Manzillo G, Maio G, Sbreglia C, Caporaso N, Thomas H, Zuckerman AJ. Hepatitis B variant in Europe. 1988 Nov 12; 2(8620):1132-3.
Leong J, Lin D, Nguyen M. Hepatitis B surface antigen escape mutations: Indications for initiation of antiviral therapy revisited. World J Clin Cases 2016;4:71.
Colson P, Borentain P, Motte A, Henry M, Moal V, Botta-Fridlund D, Tamalet C, Gérolami R. Clinical and virological significance of the co-existence of HBsAg and anti-HBs antibodies in hepatitis B chronic carriers. 2007;367:30–40.
Thakur V, Kazim S, Guptan R, Hasnain S, Bartholomeusz A, Malhotra V, Sarin S. Transmission of G145R mutant of HBV to an unrelated contact. J Med Virol 2005;76:40–6.
-Xin Yi, PhD, DABCC, FACB, is a board-certified clinical chemist, currently serving as the Co-director of Clinical Chemistry at Houston Methodist Hospital in Houston, TX and an Assistant Professor of Clinical Pathology and Laboratory Medicine at Weill Cornell Medical College.
Sepsis is a medical emergency and a global public health concern. The Surviving Sepsis Campaign started in 2012 and has since issued International Guidelines for Management of Sepsis and Septic Shock. These Guidelines have been updated several times, and the 4th edition of the 2016 guideline have been issued. The Guidelines are written from the perspective of developed (“resource-rich”) countries, where critical care settings are equipped with tools for managing these patients. Yet, the developing world carries the greatest burden of sepsis-related mortality. Unfortunately, the developing world lacks access to many of the necessary tools for managing the critically ill patient – including basic laboratory testing.
Laboratory values are a significant part of the management of the septic patient. Take a look at the sepsis screening tool. Analytes and lab tests included in screening patients for sepsis include: lactate, creatinine, bilirubin, INR, and blood gases. The Surviving Sepsis bundles require a lactate concentration within 3 hours of presentation, and a subsequent lactate within 6 hours. The care bundle also requires a blood culture within 3 hours of presentation and prior to administration of antibiotics. Early-goal directed therapy for sepsis requires administration of crystalloid based on lactate concentrations. Basics of laboratories in the US, lactate and blood cultures are both difficult to obtain and far from routine in the resource-poor care settings.
Blood gases and lactate are particularly difficult to find and to maintain in the developing world. While there are a number of point-of-care or small benchtop devices – like the iStat (Abbott), the Piccolo (Abaxis), and the Stat Profile pHOx (Nova), it is often cost-prohibitive to maintain these devices. The iStat and the Piccolo are examples of cartridge-based devices. All of the chemistry takes place in single-use cartridges and the device itself is basically a timer. In my experience, cartridge based devices hold up in environmental extremes better than open reagent systems. However, they are not cheap and this can be prohibitive. Cost of a single cartridge can range from $3-10 USD. In countries where patients and their families are expected to pay upfront or as they go for even inpatient medical care, and the income for a family is $2USD/day, routine monitoring of blood gases and lactate by cartridge is just not feasible. Reagent based devices like the Stat Profile use cartons of reagent for many uses. This is much cheaper – if all the reagent is used before it expires! Some healthcare settings can accommodate only 1-3 critical patients, and might not be able to use a whole carton before the expiry, even when adhering to Surviving Sepsis guidelines.
Blood cultures and subsequent treatment with appropriate antibiotics is a large part of the surviving sepsis campaign. Microbiology in the developing world is often limited to a few reference laboratories in country. Also, the number of potential infectious agents is larger in the developing world where diseases like malaria and dengue fever are common. Multiplexed nucleic acid tests might fill the gap here. Again, the cost is a major factor. Just reagents alone for a single multiplexed NAT can be over $250 USD.
In short, if the surviving sepsis guidelines really do help decrease sepsis mortality, the developing world doesn’t have a chance unless it has a greater laboratory capacity. Basic labs that we don’t think twice about can be very hard to come by in resource-poor environments. The tests already exist in forms that can be used in resource-poor settings – they just need to be cheaper, at least for those in limited resource settings. Are you listening, Abbott?
–Sarah Riley, PhD, DABCC, is an Assistant Professor of Pediatrics and Pathology and Immunology at Washington University in St. Louis School of Medicine. She is passionate about bringing the lab out of the basement and into the forefront of global health.