When I think of Lab Week, I think of all the Lab Week celebrations we’ve had in the past: Food, games, from “Guess whose baby picture?” to word searches and coworker trivia, and of course, more food. I’ve seen the same games over and over, but with new coworkers they’re always fun. Probably the most unique game I’ve seen, was “whose sample is this?” Smushed chocolate candy bars were stuffed into sample cups (and looked like you know what) and we had to guess which ‘sample’ came from which candy bar. Lab week also helps us remember the techs we’ve worked with in the past and the good times we’ve had in the lab and outside. And, of course, Lab week always seems to bring up reminiscing, and the question “Remember when?”
As a nod to lab week, I’d like to take you on a little trip down memory lane. Those of us who have been around for a while can laugh and add our own stories. The new techs in the lab, the younger generation will look at us and say “No way!”” or “You’re joking, right?”
I work in a lab that is very fortunate to have a few wonderful techs in their late 60’s and 70’s who still work for us part time. But anyone who has passed through our lab in the past 60 years remembers Irene, who is over 80, and has been here since 1963. That’s before many of us were born! Now Irene doesn’t work every day, or even every month, but she’s there for our students and newly graduated employees when we can use her talents for a few days. She has boxes full of teaching slides and comes in to review WBCs and RBC morphology with them and shares many stories about ‘the old days’ in the lab. Recently she was talking to a new grad and mentioned the old lab and the rabbits they kept in the lab.
“Rabbits?’ he asked.
“Yes, youngster, let me tell you about it.”
Rabbits were used for the first pregnancy tests. The first HCG tests came out in the early 1970’s, but before then, the question “Did the rabbit die?” was associated with a positive pregnancy test. Young rabbits were injected with urine or blood from a woman, and several days later, the animals were dissected to look for enlarged ovaries, a sign that HCG was present in the injected specimen, and a positive pregnancy test. So, in reality the rabbit (or mouse, or frog) always died, whether the woman was pregnant or not.
I fortunately missed the live animals in the lab era. Now that I’m working with techs who are younger than my kids (and not that much older than my grandkids!), when us ‘old timers’ talk about what the lab used to be like, we get incredulous wide-eyed stares.
“You didn’t wear gloves??”
“They drank coffee in the lab?”
“No computers?”
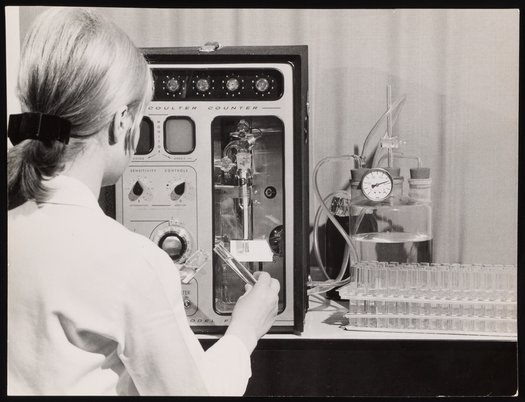
In my very first job out of college I worked in a hospital lab, and trained in Hematology, Chemistry and Blood Bank. It was the time of the rise in automation, and we had some great ‘new’ analyzers. We had a Coulter S in hematology, the first automated hematology analyzer. The Coulter S offered 7 parameters. In about 1 minute it could analyze and report the WBC, RBC, Hgb, Hct, MCV. MCH and MCHC. Before this we had to prepare samples, lyse RBCs to count WBCs, perform hemoglobin measurement on a spectrophotometer, and calculate the indices! If a physician wanted a differential, we stained slides by hand and counted a 100-cell diff. Platelet count counts fortunately were not ordered on every CBC because those were counted manually!
I remember training in the chemistry department with a lot of instruments which each did only one or 2 tests. Individual tests were done on single test analyzers. Which meant a lot of techs in the lab, and you could be assigned to a bench where you did just Na and K on the flame photometer or just Glucoses and BUNs on single test analyzers all day. We did have a STAT analyzer which did electrolytes, glucose and BUN, and a larger analyzer that did 12 test panels, but they were only used when the full panels were ordered. These multi test analyzers were new and exciting, but in 1980 we were still uncapping and pouring off all our samples by hand. Without gloves!
“What?? No gloves?”
No gloves. We drew blood and worked in the lab with no gloves. Analyzers had glass coils that techs changed with their bare hands, and there were accidents. Techs contracted hepatitis and in the 1980’s the fear of contracting HIV was real. It wasn’t until 1992, when the Occupational Health and Safety Administration (OHSA) published the Bloodborne Pathogens Standard. There was increased awareness of HIV, and OHSA implemented universal precautions to protect workers who may come in contact with bodily fluids. OSHA’s standard required employers to provide personal protective equipment, including disposable gloves.
I once read an article that said that medical technician/technologists were the profession that drinks the most coffee. Now, I don’t know about that because I don’t drink coffee, but what they didn’t mention in the article was that they used to drink it in the lab! Yes, the cup of coffee often sat next to the microscope while doing diffs. And remember, no one wore gloves. I remember a doctor walking through the lab smoking a cigar. And while I don’t remember if I ever saw eating in the lab, I’m pretty sure it happened. These things are so taboo to us now that sometimes we wish we were camels because we often go for hours without a sip of water! We may have been the profession who drinks the most coffee, but today we may be the most dehydrated because the closest ‘clean ‘area to get a drink is way down the hall! And we’re too busy to leave our work and go get a drink!
People often use the term ‘The Good Old Days’ when talking about the past, but in the lab, these times weren’t always ‘good’. Yes, we had good times. But there were also practices that weren’t what we would today consider safe. Besides the lack of gloves, and coffee in the lab, there was also mouth pipetting. Remember spit strings? Techs kept them in their pockets for use in mouth pipetting body fluids (shudder). We washed glassware, even literally rinsing blood out of test tubes and reusing them.
We also love to reminisce about obsolete lab tests. I remember when AST, LDH and CK were used for markers of myocardial infarction. Then we had a new test, the CK-MB, which is now designated antiquated and has been replaced by cardiac troponin I for diagnosing MI. Bleeding times were once widely used as a platelet function test. Today this rather crude test is rarely used and not even offered by many labs. Glass in the lab has been replaced by plastics from vacutainer tubes and blood bags to graduated cylinders and beakers. We no longer count platelets on a hemocytometer because our automated analyzers perform platelet counts. In Urinalysis, we used to do confirmatory tests for glucose, bilirubin and protein in urine. And so many more tests that have been replaced by newer and better testing. What is your favorite or no so favorite ‘obsolete’ lab test?
We’ve certainly come a long way in the last 60 years! Lab Week is a great time to generate new awareness and excitement about the laboratory medicine profession while having some fun with your lab coworkers. Thanks to everyone who is part of the laboratory team for your hard work and dedication. Happy Laboratory professionals Week!

DOWN
1. favorite drink to sip at the microscope while doing diffs
2. standard PPE that wasn’t so standard before 1990
3. standard set of guidelines for prevention of bloodborne pathogens
5. old confirmatory test for urine bilirubin
8. type of pipetting common in the old days
9. you probably won’t use one of these for heating in the lab today
10. historic method for testing for glucose in urine
11. animal kept in lab for pregnancy testing
12. old school test for MI
14. plastic blood collection bags have replaced these
ACROSS
4. used to draw blood before vacutainers
6. carried in your pocket as a pipetting aid
7. used for manual platelet counts
13. obsolete platelet function test
15. dark field microscopy was first test for diagnosis of this STD in 1906

-Becky Socha, MS, MLS(ASCP)CMBBCM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 40 years and has taught as an adjunct faculty member at Merrimack College, UMass Lowell and Stevenson University for over 20 years. She has worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. She currently works at Mercy Medical Center in Baltimore, Md. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.