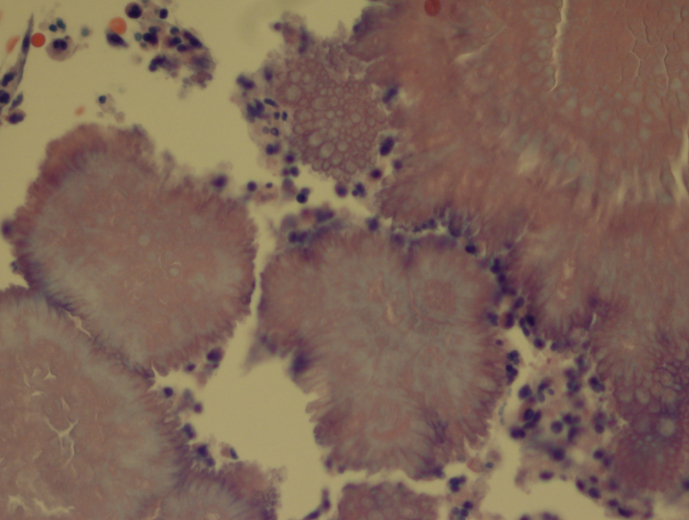
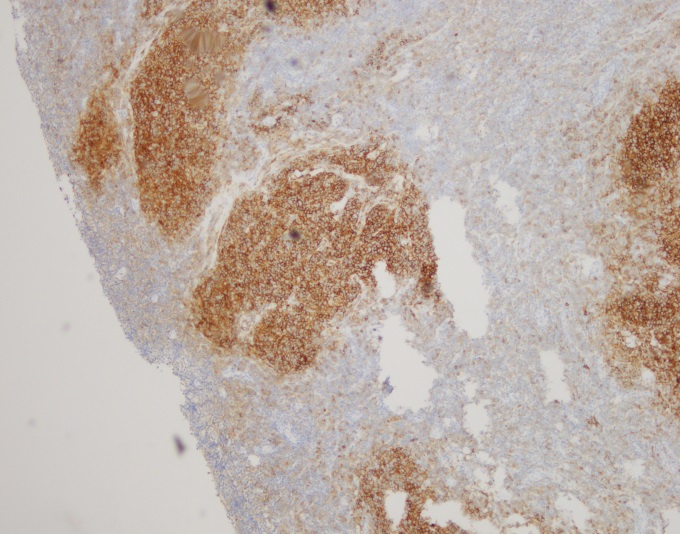
Our patient is an 83 year old female with previous history of arterial hypertension, atrial flutter and chronic obstructive pulmonary disease who presented with dry cough (~2 weeks), fever (102ºF), and cutaneous ulcerated plaques with elevated borders on forearm, foot, leg, and neck. Chest radiographs and chest CT scan showed numerous bilateral nodular consolidations compatible with pneumonia. Additionally, mild leukocytosis (14,200 cells /mm3) and hypohemoglobinemia (10.9 mg/dl) were documented. A skin biopsy was taken from the forearm lesion. Periodic acid–Schiff (PAS) and Grocott-Gomori’s (or Gömöri) methenamine silver (GMS) stains identified rare budding yeast (PAS, Image 1). Acid-fast bacilli (AFB) and Gram stains were negative for mycobacteria and bacteria, respectively.
Image 1. Budding yeast with a thick double cell wall were identified microscopically surrounded by prominent supurative granulomatous reaction (PAS, 100x).
Discussion
A diagnosis of disseminated blastomycosis was made based broad based budding yeast seen on PAS stain (Image 1).
Blastomycosis infection most commonly affects persons living in the Mississippi and Ohio River valleys, Great Lakes Region of the United States, and southern Canadian provinces. It is a fungal infection that can cause asymptomatic infection, isolated pulmonary disease, or serious and potentially fatal disseminated disease. B. dermatitidis can infect every organ of the body giving great variety of clinical manifestations, which is the reason why it is known as “the great pretender.” More than half of infected patients are asymptomatic. Symptomatic patients generally present with pulmonary symptoms, and the development of disseminated disease after hematogenous spread is common (~25 to 40% of symptomatic cases). The most common extra-pulmonary locations are: skin, bone, genitourinary tract, and central nervous system (CNS). Unlike histoplasmosis, most cases of blastomycosis are seen in immunocompetent patients, although immunocompromised patients may be at higher risk to develop severe forms of the disease.
Blastomyces is a thermally dimorphic fungus that grows as a yeast in the body and as filamentous fungi with septate hyphae in the environment. Recent phylogenic analysis has divided the Blastomyces genus into 2 species, B dermatitidis and B gilchristi . Culture of B. dermatitidis from the environment is extremely difficult, and much of what we know is conjecture from a few documented outbreaks, of which several occurred in wooded areas near waterways. These investigations found that exposure to dust clouds associated with construction or crop harvesting were the only identified risk factors for infection. Blastomycosis infection occurs through aerosolization of conidia from the environment causing respiratory infection or less commonly through direct inoculation into cutaneous abrasions. Once in the host, the conidia transform into yeast. The specific proteins expressed during the yeast phase allow the evasion of phagocytic and CD4+ cells.
Laboratory diagnosis
The most expedient method to diagnose blastomycosis remains examination of stained fluid or tissue specimens. Yeast are 8-15 µm in size with broad based buds of 4-5 µm and have a characteristic refractory double cell wall. Fluid can be stained with 10% potassium hydroxide plus calcofluor white, whereas formalin fixed paraffin embedded tissue samples can be stained with GMS or PAS. B. dermatitidis yeast can be difficult to visualize with Gram or hematoxylin and eosin (H&E) stains, but if found, the characteristic broad-based budding pattern of yeast can lead to presumptive diagnosis before culture and non-culture based diagnostic test results are available.
Culture of B. dermatitidis provides a definitive diagnosis of pulmonary and extra-pulmonary disease. B. dermatitidis grows well on routine fungal media such as Sabouraud dextrose agar, potato dextrose agar, and brain–heart infusion media. The yeast phase is inhibited by media containing cyclohexamide. Culture typically demonstrates growth in as little as 4-7 days. Colonies will initially appear yeast-like, but then develop white cottony aerial mycelium and turn tan with age. Mature growth is achieved around day 14 and the reverse of the colony is a tan color. At 25-30°C, B. dermatitidis forms septate hyphae with round or pear-shaped conidia attached to the hyphae by short or long conidiophores. This gives the characteristic appearance of “lollipops.” Scedosporium spp. and Chrysosporium spp. are common confounders because they make similar structures. Definitive identification of Blastomyces sp. can be made by conversion of the mold phase to the yeast phase by incubation at 37°C. An alternative to conversion is using a DNA probe assay.
References
Medically Important Fungi, 5th edition
Principles and Practices of Infectious Disease, 7th edition
-Julio Diaz-Perez, MD is a 1st year anatomic and clinical pathology resident at University of Chicago (NorthShore).
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois.
In the “old days” in the clinical laboratory, the main sources of potential radioactive substances were found in the Radioimmunoassay (RIA) department. Techs who worked in this specialized testing area handled reagents which often were radioactive isotopes. The materials were used to label specific antigens which would compete with unlabeled antigen from patient samples. This method would allow the determination of high-quality quantitative diagnostic values. In the early 1990s, radio-immunoassays were commonly used to perform thyroid testing, narcotics assays, and a variety of hormone level analyses. Unfortunately, the use of such isotopes for testing was costly, difficult to automate, and their use was potentially hazardous to staff. Eventually this major testing method was replaced by ELISA testing, chemiluminescence, and other techniques, but some labs still do utilize RIA analysis today.
In the Anatomical Pathology areas, there has been potential radiation exposure from certain specimens in the past, and newer techniques have introduced other sources into the lab as well. Tissues (such as thyroid gland sections) are not typically removed from patients when treated with radioactive dyes, but it can occur. Good communication to the lab from surgery staff is important so that no one is unnecessarily exposed. Sentinel lymph node biopsies are sometimes infused with radioactive tracer dyes. Pathology staff may also receive radioactive seeds used to treat prostate cancer. Usually these seeds have decayed sufficiently and are inert, but that may not always be true. Again, clear communication about these samples is important. Other radioactive seeds are now used for breast tumor localization, and these do arrive in the lab while radioactive, and they must be handled and stored with care.
The best protection from radiation exposure is distance, duration, and barriers. Being away from a radiation sources isn’t always possible, but working with them for short periods and using some form of barrier protection will help. The types of radioactive material handled in labs today generally emit low levels of energy, and the use of Standard Precautions offers sufficient protection. Gloves, lab coats and face protection will provide the necessary protective barriers when handling these standard materials (Note: items like thyroid tissue that have been infused with Iodine-125 contain above-normal levels of energy and should be treated with extra care).
The College of American Pathologists (CAP) updated its regulations last year regarding radiation safety in the laboratory. Some of the standards were moved from the Anatomic Pathology checklist, and some are new. When asked, the CAP has stated that these standards do not apply to laboratories that handle low-level radiation samples such as sentinel lymph node biopsies.
First, the regulations require radiation safety handling policies and procedures which are maintained in a radiation safety manual. This manual can be paper or electronic, and it does not need to be separate from other lab safety policies. The policies should need to spell out who in the lab is authorized and restricted from handling radionuclides. Specific procedures should also be maintained to describe what actions to follow in the event of a radionuclide leak or damage to radioactive seeds. All radioactive materials and supplies should be inspected to ensure that there is no leakage or compromise that could expose staff unnecessarily.
The updated standards also require workplace radiation decontamination procedures, and labs that perform this type of work must keep records that document the effectiveness of the decontamination processes. Laboratories that handle radioactive substances must post radiation warning signs to communicate to others the potential dangers present, and all laboratory and medical staff must have comprehensive training prior to handling radioactive substances. Lastly, the CAP checklist now requires that if radioactive substances are handled in the lab, a laboratory representative must participate as a member of an institutional radiation safety committee.
Many things have changed in the laboratory setting over the past decades, and the regulations keep changing in an effort to stay current. The bottom line for radiation safety regulations in the lab is that staff need to be aware of what radioactive substances they may become exposed to, so they need to know safe handling processes as well as emergency response procedures. In the real world of lab medicine, radioactive substances do not glow, so lab staff may not be aware of the dangers when they enter the department. If the proper communication and practices are in place, however, everyone can maintain the minimum radiation exposure levels needed to live long and safe lives.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
A propos of Lab Week 2018, the WHO announced the development of an Essential Diagnostic List (EDL). The first Strategic Advisory Group of Experts on In Vitro Diagnostics (SAGE IVD) met in Geneva in April. The role of the SAGE-IVD is to act as an advisory body to matters of global policy and strategies related to in vitro diagnostics (IVDs) – to guide the development of the EDL.
The EDL is, as it sounds, a catalog of IVDs that are essential for diagnosis, treatment, and management of diseases. An EDL was called for in 2016 by Dr. Tim Amukele, a clinical pathologist at Johns Hopkins and President of the non-profit organization Pathologists Oveseas, and Dr. Lee Schroeder, a clinical pathologist at University of Michigan Ann Arbor (N Engl J Med 2016; 374:2511-4). Amukele and Schroeder suggested the EDL to complement the WHO’s Essential Medicines List (EML). They suggested 19 categories of IVDs that are essential for 10 of the medicines appearing on the EML. As it stands, the initial EDL focuses on 4 disease areas: HIV, TB, Malaria, and Hepatitis B & C. The following categories are provided for each disease area: analyte, intended use, level of facility that should have the IVD, assay format, specimen type, and links to WHO guidelines and any WHO prequalified or endorsed products.
For example, in the disease area “Malaria”, the analyte P. falciparum has the intended use of diagnosis of P. falciparum. The rapid diagnostic assay format is recommended for all level facilities. The specimen type is capillary whole blood, and the corresponding WHO guideline is “Good practices for selecting and procuring rapid diagnostic tests for malaria, 2011”.
The EDL will provide countries a way to focus attention on which tests are most appropriate, which can have a huge impact on the cost-effectiveness of the health care system, and also improve the quality of the laboratory results. Cost-effectiveness can be achieved by 1) focusing on evidence-based IVDs appropriate for a specific disease burden and 2) facilitating proper utilization of medicines and other clinical supplies necessary for treatment/management. In my experience, many laboratories in resource-limited areas are developed seemingly on a whim; testing might reflect a pet project of an absentee lab director, or donated equipment. Focusing on more appropriate testing, as Dr. Amukele told Clinical Laboratory News, give a lab more bang for their buck. Dr. Schroeder indicated that “lab testing develop ad hoc is more prone to quality issues”. The hope is that providing more direction for development of lab testing will encourage greater quality control programs. One way I can see that playing out is, if more labs in a specific area adopt the same testing, a shared sample program for cost-effective proficiency testing might be developed.
The WHO hopes that countries will use the EDL to develop country-specific EDLs, based on the disease burden specific to the country. National EMLs have been successful. Personally, I am very excited about the EDL! The WHO efforts to control HIV, Malaria, and TB have highlighted the need for laboratory diagnostics. I think it’s about time that labs got a chance to show their worth! The EDL is an important step in bringing the lab out of the basement and onto the global health stage.
–Sarah Riley, PhD, DABCC, is an Assistant Professor of Pediatrics and Pathology and Immunology at Washington University in St. Louis School of Medicine. She is passionate about bringing the lab out of the basement and into the forefront of global health.
American Journal for Clinical Pathology is in need of an Editor in Chief.
Job Description
The Editor-in-Chief will have responsibility for the overall strategic direction of AJCP, one of ASCP’s most visible and important benefits for all Society members.
The Editor-in-Chief should have a national and international reputation, with publications in top echelon journals in the field and extensive contacts throughout the pathology community.
The Editor-in-Chief will have responsibility for actuating the editorial direction of AJCP and proactivelysoliciting and presenting timely significant research findings relating to both anatomic and clinical pathology.
This is a volunteer, term-limited, contracted position. A monthly stipend is provided. The work of the Editor-in Chief is reviewed annually.
The Editor-in-Chief will be expected to devote time daily to AJCP work, totaling approximately 10-15 hours per week.
The Editor-in-Chief will be expected to travel to major pathology and laboratory medicine meetings to solicit content and authors.
Qualifications & Requirements
Have a medical degree with a specialization in pathology (boarding in both AP and CP is particularly useful), or a doctorate in a laboratory discipline (eg, clinical chemistry).
A strong preference will be given to those with clinical experience, combined with research or academic experience.
Must have experience working with scientific, peer-reviewed journals; as a peer reviewer, and as an editor or editorial board member.
Application Content and Submission
Submissions will only be accepted prior to 4 July 2018
Please submit your full CV with “Personal Statement” that explains (in a summary paragraph for each point):
Your motivation and interest in pursuing this position
Your previous experience with peer-reviewed publications
Please prepare and submit a “Vision Statement” that explains (in 2 pages):
Your vision for the direction of the journal’s future content
Your view of the journal’s content strengths and weaknesses currently
Your understanding of the unmet needs for new types of journal content
A summary of the editorial agenda you would pursue to enact the vision
Please submit your full CV and statements to: AJCPsearch@ascp.org
Equal Opportunity Employer: /Individuals with Disabilities/Protected Veteran
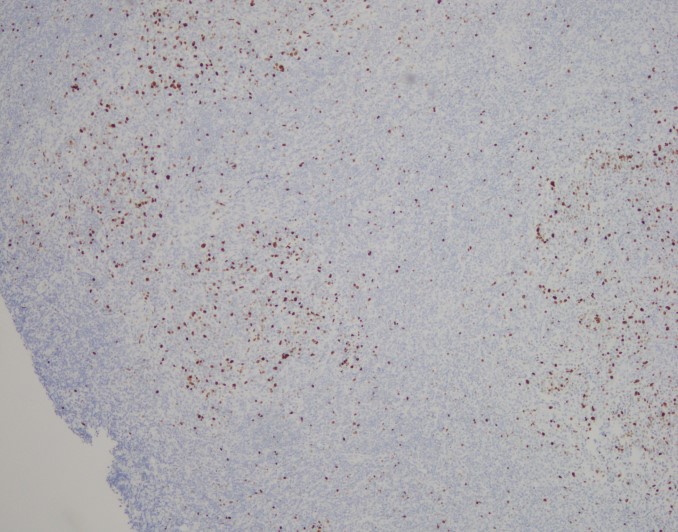
A 42 y/o female G2P2002 patient presented to her Ob/Gyn for Colposcopy for monitoring of persistent High-Risk HPV. She was originally found positive for HPV in 2015, but has had never had a Pap with a squamous intraepithelial lesion, abnormalities on colposcopy, or dysplasia seen on endocervical curettage. Additionally, she endorsed a complaint of vague diffuse pelvic/lower abdominal pain for approximately the last 2 months. She states that the pain is mild and comes and goes and is not associated with anything in particular. She has noticed some clear to gray-white discharge now and then since she first noticed the pain, but nothing that really worried her. Pt denies changes in bowel or bladder habits, denies nausea, fever, or chills. Pt has been in a monogamous relationship with her partner for the last 12 years. She had a Mirana IUD placed 4 years prior, without complication, and has not had menses since placement. Prior to that, the patient had normal, regular cycles. She has 2 children with the same father, both were delivered by spontaneous vaginal delivery without complications. She has mild anxiety and depression for which she is treated, but no other medical problems. There is no surgical history. She has 1-2 glasses of red wine every week, denies tobacco use, and denies illicit drug use.
Pelvic exam revealed a benign appearing cervix that was not painful to touch or motion. There was a clear to white mild discharge that was suspected to be normal vaginal secretions. IUD strings were noted. Colposcopy revealed an easily appreciated transformational zone without any obvious lesions. A routine endocervical curettage (ECC) was performed followed by observed increased clear discharge from the cervical os. ECC was sent for routine pathology:
Actinomyces, H&E, 20xActinomyces, H&E, 40x
Discussion
Actinomycosis is an infection by a species within the Actinomyces genus, generally seen in dental and other oropharyngeal abscess formations. However, rare occurrences of pelvic Actinomycosis can be seen in women with intrauterine devices in place. Pelvic infections can result in cervicitis and endometritis and progress into abscess formation within the fallopian tubes and the ovaries along with salphigitis. The more profound disease consisting of abscess formation generally presents with fever, specific lower abdominal tenderness, and elevated WBCs, thus can mimic acute appendicitis, ovarian torsion, or ectopic pregnancy (1). The first case reported in the literature was in 1967 (2).
Three main species of Actinomyces have been found to be associated with IUD-associated pelvic infection: A. naeslundii, A. odontolyticus (3), and A. hongkongensis (4). All of these species are obligate to facultative anaerobes, catalase negative, and nitrate reducing. A sub-species group of A. naeslundii, however, can be catalase positive and is CAMP test-positive. All members of A. naeslundii are urease positive while A. odontolyticus and A. hongkongensis are urease negative.
References
Joshi et al. Pelvic Actinomycosis: a Rare Entity Presenting as Tubo-ovarian Abscess. Arch Gynecol Obstet. 2010, 281:305-306.
Brenner et al. Pelvic Actinomycosis in the Presence of an Endocervical Contraceptive Device. Obstet Gynecol. 1967, 29: 71-73.
Woo et al. Diagnosis of Pelvic Actinomycosis by 16S ribosomal RNA Gene Sequencing and its Clinical Significance. Diagnostic Microbiology and Infectious Disease. 2002; 43: 113-118.
Flynn et al. Identification by 16S rRNA Gene Sequencing of an Actinomyces hogkongensis Isolate Recovered from a Patient with Pelvic Actinomycosis. J. Clin. Microbiol. 2013, 51(8):2721. DOI: 10.1128/JCM.00509-13.
-Jeff Covington, MD, PhD, is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
History plays a significant part in the development of any person; we are changed and altered by big historical events that take place during our life time. Understanding history is therefore an essential aspect of understanding people, communities, cultures, and generations.
The oldest generation living today is the GI Generation. This generation was born between circa 1901-1926 and have gone through significant changes in life and work environments during their lifetimes. The term GI Generation stems from the fact that a lot of soldiers from both WWI and WWII came from this generation. This generation came of age during the First World War and the Great Depression and most grew up without electricity, refrigerators, and credit cards.
The Traditionalist Generation was born around 1927-1945, so during the Great Depression and at the end of WWII. This is the era of pre-feminism, so women generally stayed at home to raise children. If women had jobs, it was typically until they were married and in professions such as secretary, nurse, and teacher.
This started to change during the next generation, the Baby Boomers, who were born between 1946 and 1964. The timeframe for this generation is so large that there are essentially two main groups: the revolutionaries from the ‘60s and ‘70s and the yuppies of the ‘70s and ‘80s. Women began working outside the home in record numbers, which created double-income households. Divorce also became more accepted and people starting buying things on credit.
The following generation is Generation X, who are born circa 1965-1980. Because most of their parents both worked, this generation is known as the “latch-key kids”, because they would walk home after school themselves as both their parents were working or divorced. This generation experienced the transition to digital knowledge, but remembers a time without computers.
The Millennial Generation, also known as Generation Y, was born around 1981-2000. This generation grew up in a world of technology and they have experiences some significant technological advances, which typically are very natural to them. They also grew up with enormous academic pressure and also the notion that you might not be save at school due to school shootings.
The newest generation is Generation Z who are born after 2001. People born during this time have never known a world without cell phones or computer and they are very technological savvy. Growing up during the great recession of the late 2000s, Z’ers feel unsettled and a level of professional insecurity.
The events mentioned above are all focused on events that took place in the United States of America, with some worldwide events included. To understand generations from other countries, it is important to learn about important historical events that occurred, while there are also some events that overlap. For instance, internet and cell phone are more widely available worldwide and there might be some similarities across nations in terms of the effect on generational understanding.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
The GI generation experienced events that impacted their assertive characteristics. If you know someone in this generation, they probably worked until they couldn’t work anymore instead of retiring. This work ethic comes from growing up during the deprivation of the Great Depression and are often referred to as the “Greatest Generation.” This term was coined by the NBC Nightly News anchor, Tom Brokaw in his book by the same name.
The Traditionalist generation are, well, traditional. The value old-time morals, safety, security and may try your patience, especially in the work place. They are still working and act as the historians of the organization and/or the family because they have been there for a long time. You still might see them serve on Board of Directors and are Presidents because of their organizational knowledge and expertise. They are also known as the Silent Generation for an interesting reason. It was this generation that coined the phrase, “Children are to be seen, and not heard!”
Did you know there are two groups of Baby Boomers? The first group was born between 1946 and 1964. They are often called the “Leading-edge Boomers.” Those born between 1955 and 1964 are often called the “Shadow Boomers or Generation Jones.” The Baby Boomers are the largest generation in the US today, but they are slowly overpowered by the Millennial Generation. The have a team-oriented attitude and take their self-worth from their job. They are driven and optimistic and are often willing to learn how to use technology, but it takes a process as it doesn’t come as natural to them as to younger generations.
The Generation X are often referred to as the “middle child.” This generation is street smart because most grew up in homes where both parents worked or were divorced. They started school without computers, but are experienced with them. They change careers often and are independent, flexible, and can easily adapt to new circumstances. They have an entrepreneurial spirit.
The Millennial Generation is our fastest growing generation in the U.S. workforce. They are the most diverse and are also known as the “Echo Boomers, Millenials, or Generation Y. Millenials understand the world of technology and it comes natural to them. They are resilient, optimistic, and creative because they experienced enormous academic pressure. They are very focused on professional development and to learn and improve what they do.
Generation Z is just starting to enter the workforce and they are independent, open-minded, and determined. They also have an entrepreneurial spirit, like Generation X, and they are loyal and compassionate. This emerging generation will be our new teachers because their minds work in so many directions because of their technology skills and aptitude.
It is easy to see how working with multiple generations in one department offers a full range of experiences, work styles, ideas, as well as, challenges. How can you improve the generational diversity of your personal or professional life?
-Catherine Stakenas, MA, is the Senior Director of Organizational Leadership and Development and Performance Management at ASCP. She is certified in the use and interpretation of 28 self-assessment instruments and has designed and taught masters and doctoral level students.
A 68 year old man with no significant past medical history presented with 3 weeks of upper back pain and bilateral leg weakness. He denied numbness, tingling, leg pain or urinary or fecal incontinence. MRI showed severe cord compression at the upper thoracic spine with a T2-T5 epidural mass. Due to the patient’s decline, an urgent decompression was scheduled and the patient underwent T2-T5 thoracic laminectamies with resection of extramedullary epidural tumor.
“Round blue cell tumor. Await permanents for final diagnosis.”
Differential Diagnosis
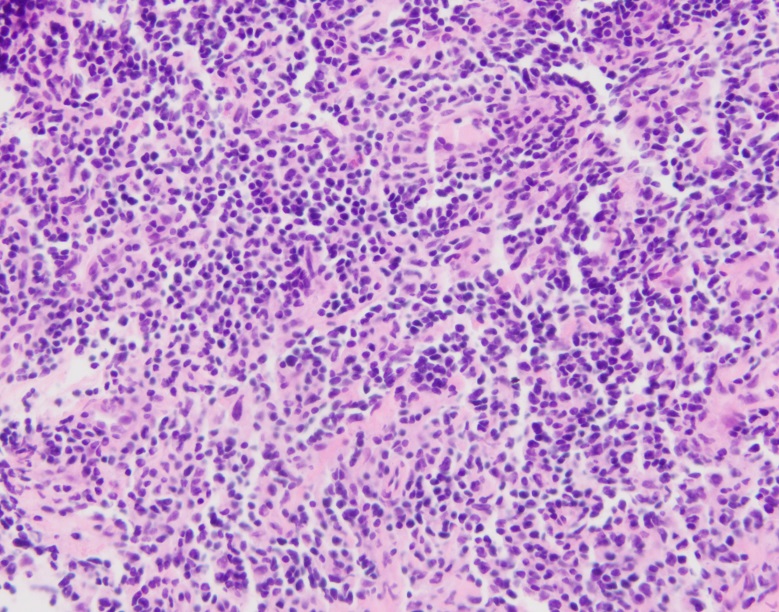
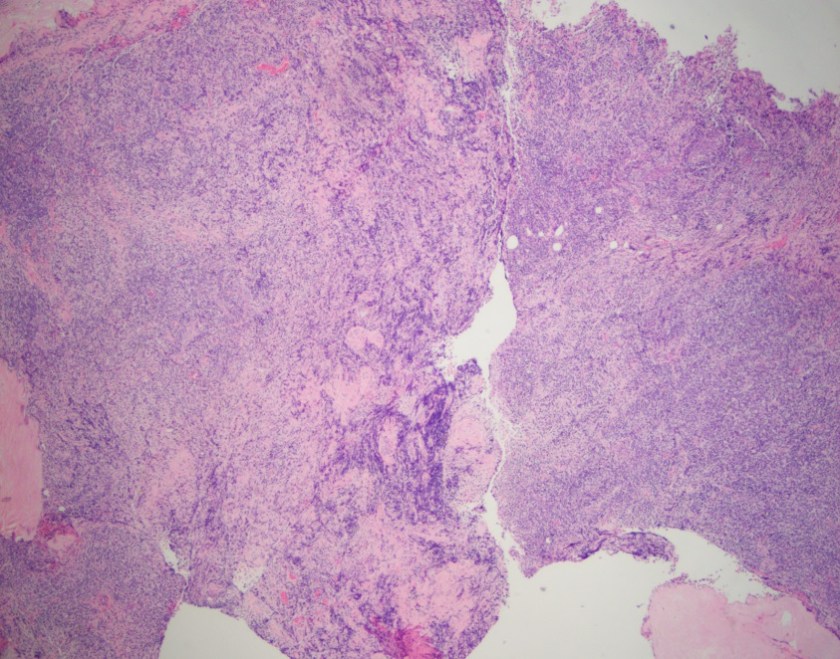
Small round blue cell tumor is a term generally used for a group of neoplasms characterized by small, round, basophilic, relatively undifferentiated cells on H & E staining. The differential diagnosis is wide, but includes Ewing’s sarcoma/peripheral neuroectodermal tumor, mesenchymal chondrosarcoma, small cell osteosarcoma, desmoplastic small round cell tumor and Non-Hodgkin Lymphoma. 1
H&E, 2x
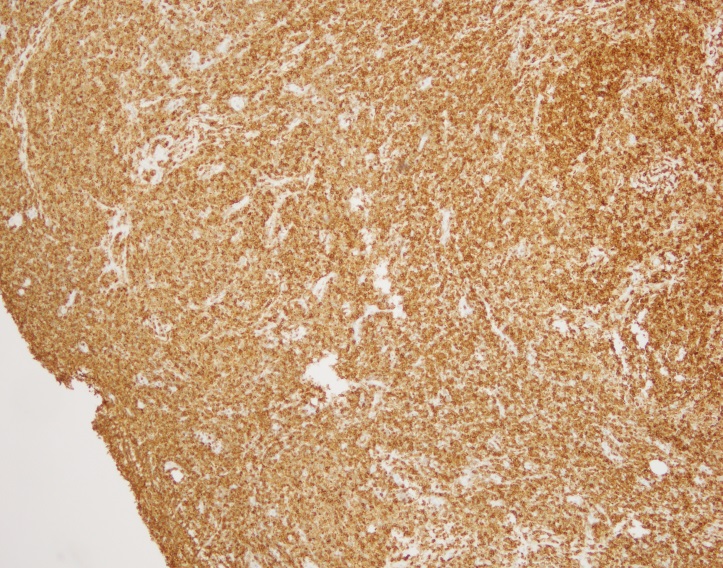
CD20, 4x
CD20, 4xBCL2, 4xCD10, 4xCD21, 4xKi-67, 4xIGH/BCL2 double fusion FISH probe. White arrows: IGH/BCL2 fusion
Diagnosis
Sections show fragments of fibrous tissue and focal bone with extensive crush artifact. There is an abnormal lymphoid infiltrate with areas showing a vaguely nodular architecture. The lymphocytes are small to medium in size with irregular cleaved nuclei, inconspicuous nucleoli and small amounts of cytoplasm. Scattered centroblastic cells are seen but are <15 per high power field. Between the nodules, the cells are centrocytic appearing. Rare mitotic figures are identified.
By immunohistochemistry, the neoplastic cells are immunoreactive for CD20 and BCL2. BCL2 is brighter in the vague nodular areas which are also highlighted by CD10 and BCL6. CD23 is variably positive in a large subset of cells. MUM1 is negative. CD21 highlights the enlarged and irregularly shaped follicular dendritic cell meshwork present in the areas with nodules. CD3 and CD5 highlights admixed T-cells. The proliferation index by Ki-67 is low and approximately 10%.
Cytogenetic analysis using fluorescent in-situ hybridization performed on paraffin embedded sections revealed numerous cells with an IGH/BCL double fusion probe signal pattern consistent with IGH/BCL2 gene rearrangement.
Overall, the morphologic and immunophenotyipic findings in conjunction with the cytogenetic results are in keeping with involvement by a B-cell lymphoma most consistent with a follicular lymphoma. The follicles present contain <15 centroblasts per hpf and the low proliferation fraction makes it most compatible with a low grade (WHO morphologic grade 1-2/3) follicular lymphoma.
Discussion
The differential diagnosis for an extramedullary epidural tumor is wide and can include anything from an epidural abscess to a metastasis. Although rare, lymphoma must be considered, especially when initial pathology shows “Round blue cells.”
Making the diagnosis of follicular lymphoma involves assessing the H & E slides for follicular architecture, characteristic immunostains including positivity for BCL2 within follicles and the typical t(14;18) IGH/BCL2 translocation, which occurs in 90% of cases. 2
Primary spinal epidural lymphoma (PSEL) includes extramedullary/extranodal lymphomas of the epidural space for which there are no other sites of disease at the time of diagnosis. As demonstrated in Figure 1 below, the lymphoma is seen entirely within the epidural space. 3
Figure 1. Primary spinal epidural lymphomas. Journal of Craniovertebral Junction and Spine (2011).
An epidural location for lymphoma is observed in 0.1-6.5% of cases. Patients tend to present in the fifth to seventh decade of life with a higher proportion of male to female cases. Presenting symptoms include weakness in the upper or lower limbs and back pain corresponding to the site of involvement of tumor. The most common tumor site is the thoracic spine (75%) followed by lumbar and cervical. Most epidural spinal tumors are B-cell lymphomas of intermediate and high grade, but low grade lymphomas have been reported. 3
Although rare, lymphoma is an important consideration in the differential diagnosis for tumors involving the spine. Surgical intervention is often necessary to relieve spinal cord compression and to make a histologic diagnosis. Treatment includes radiation and chemotherapy. Patients with primary spinal epidural lymphoma tend to have a better prognosis than patients with systemic lymphoma involving the epidural space, as well as patients with metastatic carcinoma. 3
References
Hameed, Meera: Small Round Cell Tumors of Bone. Arch Pathol Lab Med (2007) 131: 192-204.
Louis D.N., Ohgaki H., Wiestler O.D., Cavenee W.K. (Eds.): WHO Classification of Tumors of the Central Nervous System. IARC: Lyon 2007.
Cugati G, Singh M, Pande A, et al. Primary spinal epidural lymphomas. Journal of Craniovertebral Junction and Spine (2011) 2(1): 3-11.
–Chelsea Marcus, MD is a third year resident in anatomic and clinical pathology at Beth Israel Deaconess Medical Center in Boston, MA and will be starting her fellowship in Hematopathology at BIDMC in July. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
Labs: the final frontier. These are the voyages of lab-techs everywhere. Our continuing mission: to explore strange new orders, to seek out new tests and new sero-preparations, to boldly notify floor clinicians about sample hemolysis for redraw…
Or at least that’s close enough to Gene Roddenberry’s vision for futurism in exploration—except instead of starships, we’re talking Star Labs. Happy 2018 Lab Week everybody, and thanks for checking back in!
Okay, so here’s something a little bit different. Different from my usual Zika or medical school posts, this piece is a celebration of several lab “truths” which I know many of us share. It seems like one of the overarching themes I’ve encountered regarding laboratory operation (and appreciation) is communication. Expectations and needs aren’t always communicated effectively across different medical disciplines and scopes. A while back I thought of 40 things every lab professional should know, but I’d like to expand on that a bit.
How many times have you said or encountered any of the following:
Why does the blue top have to be full, if the other ones weren’t as full?
I just put some blood from the lavender top into the tiger top—patient is a hard stick…
I’m checking on results for the patient in room 123…no, I don’t have their MRN…
There’s a trauma patient coming in via helicopter, I need crossmatched units before they’re here.
Can you please add on a serum lactic acid, there was a BMP from yesterday?
This C. Diff sample is solid…
Why are some hospitals’ rapid flu-tests done with just the swab of a swab kit, a little aliquot of saline from an IV push syringe, and a wasted no gel SST?
Are the results ready for the biopsy we did just now?
Do we have a critical value range for ESR?
We haven’t had an in-service on running POCT Glucose controls, so we haven’t done them yet
I didn’t want the tubes to leak in transit, so I used the labels as tape to keep the caps on!
In order to get SUPER GOLD STAR STROKE AND GOUT CENTER accreditation, we have to slash TATs by 40%
Captain Hematologist Jean Luc Picard (front) pleads with a clinician that only wants the WBC and H/H from a clotted CBC. Second Officer Riker (bottom left) smiles because he knows clots are dangerous for most analyzers. Lt. Operations Officer Worf (top right) agrees firmly for the sake of honor and quality assurance. An ensign trains on urinalysis (top left). [Source: StarTrekTNG]I’m sure by now you realize I could go on, and on, and on…There are always issues in laboratory medicine that don’t always translate well between floor clinicians and laboratory staff. It’s a tale as old as time. And, until we do develop universal translator technology, it will remain somewhat of a barrier to improving workflow. So how to we fix it? I argue it starts with Lab Week.
Lab Week is supposed to celebrate the clinicians, laboratory professionals, and ancillary staff that work diligently to produce results. Hundreds of thousands of laboratorians work throughout the country and are highly-trained, well educated professionals who use their expertise to diagnose and monitor treatments. Quality medical testing and exceptional care are part of the core values that each of us are celebrated for every year in April! Let me be clear, we are not support services for other clinical professionals—we’re all on the same team. Don’t be angered by the misinformed questions above, or by the stereotypes you might encounter in pathology, try and use them as teaching platforms within our community.
Capt. Hematologist Jean Luc Picard (right) takes endorsement from Chief Instrument Engineer Geordi LaForge (left) and while examining active Laboratory Data (center) speaks with clinical staff regarding temporary procedural changes for sending and holding PTT mixing studies while maintenance is being completed. [Source: Star TrekTNG]The whole point is that we’re in this together. Not just interdisciplinary teamwork that makes this year’s Star Lab theme so poignant, but teamwork across scopes. Those calls and messages we get in our managers’ offices or various bench top phones are part of our team too. It’s about the patients. We already know we contribute over 70% of clinical relevant information in every patient’s chart—some diagnoses like cancer rely completely on pathologist interpretation for screening, diagnosis, staging, and treatment recommendations.
While EMH Drs. Mark I and Mark II receive their “bad” results, it’s all part of a larger picture. As a note, “panic results” rarely illicit the expected reaction in the nurses and physicians we report them to. These doctors would think our current medical practice standards medieval, anyway… [Source: Star Trek Voyager]Here are a few examples of effective communication you could keep in mind.
For any Laboratory Professionals reading:
Instead of this: “Our policy is to reject clotted CBCs, we need a redraw, sorry.”
Try this: “While policy says to reject clotted CBCs, it’s not just because it could affect your PLT count. Other cell counts may be affected, and micro-clots can jam up the sensitive lines in the analyzers shutting them down for a while and affecting other patients’ results.” Try and realize that clinicians really do rely on those results! First and foremost, many clinical decisions are made on that last pending result for the next step of treatment. Whether it’s a PLT count or an acetone level, every result matters.
Instead of: “Room numbers aren’t adequate for patient and sample identification, sorry.”
Try this: “Because room numbers can change so quickly, we can’t use them to properly identify a specimen or patient. Do you have any of the following information…?” Understand that doctors, nurses, etc. aren’t always calling the laboratory from a private area. Thus, with so many people walking around a medical unit, a name might not be an option for them to use—room numbers are a sort of code for HIPAA compliance.
For any Clinicians reading:
Instead of this: “I really need you to rush that type and cross, quickly.”
Try this: “What can I do to help facilitate quicker turn-around for getting these units available for my patient?” Not only will you have started a conversation with the bench tech working on crossmatches, but you’ll demonstrate awareness of the complex process of safety/reportability blood bank goes through. Understand that Blood Bank is one of the more highly regulated aspects of laboratory medicine; FDA guidelines treat blood products as both a controlled substance and a tissue transplant, effectively.
Instead of this: “You have to run these samples because the patient is a hard stick.”
Try this: “What would be the minimum amount sufficient to run a particular test?” and if you need more information, simply ask! You’d be surprised how much the lab scientist on the phone would know about a particular testing method. Understand that QNS guidelines for specimens are not arbitrary amounts for the sake of covering repeats or mistakes in analysis. They are there to ensure quality results based on research and efficacy for a given instrument or method.
We all get angry. Especially at work, when our labs might be understaffed, overloaded, and dealing with instrument failures or evil advanced genetically modified arch-nemeses on the floors like Laboratory Manager Capt. Kirk (pictured). [Source: Star Trek the Wrath of Khan]So, it’s okay to get frustrated. It’s human. But I’ve got to tell you, I have been on both sides of this now—as a laboratorian and a clinician—and what I see time after time are simple gaps in communication. If we want to get better, not just for us, but for our patients, we should play an active part in helping close that gap.
I gave a few examples above, but how do we really change anything? My answer: interdisciplinary collaboration—and that’s not just a buzz word from my finishing LMU! If we want to really change anything, we should start it. If you’re a bench tech, start a discussion with your senior staff, supervisors, and managers about what you feel could be improved. If you’re a manager, seek out those barriers and be an active advocate for your staff—you’re already an advocate for the lab. If you’re a clinical pathologist, coordinate with your colleagues on the floor, develop more relationships, reach out for more than just consults on sign-outs.
Don’t be afraid to be a voice for change. Staff meetings, in-services, and self-aware improvement can be facilitated with good leadership, organization, and clear goals! Even if things look grim and you’re on downtime with a full ER, or stuck in the middle of a volatile asteroid field, noted barriers to improved communication will always GET RESULTS. [Source: Star Trek TNG]Want to change the knowledge gaps between clinical staff and laboratory staff? Hold an in-service or distribute messages with the missing information. When I was at Northwestern Medicine’s Blood Bank, I was an instructor once a month for nursing staff regarding blood products and transfusion protocols. We walked through the process with new nurses from proper phlebotomy and labeling, to order sets, to transfusion, to dealing with transfusion reactions. It was excellent! It was a great time to answer many questions and also gain insight into the clinical side of transfusion medicine.
Want to make sure no more sideways or crooked labels get sent to your specimen receiving stations? Instead of relying on the shear number of rejections to speak for themselves, discuss policy changes with your management, find the barriers to this change of specimen labeling, even send flyers out with “best dressed” tube images—it’s worked, I’ve seen it!
Want to make sure pathology stereotypes aren’t continued into the future? Change them! I plan to! Everyday I think of new ways to facilitate a new model of inclusion for pathologists into clinical healthcare teams. They’re an integral member already, why not reach past that tumor board, or biopsy report?
It takes a village to run a lab, or a space station. An interdisciplinary team is the only way healthcare can continue to improve. Shapeshifting flexibility, shrewd business deals, passion for quality assurance, creative license, and scientific knowledge are only as good as the teamwork they are a part of—even if you have religious emissaries on your staff. Sharing knowledge and effective communication are critical for labs, clinicians, and our patients. [Source: Star Trek DS9]The bottom line: if laboratorians want to grow and advance into the changing fronts within healthcare, we should take this opportunity during Lab Week 2018 and really embrace our profession as part of an interdisciplinary team. We deliver exceptional care and advocate for patients through our quality work in detecting, reporting, and preventing illnesses. I recommended laboratory professionals become more actively involved with fellow clinicians to directly improve patient outcomes. Let’s teach, let’s change policies, let’s have interdisciplinary rounds, let’s have roundtable discussions, let’s advocate together.
Because, after all, aren’t we advocating for the same thing: our patients.
Thank you! See you next time, and Happy Lab Week!
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student at the American University of the Caribbean and actively involved with local public health.
A 36 year old Caucasian male presented to the hospital with symptoms of a bowel obstruction. His past medical history was significant for a gunshot wound to the abdomen followed by the development of colon cancer with metastasis to the liver. Recently, he had an intestinal stent placed in order to relieve an obstruction from tumoral growth. During the current admission, he was taken to the operating room for a diverting colostomy and two days later developed a fever of 101.1°F and increasing abdominal pain. Due to a concern for sepsis, blood cultures were collected and piperacillin-tazobactam was added to his antibiotic therapy regimen which already included vancomycin and ciprofloxacin.
Laboratory Identification
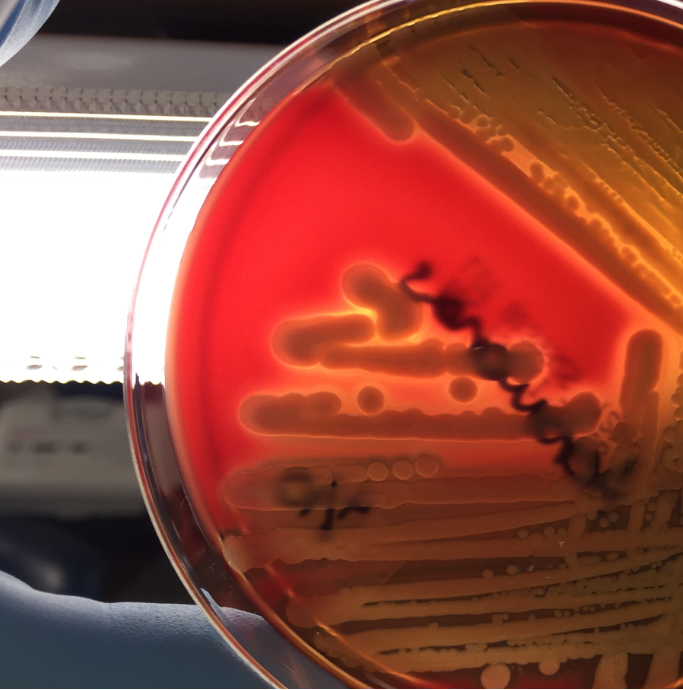
Image 1. Gram stain from the blood bottle showing many gram negative rods (100x oil immersion).Image 2. The organism grew as mucoid colonies on blood, chocolate and MacConkey agars after 24 hours of incubation at 35°C in 5% CO2.
Image 3. The organism exhibited beta hemolysis on blood agar when held up to a light source.
The blood culture signaled positive after less than 24 hours on the automated instrument and Gram stain revealed gram negative rods (Image 1). The organism grew as mucoid colonies on blood, chocolate and MacConkey agars after 24 hours of incubation at 35°C in 5% CO2 (Image 2). When the blood agar plate was examined with a light source, the organism clearly illustrated beta hemolysis (Image 3). Rapid biochemical testing was positive for catalase, oxidase and indole. The Vitek II identified the isolate as Aeromonas veronii bv. sobria.
Discussion
Aeromonas spp. are facultative anaerobic gram negative rods. They are inhabitants of aquatic ecosystems and as such can cause wound infections in people exposed to polluted lakes or brackish water with fresh breaks in their skin. Additionally, gastroenteritis is common with Aeromonas spp. and are often acquired through ingestion of unpurified water or to a lesser extent by consumption of contaminated meats, fresh produce or dairy products. Extraintestinal infections, including sepsis and meningitis, can result by spread from GI sources or wound infections. Interesting, medicinal leeches, used in the post-operative setting to increase blood flow to the surgical site, are colonized with Aeromonas spp. (most commonly Aeromonas veronii bv. sobria) and can result in systemic infections in the patient.
In the laboratory, Aeromonas spp. grow readily from stool, wound and blood sources on commonly used media and exhibits beta hemolysis on blood agar. In addition, Aeromonas spp. will grow on CIN agar (at room temperature as well as incubator temperature) as colonies with a pink center surrounded by a white apron and are indistinguishable from Yersinia spp. Aeromonas spp. is positive for catalase, oxidase and indole by rapid testing. In most cases, identification of Aeromonas spp. to the complex level can be accomplished by biochemical testing (esculin, VP), automated instrumentation or MALDI-TOF mass spectrometry. The three clinically relevant complexes include: A. hydrophila complex, A. caviae complex and A. veronii complex.
With regards to susceptibility testing for Aeromonas spp., the CLSI M45, 3rd edition provides guidelines for the three complexes discussed above. Third or fourth generation cephalosporins, fluoroquinolones and trimethoprim-sulfamethoxazole are recommended as antibiotics for primary testing for isolates from extraintestinal sites. Aeromonas spp. are uniformly resistant to ampicillin, amoxicillin-clavulanate and cefazolin and many strains may possess various inducible beta lactamases.
In the case of our patient, with the laboratory identification of Aeromonas veronii bv. sobria, his gram negative coverage was switched to ciprofloxacin for a 10 day course. His PICC was removed and on further imaging studies he was found to have a large abdominal abscess which required surgical drainage. Subsequent cultures from the abdominal abscess were negative.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the director of the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement, and resident education.
In Seattle, Pike Place Fish Market is nearly synonymous with the Pike Place Market. Tourists and locals stand and watch the fish mongers fill orders by throwing fish around the stand. Everyone, including the employees, laughs and enjoys the atmosphere. This is where the FISH! Philosophy was born. FISH! is a leadership training method that focuses on four concepts to increase collaboration and excitement about work:
Choose your attitude
Be present
Play
Make someone else’s day
These concepts are not mind-blowing, and this is exactly why they’re effective. They are easy to remember and easily integrated into daily practice, whether you are a teacher,a an office worker, or a laboratory professional. Becoming an effective and productive employee starts with choosing your own attitude. For example, when you choose the attitude of empowerment, support, and kindness, you start enacting them. In other words, you become kinder and you support and empower others more easily. As an experiment, I recently said to myself “I am energized and excited” when I was feeling the complete opposite. I started it as more of a joke, to be honest, but the interesting thing is that within twenty minutes, I actually became energized and excited. The power of our attitude is immense and we can all use it to our own and others’ benefit.
To be present is not an easy task. We are often pulled in many different directions, whether professionally or personally. Sometimes we can only think about work when we are at home, or we want to be at home when we are at work. The power of being present comes from acceptance; accepting that we are at work frees us from the resistance that is sapping our energy if we are mentally at home. We have all had conversations where someone wasn’t quite present and we can all remember how frustrating that was. On the other hand, having a conversation with someone who is present makes us feel important, appreciated, and empowered.
Work can be a serious place, especially when lives are at stake. However, there are always moments of play possible, even if it is during breaks or at lunch. If we focus on making someone else’s day, not only do we create a happier work force, we become happier ourselves. We all know how good it feels to make someone laugh, to make someone feel cared for. Perhaps it is something small, like asking if you can bring someone a coffee when you are running out to get one. Or perhaps you leave them a nice note or do a small task for them to make their day easier. I have a notepad with “Awesome Citations.” It is a simple note that I fill out and I hand to someone each week. Making someone’s day does not have to be big or extravagant. It is often the small gestures that people remember.
So go out and be present, while choosing your attitude. Play a little at work to make someone’s day. The simple acts we take every day can transform an entire department and organization. So why not throw some fish and have some fun?
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
My story begins many decades ago when I was working in the laboratory at Bronson Methodist Hospital in Kalamazoo, Michigan. While my favorite departments were Blood Bank and Hematology, I had the honor of working with Joie Vine and Dr. Hubbard, the supervisor and chief pathologist, respectively, of the microbiology department. Microbiology was my least favorite department, but luckily for me, Dr. Hubbard discovered early on that I loved to learn. Dr. Hubbard was small in stature, yet large in leadership skills. He knew when to be serious and when to be light-hearted. That attitude permeated the lab. Dr. Hubbard made it possible for me to go to the AABB conferences and U-Hospital (University of Michigan) for specialized training. As a lab professional, I was living the dream!
It was spring when Joie told me she was going on vacation and was short-staffed. She asked me to fill in for her during the lunch hour for one week, which would allow her staff to go to lunch. I said yes. Everyday Dr. Hubbard would check in with me on his way to and from lunch. By Thursday, I was really missing Blood Band so I decided to have some fun. When Dr. Hubbard stopped by microbiology, I opened a feces container. I look at him and said, “hmmm, looks like feces,” held it to my nose, “smells like feces,” and with my finger, I scooped a little and placed it in my mouth. I proclaimed, “it tastes like feces!” He was in total shock. After a brief moment I burst into laughter and so did he! I had placed peanut butter in the feces container!
So if you’re thinking you can’t apply the Fish Philosophy to the clinical laboratory environment, remember, we “Choose our Attitude every day.” It feels good to “Be There” when a friend needs us. I’ll always remember when Dr. Hubbard said that “I Made His Day!” because we took a break from our serious work and played!
Catch the Energy — Lab Professionals are Fun People!
-Catherine Stakenas, MA, is the Senior Director of Organizational Leadership and Development and Performance Management at ASCP. She is certified in the use and interpretation of 28 self-assessment instruments and has designed and taught masters and doctoral level students.