Case History
A 42 y/o female G2P2002 patient presented to her Ob/Gyn for Colposcopy for monitoring of persistent High-Risk HPV. She was originally found positive for HPV in 2015, but has had never had a Pap with a squamous intraepithelial lesion, abnormalities on colposcopy, or dysplasia seen on endocervical curettage. Additionally, she endorsed a complaint of vague diffuse pelvic/lower abdominal pain for approximately the last 2 months. She states that the pain is mild and comes and goes and is not associated with anything in particular. She has noticed some clear to gray-white discharge now and then since she first noticed the pain, but nothing that really worried her. Pt denies changes in bowel or bladder habits, denies nausea, fever, or chills. Pt has been in a monogamous relationship with her partner for the last 12 years. She had a Mirana IUD placed 4 years prior, without complication, and has not had menses since placement. Prior to that, the patient had normal, regular cycles. She has 2 children with the same father, both were delivered by spontaneous vaginal delivery without complications. She has mild anxiety and depression for which she is treated, but no other medical problems. There is no surgical history. She has 1-2 glasses of red wine every week, denies tobacco use, and denies illicit drug use.
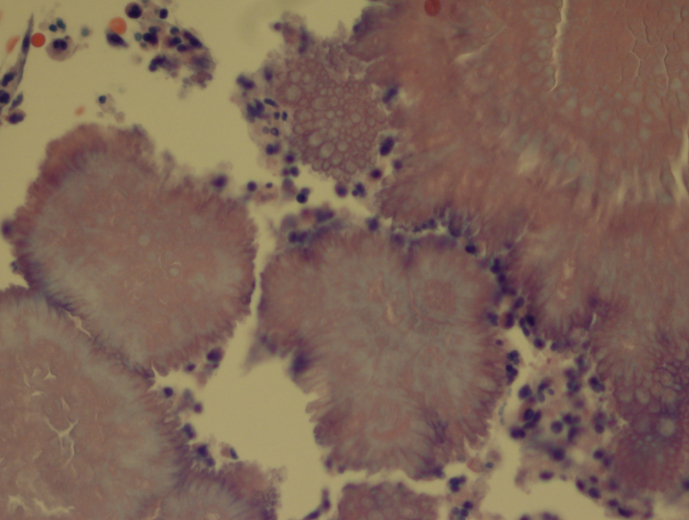
Pelvic exam revealed a benign appearing cervix that was not painful to touch or motion. There was a clear to white mild discharge that was suspected to be normal vaginal secretions. IUD strings were noted. Colposcopy revealed an easily appreciated transformational zone without any obvious lesions. A routine endocervical curettage (ECC) was performed followed by observed increased clear discharge from the cervical os. ECC was sent for routine pathology:

Discussion
Actinomycosis is an infection by a species within the Actinomyces genus, generally seen in dental and other oropharyngeal abscess formations. However, rare occurrences of pelvic Actinomycosis can be seen in women with intrauterine devices in place. Pelvic infections can result in cervicitis and endometritis and progress into abscess formation within the fallopian tubes and the ovaries along with salphigitis. The more profound disease consisting of abscess formation generally presents with fever, specific lower abdominal tenderness, and elevated WBCs, thus can mimic acute appendicitis, ovarian torsion, or ectopic pregnancy (1). The first case reported in the literature was in 1967 (2).
Three main species of Actinomyces have been found to be associated with IUD-associated pelvic infection: A. naeslundii, A. odontolyticus (3), and A. hongkongensis (4). All of these species are obligate to facultative anaerobes, catalase negative, and nitrate reducing. A sub-species group of A. naeslundii, however, can be catalase positive and is CAMP test-positive. All members of A. naeslundii are urease positive while A. odontolyticus and A. hongkongensis are urease negative.
References
- Joshi et al. Pelvic Actinomycosis: a Rare Entity Presenting as Tubo-ovarian Abscess. Arch Gynecol Obstet. 2010, 281:305-306.
- Brenner et al. Pelvic Actinomycosis in the Presence of an Endocervical Contraceptive Device. Obstet Gynecol. 1967, 29: 71-73.
- Woo et al. Diagnosis of Pelvic Actinomycosis by 16S ribosomal RNA Gene Sequencing and its Clinical Significance. Diagnostic Microbiology and Infectious Disease. 2002; 43: 113-118.
- Flynn et al. Identification by 16S rRNA Gene Sequencing of an Actinomyces hogkongensis Isolate Recovered from a Patient with Pelvic Actinomycosis. J. Clin. Microbiol. 2013, 51(8):2721. DOI: 10.1128/JCM.00509-13.
-Jeff Covington, MD, PhD, is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
