I volunteered in April 2019 in Tanzania at the Kilimanjaro Christian Medical Center. I was there specifically to teach breast mastectomy grossing. There are two pathologists at KCMC, Dr. Mremi and Dr. Patrick, but finding time in their schedule to work with them proved to be the biggest challenge. The pathologists have many responsibilities outside of just looking at slides. Dr. Alex Mremi is the head of the department, but he also teaches at the medical school and meets with medical students. The pathologists at KCMC perform autopsies, including the forensic autopsies that would normally be sent to a medical examiner or coroner’s office in the United States. Dr. Mremi was pulled away one day to do an autopsy and two other days to go to court to discuss autopsy findings. One of the days Dr. Mremi also performed an FNA, where he was not only preparing the slides, but procuring the specimen from the patient himself.
In the end I was able to go over one mastectomy case with each pathologist, but I had hoped to discuss my case study examples and talk to them about the differences in our grossing techniques in greater detail. When the pathologists were busy I would go over grossing techniques of the less complex specimens with the lab aides that perform grossing. Unfortunately the lab aides have responsibilities as accessioner, histotech, grossing aide, transcriptionist, etc. They do it all, so it was equally difficult to find time in their busy schedule. In addition to scheduling conflicts, there was also the issue of ventilation in the gross room. Because there is a window fan, but not proper ventilation, whoever is grossing could only be in the gross room for a limited amount of time before formalin exposure would be too much. I did bring a formalin 3m mask that was donated by a colleague of mine with some replacement cartridges that I hope they will implement into their routine.
In retrospect I wish I had known how difficult it would be to schedule my grossing time with both the pathologists and the lab aides. It takes a forceful and persistent personality to wrangle people into the gross room when they are bogged down with their other work. I wish I had known about this blog before my trip to Tanzania because this seems to have been previously stated by PAs. I would also recommend that the PA make sure to have all their transportation arrangements and initial appointments at the hospital set up in advance because you will essentially be dropped in a place with no Wi-Fi. I made sure to arrange all of this with the help of Alpa Pandya, Dr. Milner’s assistant, who was incredibly helpful. If you are able to exchange money in advance or schedule a trip to the bank with your airport driver this will be very helpful. The day I arrived was a Sunday so banks were closed. It was somewhat of a challenge to find a restaurant or local transportation that would take US dollars. I would recommend getting your visa before your trip because this may prove difficult to accomplish at the airport upon arrival. Be sure to get all the recommended vaccines and anti-malarial medicine if necessary in the area you are travelling. I was very surprised to see no mosquitos at all during my entire trip and find out that malaria is nearly eradicated in the Kilimanjaro region. I also had my clothing sprayed with an anti-bug spray that may have helped keep flies away from me. I would recommend people learn basic phrases (hello, thank you, please, etc.) in the language of the country they are visiting to be more respectful of the local people. Language apps such as Duolingo or Babel are a great help.
I recommend that if a PA is volunteering in a low resourced setting they find out exactly what would be most beneficial to the pathology department in that setting. Since my trip was more focused on breast mastectomy grossing I brought Lester, breast diagrams, templates, inking diagrams, breast protocols and procedures from my hospital, as well as multiple case examples. Some of which I laminated in advance so they could be used again and again in this setting. If I were to volunteer again I would try to set up a more concrete schedule in advance with exact times blocked out to discuss techniques, be in the gross room or give presentations. I am incredibly grateful I got to have this experience, I only wish I was able to make more of an impact. I hope that more PAs will continue to volunteer and that pathologists will participate in the telepathology volunteer roles to free up more time for the few pathologists in these low resource environments. Thank you again to ASCP, Dr. Milner and Alpa for this opportunity!
-Faith Fletcher is a Pathologists Assistant at Henry Ford Hospital in Detroit, Michigan.
An 8 year old male with no significant medical history
presented with left knee pain and swelling for one week. Physical examination
revealed a temperature of 101.2°F and a left swollen, tender knee with reduced
range of motion. A joint aspirate was performed, and synovial fluid and blood
were sent for microbiological analysis.
Laboratory Findings
Synovial fluid analysis showed increased neutrophils, a
nucleated cell count of 90,840 cells/cmm, and no crystals.
Blood cultures were negative. Gram smear of the joint fluid
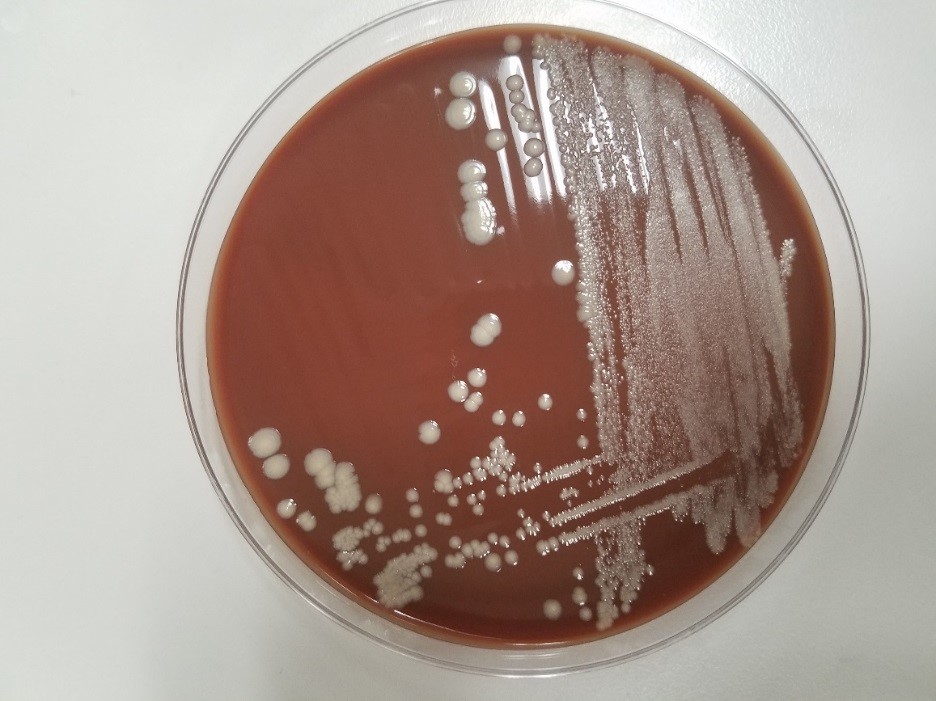
showed many neutrophils and no bacteria. Fluid culture grew convex tan-yellow
colonies on blood and chocolate plates at 48 hours (Image 1). Gram smear
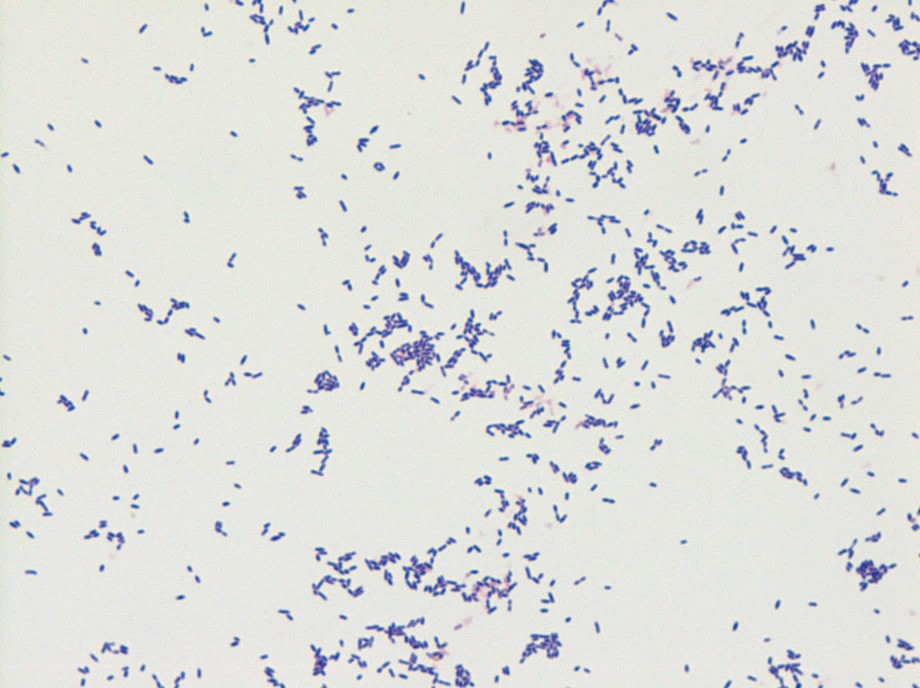
revealed gram-negative cocci (Image 2). The organism was identified by
MALDI-TOF as Aggregatibacter aphrophilus.
Antibiotic susceptibility testing showed susceptibility to augmentin,
ampicillin, ceftriaxone, and levofloxacin.
Image 1. Growth on anaerobic chocolate plate.Image 2. Gram stain from anaerobic culture showing gram negative cocci.
Discussion
Aggregatibacter
aphrophilus is a gram negative coccobacillus that requires 5% CO2 and grows
best on blood agar. It is oxidase negative and catalase negative. It is
categorized as a HACEK organism, being a cause of culture-negative
endocarditis. It is considered normal oral flora, and dental procedures can be
a source of infection. Aggregatibacter endocarditis
can cause a positive P-ANCA and be misdiagnosed as a vasculitis. It has also
been reported as causes of sacroiliitis, bartholinitis, endophthalmitis, and
brain abscesses. Treatment is generally ceftriaxone for 8 weeks. Identification
is by biochemical methods or MALDI-TOF. Broad range PCR (br-PCR) has also been
described, which targets a highly-conserved region of 16S rDNA, and then
compares the sequences to database sequences.
The patient was given cefazolin, and his temperature
downtrended. He was discharged prior to results but placed on oral augmentin.
After susceptibility testing, infectious disease was consulted and he was
placed on ceftriaxone for 8 weeks. He continued to improve and subsequent
cultures were negative.
References
Ratnayake L, Olver WJ, Fardon T. Aggregatibacter
aphrophilus in a patient with recurrent empyema: a case report. J Med Case Rep.
2011;5:448. Published 2011 Sep 12. doi:10.1186/1752-1947-5-448
Hirano K, Tokui T, Inagaki M, Fujii T, Maze Y,
Toyoshima H. Aggregatibacter aphrophilus infective endocarditis confirmed by
broad-range PCR diagnosis: A case report. Int J Surg Case Rep. 2017;31:150–153.
doi:10.1016/j.ijscr.2017.01.041
-Jonathan Wilcock, MD is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
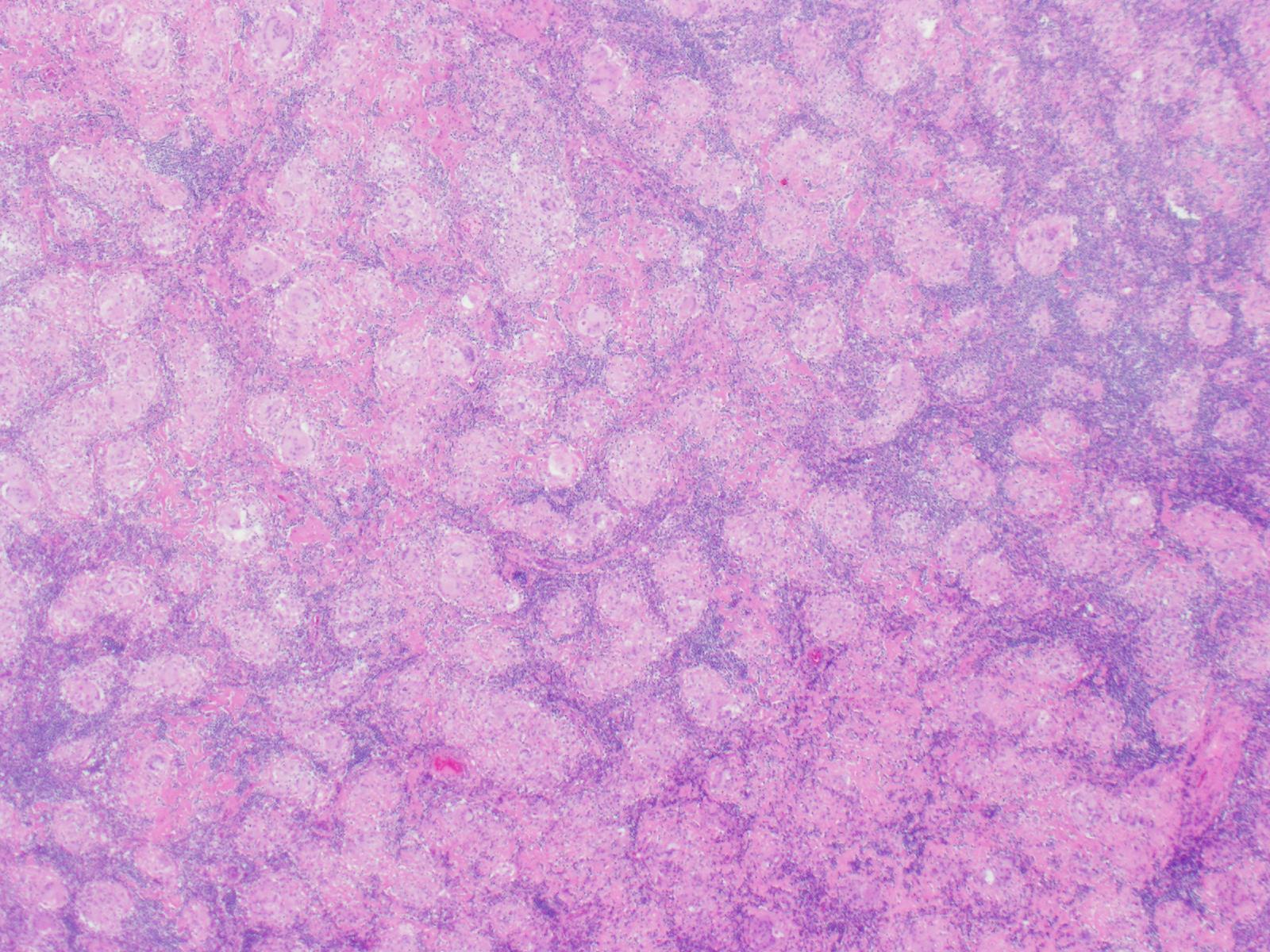
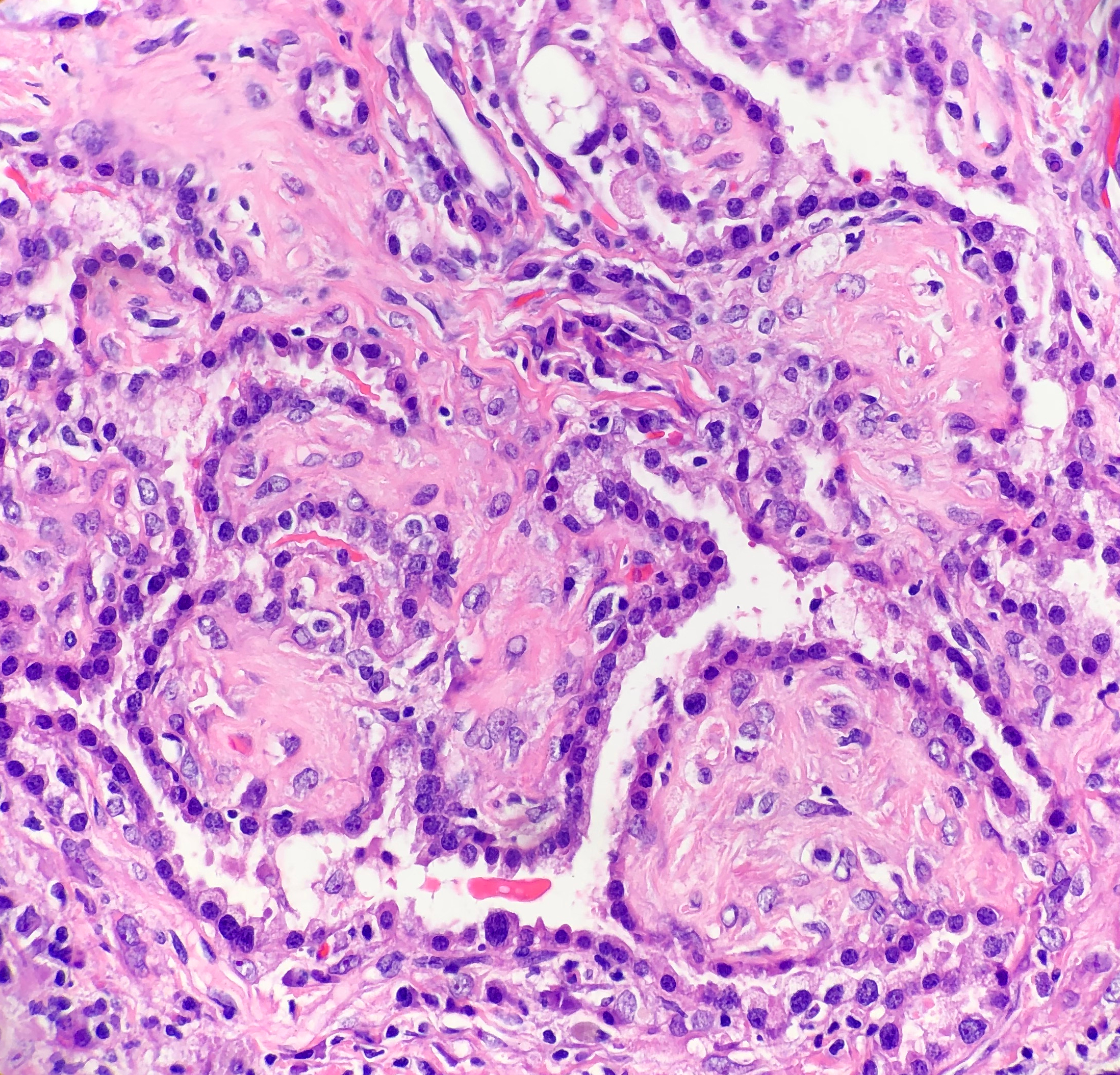
A 36 year old female underwent thyroidectomy for multinodular goitre that led to the fortuitous discovery of a neck mass. The neck mass specimen submitted comprised two lymph nodes measuring 2.2 cm and 1.3 cm in the greatest dimensions, with a fleshy tan cut surface.
Biopsy Findings
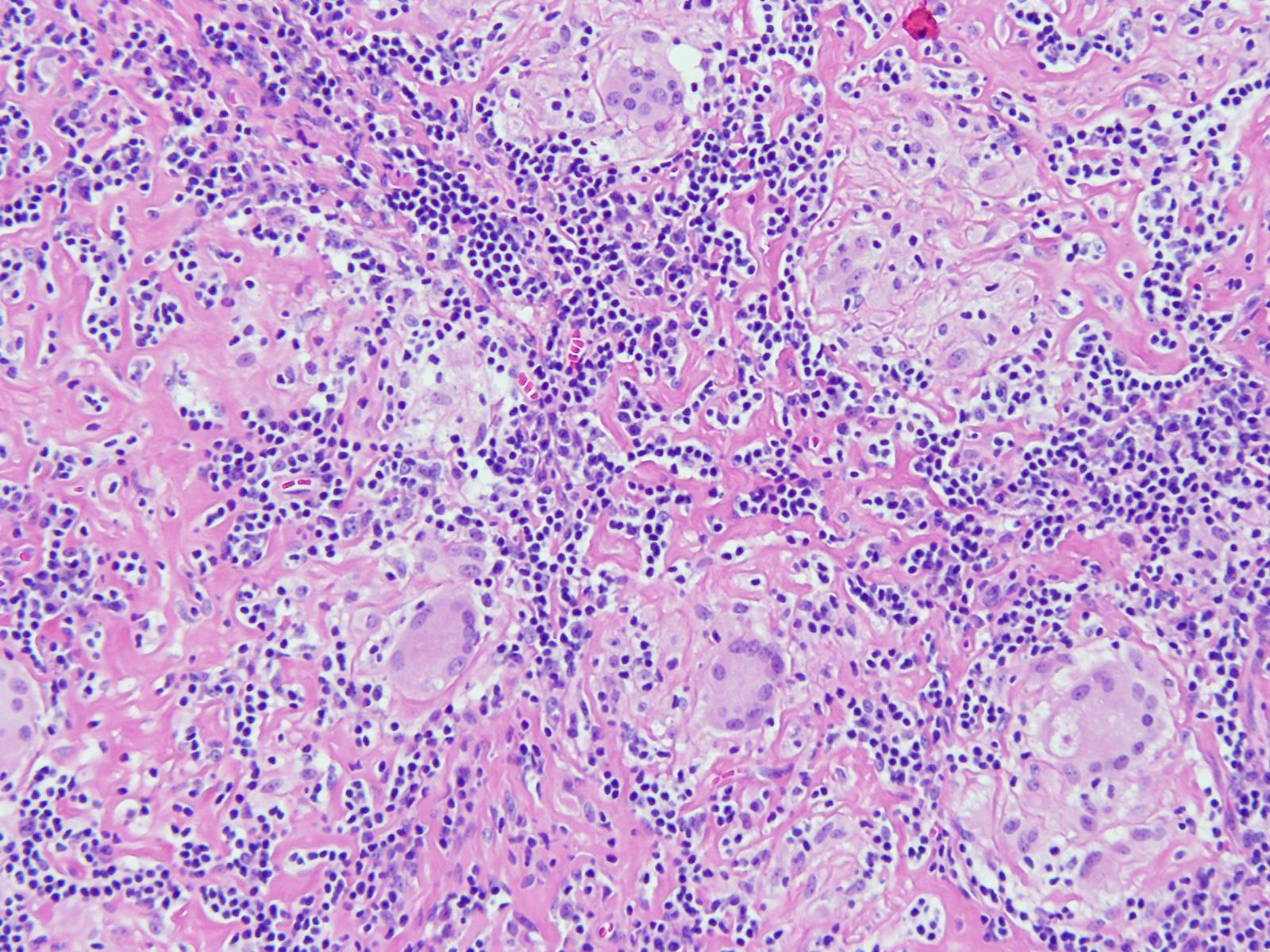
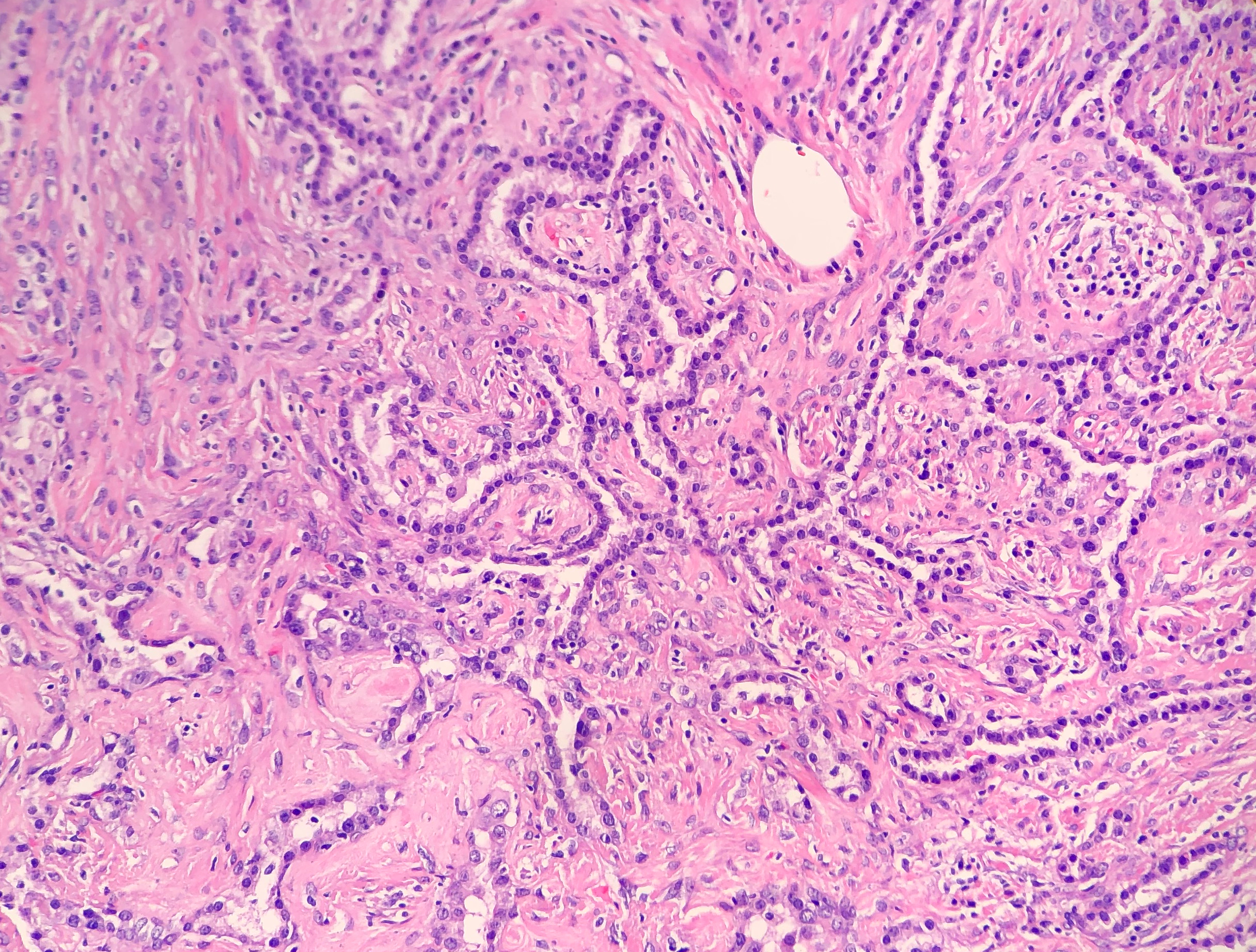
H&E stained sections revealed numerous non-necrotizing
granulomas effacing and replacing normal lymph node architecture. These
consisted of pale epithelioid histiocytes and Langhans type of giant cells. The
granulomas lacked a peripheral rim of lymphocytes. AFB and GMS stains were
negative for microorganisms
Diagnosis
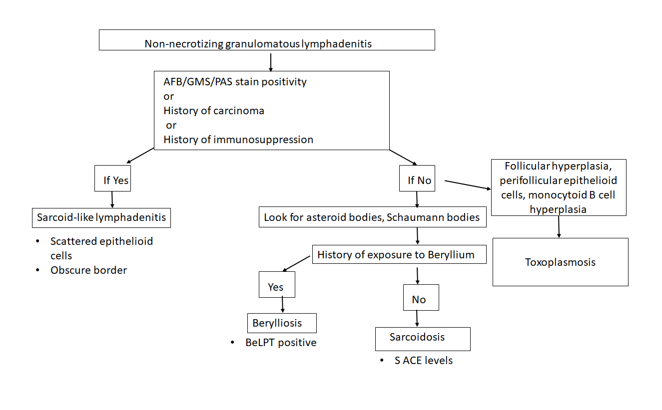
A diagnosis of non-necrotizing granulomatous
lymphadenitis was rendered noting that in the correct clinical context the
findings could represent sarcoidosis.
Discussion
Granulomatous inflammation is a special type of
chronic inflammatory response characterised by the formation of discrete
collections of histiocytes called granulomas. Activated histiocytes appear as
epithelioid cells with round to oval nuclei, often with irregular contours and
abundant granular eosinophilic cytoplasm with indistinct cell borders. They may
coalesce to form multinucleated giant cells. When found in the lymph node, the
reaction pattern is called granulomatous lymphadenitis. It can be caused by a
variety of different conditions, and therefore, requires thorough workup to
come to a conclusive diagnosis.
On the basis of presence or absence of necrosis,
granulomatous lymphadenitis can be classified as necrotizing or non-necrotizing.
Additionally, the presence of an abscess, usually central, indicates a
suppurative lymphadenitis.
Non-necrotizing
granulomatous lymphadenitis:
Sarcoidosis lymphadenitis is
the prototype of non-necrotizing granulomatous lymphadenitis. It shows the
presence of discrete granulomas without a peripheral rim of lymphocytes, called
“naked granulomas”. The early phase shows follicular hyperplasia and sinus
histiocytosis, followed by appearance of epithelioid cell nodules toward the
end of this phase. The peak phase shows well-demarcated
granulomas composed of epithelioid cells with scattered multinucleated giant
cells observed throughout the lymph node. Granulomas may occasionally coalesce.
In the late phase, increased collagen fibers result in fibrosis and
hyalinization. There are no neutrophils and it is uncommon to find small
foci of central necrosis. Numerous inclusions such as asteroid, Schaumann, or
Hamazaki-Wesenberg bodies can be seen. In this case, we observed
well-demarcated granulomas throughout the lymph node, typical of the peak phase
without any caseous necrosis or suppuration.
Other causes of granulomatous lymphadenitis can be ruled
out as follows.
Sarcoid-like lymphadenitis:
It shows a similar pattern of non-necrotizing
lymphadenitis like sarcoidosis. However, classically sarcoid like reaction
shows scattered small epithelioid granulomas with sparsely arranged epithelioid
cells. The border of the granulomas is usually obscure. The CD4:CD8 ratio
ranges from 0.8 to 2.25 while in sarcoidosis, it is >3.5. These findings
help distinguish sarcoid-like lymphadenitis from sarcoidosis.
Sarcoid-like adenitis may be seen in numerous conditions
such as carcinoma, Toxoplasmosis, fungal infections, tuberculosis,
immunocompromised states, pneumoconiosis etc. The fact that tuberculosis and
fungal infections can present with a non-necrotizing granulomatous lymphadenitis
highlights the importance of performing fungal (PAS & GMS) and AFB (Ziehl
Neelson) stains in non-necrotizing lymphadenitis as well. In this case, the
granulomas had distinct borders, numerous epithelioid cells, no organisms were
identified on special stains, nor was there any history of immune compromise;
ruling out a sarcoid-like reaction.
Berylliosis: The lymph node picture in Berylliosis is identical to that of sarcoidosis.
We may even see asteroid bodies or Schaumann bodies. A diagnosis can be
established by eliciting a history of chronic exposure to Beryllium. Beryllium
lymphocyte proliferation test (BeLPT) is a test that measures Beryllium
sensitization and is very specific for Beryllium exposure. There was no known
history of exposure to Beryllium in this case.
Toxoplasmosis: A classic triad of follicular hyperplasia, small granulomas composed of epithelioid cells within and around hyperplastic follicles and, monocytoid B cell hyperplasia, is observed in toxoplasmosis lymphadenitis. This case did not show follicular hyperplasia, ruling out toxoplasmosis.
Necrotizing granulomatous lymphadenitis
Even though we did not find any necrosis in this case,
yet, it is worthwhile to review briefly the various causes of necrotizing lymphadenitis.
Non-suppurative
Tuberculosis: Histology
of a tuberculous lymph node is characterised by central caseous necrosis
surrounded by an epithelioid cell layer. The outermost layer is comprised of
lymphocytes and fibrosis. Plasma cells are not observed. Diagnosis can be
established by performing an AFB stain that demonstrates acid fast rod shaped
bacteria in the areas of necrosis. Organisms can also be detected by PCR.
BCG lymphadenitis:
About 0.7 to 2.3% of BCG vaccinated children may develop BCG lymphadenitis that
is smaller than tuberculous lymphadenitis. Early phase shows follicular
hyperplasia and sinus histiocytosis. Later, there is development of
micronodules of epithelioid granulomas without necrosis and epithelioid cell
granulomas with central caseous necrosis. Langhans giant cells are rare.
Fungal infections:
Fungal infections by Histoplasma, Cryptococcus, coccidiodomycosis, pneumocystis
may also cause a necrotizing granulomatous inflammation. There are numerous
neutrophils, and fungal structures can be seen. GMS and PAS can be used in
cases where it is difficult to the find the fungal elements on H&E.
Suppurative
Tularemia: There
are three forms of histological changes, Abscess form, showing abscess
with central necrosis and mononuclear cells, Abscess-granulomatous form with granulomas with central necrosis,
which form large lesions with central abscesses, and granulomatous form with
caseating necrosis at the centre of the granulomas.
Cat Scratch disease:
Similar to tularemia, there are three phases of histologic presentation, an
early phase of follicular hyperplasia, intermediate phase of microabscess, and
a late phase of granulomatous inflammation. Monocytoid B cell clusters are
observed close to the abscess.
Conclusion
Sarcoidosis is usually diagnosed by
excluding other causes of granulomatous inflammation, as we did in this case.
Characteristic non-necrotizing, discrete granulomas were seen throughout the
lymph node. The age of the patient and female gender epidemiologically support
the diagnosis. This case reflects an example work up of a granulomatous
lymphadenitis that is a morphologic presentation of myriad diseases.
-Swati Bhardwaj, MD has a special interest in surgical pathology and hematopathology. Follow her on Twitter at @Bhardwaj_swat.
–Kamran M. Mirza, MD, PhD, MLS(ASCP)CM is an Assistant Professor of Pathology and Medical Education at Loyola University Health System. A past top 5 honoree in ASCP’s Forty Under 40, Dr. Mirza was named to The Pathologist’s Power List of 2018. Follow him on twitter @kmirza.
Kumarasen Cooper, MD, PhD completed his medical training
from his home country in South Africa and his PhD at Oxford. He now works as a
surgical pathologist at the University of Pennsylvania and is responsible for
leading the initiative to engage the pathology department in the Botswana-UPenn
partnership through the Perelman School of Medicine Center for Global Health. He
has over 260 publications and has lectured in 5 continents. Despite this busy
schedule, Dr. Cooper devotes two separate months of the year to work in
Botswana’s only academic pathology department, where he pours his energy into
helping the department advance.
I met Dr. Cooper through email when I heard about the work
he was doing in Africa. He generously agreed to come visit my department to
give an excellent Grand Rounds lecture on his experiences working in Global
Pathology, and he led a much-appreciated resident slide session of unusual and
difficult cases from his work in Botswana. Humility and grace envelop Dr.
Cooper despite his brilliant accomplishments. He also proved to be incredibly
generous with a refusal of his speaker honorarium, in exchange for an agreement
that we would collect pathology textbooks to send to the under-supplied
residency program in Botswana. I’m excited to share the inspiring work that he
does through the Botswana-UPenn partnership with all of you today, as I think
this program could be used as a model for all institutes to involve their
pathology departments in global health opportunities.
Q: What began your interest
in global health?
A: I was born,
raised, and completed my medical training in South Africa. I spent 15 years
working as a Pathologist and served as the Chair of Pathology in Johannesburg
until I was recruited to the US to work as Vice-Chair at the University of
Vermont. I knew when I left Africa that I would always come back, and that I
could use what I learned abroad to give back in some way. I wasn’t sure in what
form that would take at the time, but I knew there was work that still needed
to be done. This was also influenced by my visits to the pathology departments
in many different countries over the years…I was able to gain a sense of the
‘haves and have-nots’, and so developed a strong feeling that I needed to give
back.
A: When I first discovered
the partnership, I thought that this may be an avenue for me to participate in
global pathology. At the time, the pathology department was not involved in any
of the ongoing BUP projects, though other clinical departments at UPenn were. After
my initial assessment of the Botswana pathology department and its resources in
April of 2016, I was able to identify ways that I could help. Together with the
Director of BUP, I approached the Chairman of my department with the proposal,
and we started the pathology partnership program in October of that year. Since
then, I travel to Botswana twice a year for one month at a time, and each time
I take 1-2 residents from UPenn along with me.
Q: Can you describe
the pathology department in Botswana?
A: To serve a
population of just over 2 million people, Botswana has only one academic
pathology department, a College of the University of Botswana (UB) School of
Medicine, which consists of six pathologists who
are all from other countries. There are currently no Botswana pathologists
working in the department. There are about six technicians working in the
laboratory, all of whom were trained internationally. The laboratory receives
around 7,000 surgical specimens yearly, plus cytology, and autopsy. They work
with an extremely limited panel of immunostains that are not routinely used but
are spared for the rare case that cannot be diagnosed with morphology alone.
The residency program is still very new. There are six
residents in the program at the present time, and the program is designed so
that they will spend the first two years in Botswana and then they will
continue their final years of training in South Africa. I look forward with
anticipation to the first Botswana trained pathologists in the country.
Q: What is your role
when visiting Botswana?
A: We try to help
with everything we can. I sign out cases with the residents during the time I
am there, and I teach the residents using these cases every day. The UPenn
residents that I bring with me are eager to teach as well, so they deliver
didactics regularly also. We all participate in tumor boards and the FNA
clinic. We each take on projects that we can partner with them to tackle…things
like improving turnaround time, quality improvement, and SOP preparations. We also work on developing academic programs, grossing
templates and manuals (A UPenn pathology PA spent two weeks working in Botswana
on this project), synoptic reports, cancer guidelines…anything they need I try
to help them with.
Q: How are the UPenn pathology
residents given credit in their home program to join you?
A: As of this
year, the BUP pathology program is now offered as one of the official electives
that residents are allowed to choose from. They are able to use elective time
and their travel expenses are paid for by a resident travel grant.
Q: In your role as
supervisor of the UPenn residents, what do you see the residents gaining from
the experience?
A: The residents
that have come with me to Botswana are very compassionate and are eager to
contribute in any way they can. Experiencing pathology in Botswana, where
people are trying to achieve so much with so little resources, it makes the
UPenn residents even more grateful for all of the resources they have available
to them. They also have the opportunity to not only learn from the unusual
cases that present in Botswana, but also the opportunity to contribute their
own unique set of skills – some have focused on teaching autopsy technique,
others give enthusiastic and detailed
lectures, and one gave a talk about successful study techniques. [For more
information about the resident experience, one can read more about it in the UPenn
blog here: https://pathology.med.upenn.edu/department/blogs/residency-matters/penns-pathology-residency-program-reaches-botswana]
Q: How do you see the
BUP pathology partnership affecting the trainees in Botswana? What changes have
you seen since you started working with them?
A: The residents in
Botswana really appreciate the partnership that we have formed. I have seen the residents develop so much
since working with them. At first, they were reserved and now they actually
request lectures on topics they feel they could improve on. They are still very
humble and respectful, but I have encouraged them to be advocates for
themselves. They have really embraced their program and I’m very proud of them.
We have a deep appreciation for each other and are proud of what we have
achieved together.
We’ve also started hosting Botswana residents at UPenn for a
one month rotation so they have the opportunity to supplement their training
even further. We fly them to the US, house them, and include them in our
residency training program for the month. They have the opportunity to sit in
on sign-outs, shadow grossing and autopsy, attend conferences, and be exposed
to the advanced testing that we routinely perform in the US.
Q: How do you see the
pathology partnership growing in years to come?A: I’m currently helping them find placements in
South Africa or possibly partnering with private laboratories to help expose
the residents to a greater diversity and volume of cases. As the program
continues to grow, we look forward to seeing the fruits of the partnership for
many years to come.
-Dana Razzano, MD is a Chief Resident in her third year in
anatomic and clinical pathology at New York Medical College at
Westchester Medical Center and will be starting her fellowship in
Cytopathology at Yale University in 2020. She was a top 5 honoree in
ASCP’s Forty Under 40 2018 and was named to The Pathologist’s Power List
of 2018. Follow Dr. Razzano on twitter @Dr_DR_Cells.
The patient is a 43 year old woman who experienced chest congestion and presented to her local physicians office. A chest X-ray was ordered and demonstrated a lung abnormality. A follow-up CT scan confirmed a 1.9 cm smoothly marginated nodule in the upper lobe with no adenopathy and a normal liver and adrenal glands. The nodule was mildly hypermetabolic on PET scan. A bronchoscopy was performed, which was non-diagnostic. Two subsequent CT scans demonstrated no change in the size of the nodule. Overall, the patient feels well and denies cough, hemoptysis, dyspnea on exertion, and weight loss. Due to the suspicion of cancer, the patient has decided to undergo a lung lobectomy.
Diagnosis
Received in the Surgical Pathology lab for
intraoperative consultation is a 30.0 x 7.2 x 2.2 cm lung lobectomy specimen. There
is an attached 6.2 cm staple line, which is removed and the subjacent resection
margin is inked blue. The entire pleural surface is inked black. The specimen
is sectioned revealing a 2.1 x 1.7 x 1.0 cm white-tan, firm, round nodule that
is 0.5 cm from the blue inked resection margin and 0.2 cm from the black inked
pleural surface. The remainder of the specimen is composed of red-tan, spongy,
grossly unremarkable lung parenchyma without nodules or other lesions.
Photographs of the specimen are taken (Figure 1). A representative section of
the nodule is submitted for frozen section and read out as “diagnosis
deferred”. Representative sections of the specimen are submitted as follows:
A1FS: Frozen
section remnant
A2-A7:
Nodule, entirely submitted
A8-A10: Grossly unremarkable lung parenchyma
Immunohistochemical stains show the epithelial cells in the lesion to be positive for CK7, TTF-1, and surfactant proteins A and B which supports these cells to be type 2 pneumocytes (all controls are appropriate). Based on the immunohistochemical stains and routine H&E slides, the case was signed out as a sclerosing pneumocytoma
Image 1. Gross presentation of the well-defined, round sclerosing pneumocytoma.
Discussion
Sclerosing pneumocytoma (SP) is a rare, benign pulmonary
tumor that was first described in 1956 as a vascular tumor, but has since been
found to be of primitive respiratory epithelium origin. In the past, SP has
also been referred to as sclerosing hemangioma, pneumocytoma, and papillary
pneumocytoma, but the 2015 World Health Organization classification of lung
tumors states that the agreed upon term for this tumor should be a sclerosing
pneumocytoma. SP is commonly seen in middle aged adults, with a female to male
ratio of 5:1. There is no racial bias. Patients are usually asymptomatic, with
the tumor incidentally found on screening chest radiographs. If the patient was
to present with any symptoms, they would usually include a cough, hemoptysis
and chest pain. Radiographically, SP appears as a solitary, well-defined,
homogenous nodule along the periphery of the lung.
Grossly, most SPs appear as a solitary, firm, well-circumscribed,
yellow-tan mass generally arising along the periphery of the lung. The majority
of these tumors appear within the lung parenchyma, but there have been cases
reported of endobronchial and pleural based SP tumors. Multifocal unilateral
tumors and bilateral tumors are uncommon.
Histologically, SP consists of two epithelial cell types:
surface cells and round cells. Surface cells are cuboidal, resembling type II
pneumocytes, with finely stippled nuclear chromatin, indistinct nuclei,
occasional nuclear grooves, and inclusions. The stromal round cells will have bland
oval nuclei with coarse chromatin and eosinophilic cytoplasm (Figure 2). Both
the surface cells and round cells will have a low mitotic rate, but can have
moderate to marked nuclear atypia. Ciliated bronchial epithelium is often
identified in the tumor. There are four architectural patterns identified
within SP: papillary, sclerotic, solid and hemorrhagic, with over 90% of SPs
displaying three of the patterns, and all of the tumors containing at least two
of the patterns.
Papillary pattern: Complex papillae composed of surface cells covering a stroma of round cells
Sclerotic pattern: Papillae containing hyalinized collagen, either in solid areas or along the periphery of hemorrhagic areas (Figure 3)
Solid pattern: Sheets of round cells bordered by surface cells
Hemorrhagic pattern: Large blood filled spaces
Image 2. Photomicrograph demonstrating the cuboidal surface cells and round stromal cells.Image 3. Photomicrograph of the papillary and sclerotic architectural patterns.
Immunohistochemical stains can be helpful in the diagnosis of
SP, with both the surface cells and round cells exhibiting expression of
thyroid transcription factor 1 (TTF-1) and epithelial membrane antigen (EMA). It
should be noted that TTF-1 is also used for the diagnosis of pulmonary
adenocarcinoma, increasing the risk of misdiagnosing SP. The surface cells will
also express both pancytokeratin (AE1/AE3) and Napsin A, with the round cells
being negative for AE1/AE3, but having a variable expression of cytokeratin 7
and the low molecular weight cytokeratin (CAM 5.2). Molecular pathology has demonstrated
a frequent loss of heterozygosity at 5q, 10q and 9p, and an allelic loses at
p16 in the surface and rounds cells. Although the immunohistochemical stains
and molecular pathology results can be very helpful, diagnosis of a SP is still
largely based on routine H&E slides showing the two epithelial cell types
and four architectural patterns.
Electron microscopy will show abundant lamellar bodies
similar to those in type II pneumocytes in the surface cells. Round cells will
lack the lamellar bodies and instead will contain variably-sized electron-dense
bodies that have been thought to represent the different stages of lamellar
body maturation.
The differential diagnosis for SP includes a variety of
benign and malignant neoplasms, which can be difficult to distinguish on
cytology, small biopsies and intraoperative consultations. The cytologic
features include moderate to high cellularity with a bloody background and
foamy macrophages, occasional nuclear pleomorphism in the round cells, absent
mitotic figures, and occasional necrosis with cholesterol clefts and
calcifications. In the case of small biopsies, making a diagnosis of SP can be
difficult if the papillary pattern is highly prevalent without one of the other
three patterns present. With intraoperative consultations, the frozen section
artifact can make it difficult to appreciate the two epithelial cell types or
the four architectural patterns. The gross examination, as well as the
radiographic findings of a well-circumscribed tumor can help point the
Pathologist to favoring a benign neoplasm over a malignant one. The benign
neoplasms that should be considered in the differential diagnosis include:
Clear cell tumor, which will have clear cells
with scant stroma, thin-walled vessels and a strong expression of HMB-45
Pulmonary hamartoma, which will have a
combination of cartilage, myxoid stroma, adipose tissue and trapped respiratory
epithelium
Hemangiomas, which are rare in the lung, and will
lack epithelial cells and contain either a cavernous or capillary morphology
The malignant neoplasms that should be considered in the
differential diagnosis include:
Bronchioalveolar carcinoma, which can have a
papillary pattern, but will not contain the two epithelial cell types and
combination of the four architectural patterns
Metastatic papillary thyroid carcinoma, which is
distinguished from SP by the presence of the characteristic Orphan Annie nuclei
Metastatic renal cell carcinoma, which will
contain nuclear atypia and striking vascularity
Carcinoid, which will contain organoid and
ribbon-like growth patterns
Currently, with the benign nature of SP, surgical excision is
the preferred treatment choice to cure the patient. There have been cases
reported of lymph node metastasis and recurrence, but neither of these appear
to effect the prognosis. This just helps to highlight the need for a
multidisciplinary approach to this benign tumor.
References
Hisson E, Rao R. Pneumocytoma (sclerosing
hemangioma), a Potential Pitfall. Diagn
Cytopathol. 2017;45(8):744-749
Keylock JB, Galvin JR, Franks TJ. Sclerosing
Hemangioma of the Lung. Arch Pathol Lab
Med. 2009;133(5):820-825.
Travis WD, Brambilla E, Nicholson AG, et al. The
2015 World Health Organization Classification of Lung Tumors: Impact of
Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J Thorac Oncol. 2015;10(9):1243-1260.
-Cory Nash is a board certified Pathologists’ Assistant,
specializing in surgical and gross pathology. He currently works as a
Pathologists’ Assistant at the University of Chicago Medical Center. His
job involves the macroscopic examination, dissection and tissue
submission of surgical specimens, ranging from biopsies to multi-organ
resections. Cory has a special interest in head and neck pathology, as
well as bone and soft tissue pathology. Cory can be followed on twitter
at @iplaywithorgans.
A 58 year old female with no significant past medical history presented her primary care physician with chief complaint of abdominal pain. She reported continued vague abdominal symptoms for the past two months, with intermittent diarrhea and increased flatulence. No recent travel history or significant exposures were identified. An ultrasound of the right upper quadrant was unremarkable and no gallstones were present. The patient was scheduled for a screening colonoscopy. A stool specimen was submitted to the microbiology laboratory for stool culture and ova & parasite exam.
Laboratory
Identification
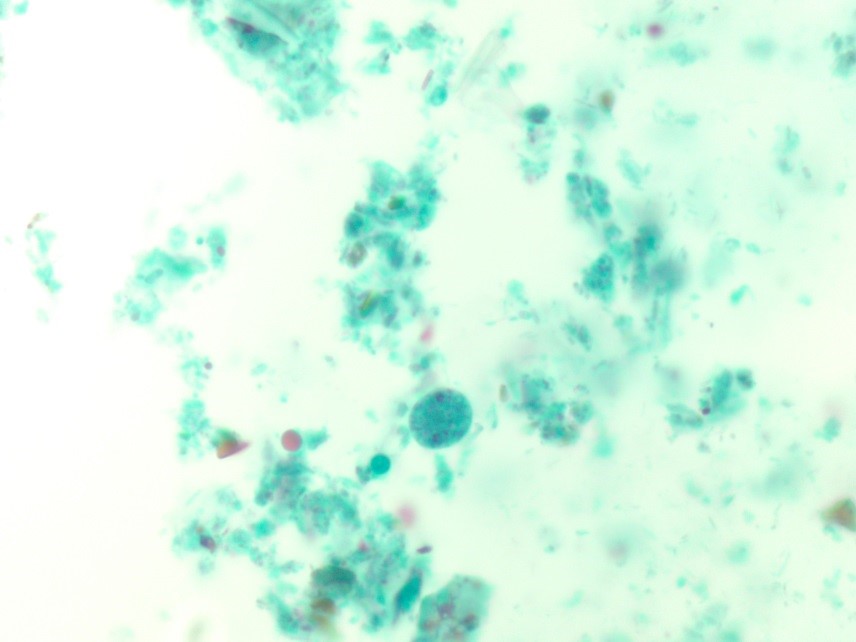
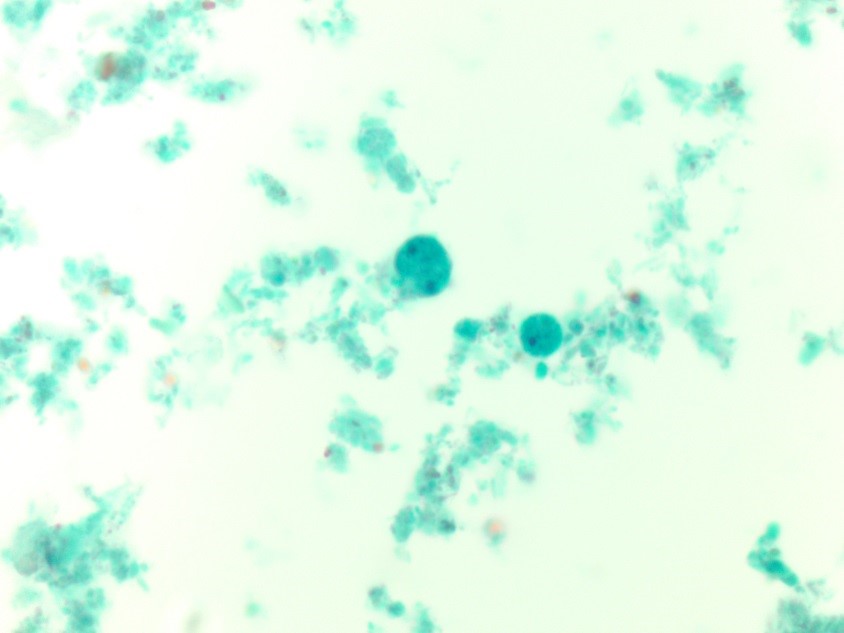
Image 1. Trichrome stained fecal smear illustrating a binucleated trophozoite with fragmented karyosomal material from a stool ova & parasite exam. Image 2. Additional trichrome fecal smear image highlighting both uninucleate and binucleate trophozoites that range in size from 5 to 15 um.
The findings from the ova and parasite
exam were consistent with Dientamoeba
fragilis, an intestinal flagellate. The stool culture was negative for Salmonella, Shigella, and Escherichia coli 0157:H7.
Stool enzyme immunoassays were negative for Campylobacter
spp.and Shiga toxin 1 and 2.
Discussion
Dientamoeba
fragilis is an intestinal flagellate
with worldwide distribution and causes asymptomatic and symptomatic infections,
predominantly in small children. Symptoms of infection may include intermittent
diarrhea, abdominal pain, anorexia, weight loss, and flatulence. While the pathogenesis is not completely
understood, transmission is thought to occur via the fecal oral route and it is
hypothesized that the trophozoites are transmitted via the eggs of nematodes, Enterobiusvermicularis and Ascaris
lumbricoides, due to a higher incidence of co-infections between these
organisms than expected.
In the laboratory, the diagnosis of D. fragilis is made by ova and parasite
exam. The trophozoite resembles amebae and is typically 9-12 µm. Most
trophozoites are binucleate with finely granular cytoplasm and the within the nuclei
there are 4-8 fragments of karyosomal granules (Figure 1). Due to the fact that
30-40% of D. fragilis trophozoites
are uninucleate (Figure 2) and they lack external flagella, they must be
differentiated from Endolimax nana and
Entamoeba hartmanni, which are both
non-pathogenic amebae. Historically, no cyst phase was known for D. fragilis; however, recent studies have
identified precyst forms or putative cysts. Permanently trichrome stained
slides are essential to diagnosing D.
fragilis infection, as the organism is hard to detect in concentrated
smears.
Since our patient was symptomatic, she was treated with iodoquinol, the drug of choice for D. fragilis infections. Her symptoms resolved and colonoscopy did not reveal additional pathology.
-Debbie Walley, MD, is a 4th year Anatomic and Clinical Pathology chief resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the
University of Mississippi Medical Center in Jackson, MS. She is
certified by the American Board of Pathology in Anatomic and Clinical
Pathology as well as Medical Microbiology. She is the Director of
Clinical Pathology as well as the Microbiology and Serology
Laboratories. Her interests include infectious disease histology,
process and quality improvement, and resident education.
Last month, it was as fun to write about hematology peripheral
smear differentials as it was to address the importance of
interdisciplinary collaboration. I found myself in a unique position both as a
medical student as well as a former medical laboratory scientist in what was a
great clinical training rotation in hematology/oncology. Now, with just one
rotation left until the end of my medical school journey, I want to take you on
a look back at some of the very first posts I made here on Lablogatory and
update you on the intersectional, collaborative topic that I shared with you
almost two years ago: Zika!
Image 1. ASCP’s official professional society partner, The Pathologist. I’ve been getting them in my mailbox since the official partnership was announced. It’s an excellent platform for laboratory professionals across scopes to discuss relevant topics in pathology. I was particularly excited to see Zika make an appearance last month! (Source: The Pathologist [online] https://thepathologist.com/diagnostics/our-powers-combined)
In a recent digital article on ASCP’s partner, The
Pathologist, author and staff editor Michael Schubert wrote about the
connectivity between public health, epidemiologic research, laboratory
medicine, and clinical patient outcomes. He examined the effectiveness and
accuracy of Zika testing availability in commercially available assays and
spoke with a leading virologist in the field from Berlin. You may recall one of
those “ancient” posts I made about Zika, where I was part of a research team
that used the same methodology! Combined immunoglobulin-specific assays,
arbovirus detection in the heat of a public health epidemic’s epicenter, and
lab medicine that complimented my concurrent immunology class in med
school—what more could you ask for?
And, since the last tagged Lablogatory Zika update I can see
was
by Dr. Sarah Riley in February of 2017, here’s my update! Dr. Riley’s post
was a fantastic summary of the Zika epidemic, its troublesome diagnostic
assessments, and the recommendations and plans of organizations like the World
Health Organization (WHO). She was, and still is, right—the “struggle is still
real’ when it comes to Zika testing. Curious about what it was like during the
2016 epidemic? Who was doing testing, what kind of testing, and what was the
lab data climate? Well…it feels like it’s time for a…
*** FLASHBACK ***
An Arbovirus Abroad
Hey! My inaugural
post! It was fun to go back and see the data from the work then (Spoilers:
epidemiologic updates are on your horizon). We were just getting started to
take an assessment of the situation and address it as a public health concern.
My then Caribbean location was a great place to study Zika trends coming from
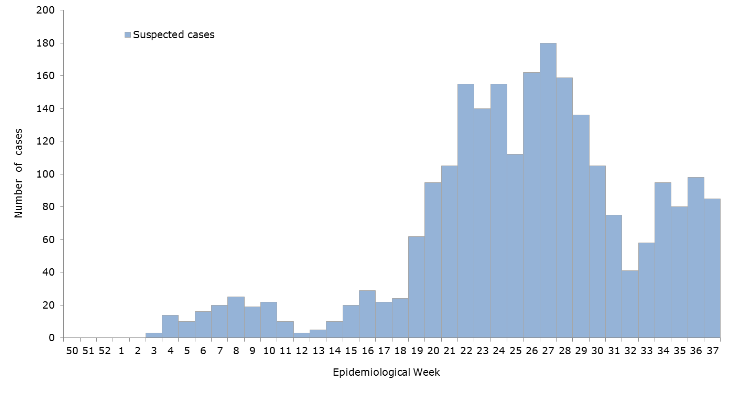
Brazil, Puerto Rico, and Florida. As a snapshot, at that time (Dec 2016) there
were a purported almost 2,000 cases, however less than a fifth of those cases
were serologically confirmed by lab testing. Before the recommendations to move
toward RT-PCR, most labs in the region were requesting commercially available
screening tests for IgG/IgM assays.
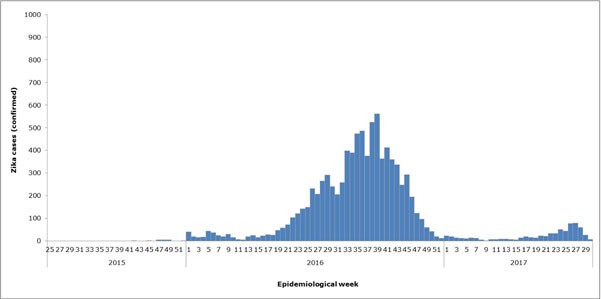
Image 2a. These were the (then) suspected Zika viral infection cases per epidemiological week, Pan-American Health Organization (PAHO) and World Health Organization (WHO) 2016. My wife and I are included in these statistics—that mosquito virus rash is awful!Image 2b. Remember that spoiler I promised above? Well here’s the updated WHO epidemiologic data for confirmed Zika cases in the region we worked in. Seems like the mosquitoes…buzzed off. (Source: WHO)
Healthy Me
How do you reach people when you’ve got compelling public health
lab data that translates to possible prevention of infection and spread of
disease? Easy: go
to where the people are and engage them when and where they’re comfortable.
One of the overarching themes in public health is mitigating barriers to change
by way of utilizing social humility. This a certainly a type of
interdisciplinary collaboration because if we’re the experts on IgM and IgG
trends in testing confirmations, the public are the experts in social
determinants of health within their communities.
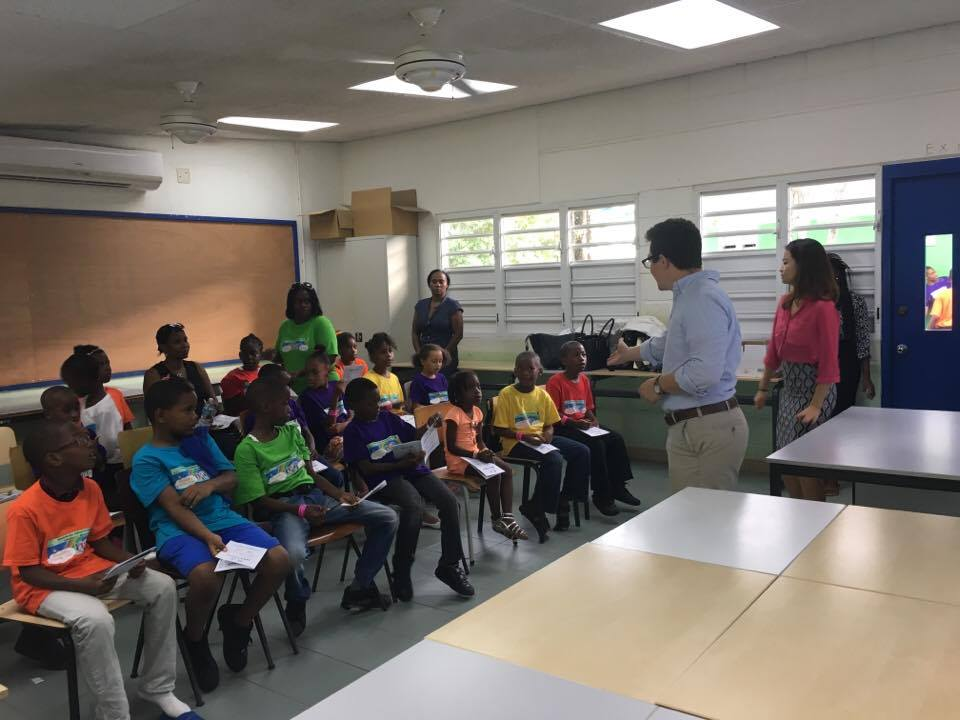
Image 3. Want to make sure a message gets home to every family? Bug their kids about Zika bugs in fun, educational ways. That’s me delivering one of my “Healthy Me” presentations to children, October 2016.
Laboratory Data and Global Health Security
As my team and I were busy preparing SOPs, conducting a new
project aimed at improving local health literacy and source reduction, securing
IRB approval, and collecting data about the residents of Sint Maarten to
correlate with local Health Ministry projections, one of the officials—who now
serves as a regional director for PAHO—took our work to the Global
Health Security Agenda Summit. Talk about motivation! In and out of the
lab, I worked with teams who were getting some fantastic work done on the
ground with respect to mosquito-borne virus research.
Image 4. IgM and IgG seroprevalence of Zika virus (along with other Arboviruses i.e. West Nile, Chikungunya, Dengue, and Yellow Fever etc.) within the community around my medical school. We used commercially available IgG and IgM assays from Germany with great success. Internal controls and known cases were fantastic ways to include internal validation.
IRBs and Public Heath Pathology
For those of us who work in laboratory medicine, it’s easy
to talk about the best way to test, detect, and treat an epidemiologic
threat—it’s even exciting when it’s a current threat. But to really be
successful, you’ve got to collaborate with those outside of the lab, and often
this means thinking “outside the box.” Public
health is different from lab medicine in that while lab-work is based
around results, testing, and organized data-driven decisions, success in public
health is highly determined by community buy-in in the form of partnerships!
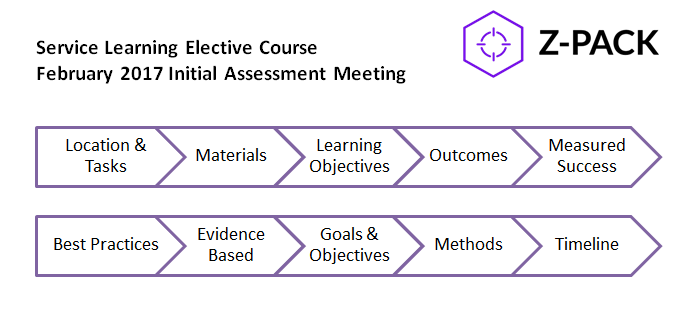
Figure 1. There’s a method to the community “buy-in” concept. With a foundation in evidence-based practices, any project aimed at improving public health outcomes must include some critical components like clear objectives, attainable goals, sustainability, and effective (and constant) re-evaluation.
*** FLASH …
FORWARD? ***
So, after my time in Sint Maarten, I came to New York City
to rotate through my clinical clerkships. And, if you’ve seen some more recent
post-Zika posts on this website, you know they’ve been going great! Within a
few months of being here, my wife brought back some swag from a training
session she attended. (Side note: she’s a graduate-level nurse, working in the
public health non-profit sector with vulnerable populations in the inner
city—she’s too busy to blog.) After months of both of us working and learning
about Zika and public health initiatives in the Caribbean, we were greeted by
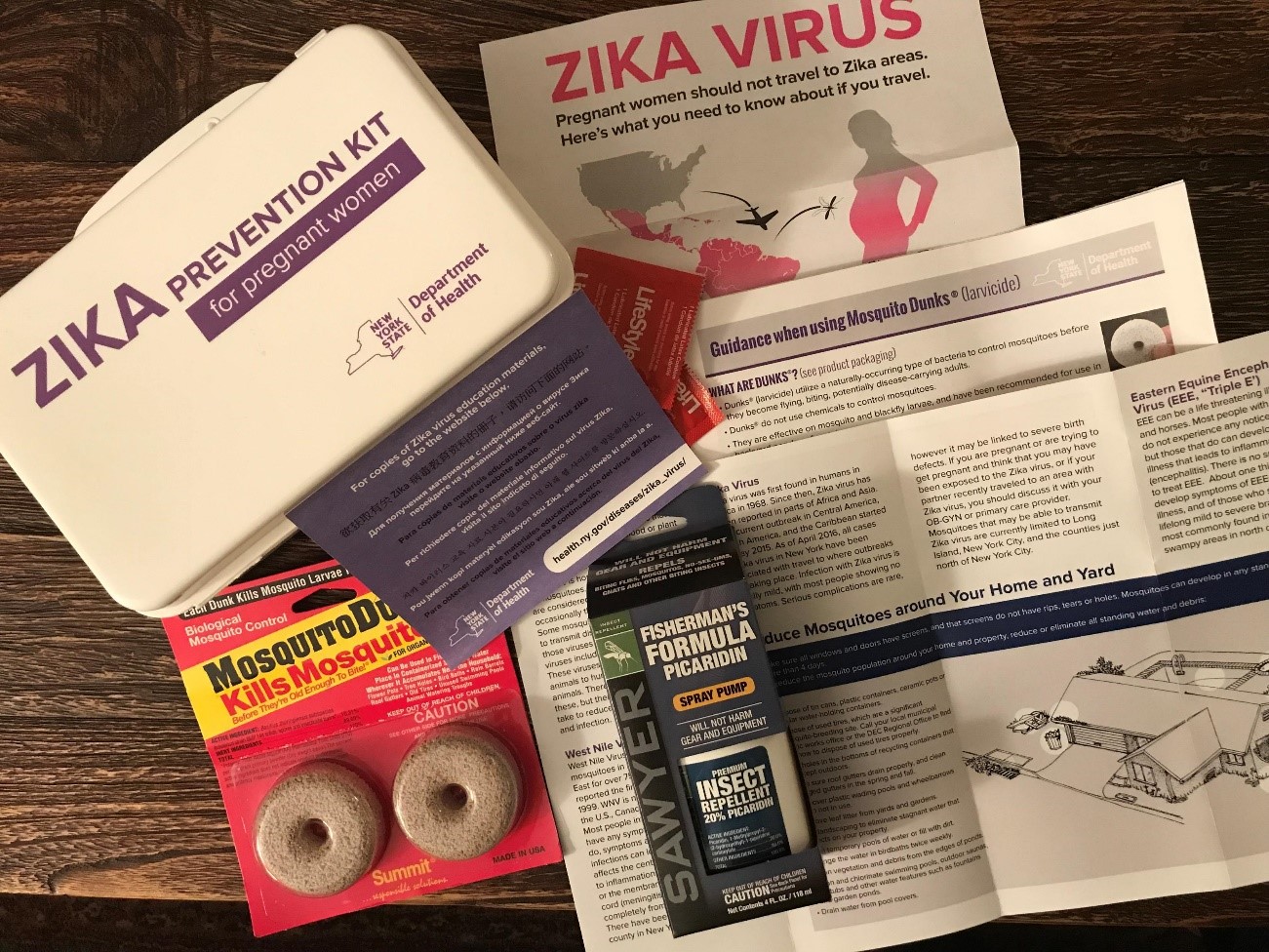
this fantastic toolkit from the New York State Department of Public Health!
Image 5. Empowering a large number of patients with highly variable demographics is challenging. The NYS DOH distributed “Prevention Kits” for Zika Virus which included: Zika Virus educational materials in 8 languages, pamphlets on reducing mosquito activity, travel related information for pregnant women, 2 larvicide pellets with instructions for using larvicide, picaridin insect repellent, and condoms.Image 6. That’s us! My wife Kathryn and I presenting on the importance of Disaster Planning and Implementation of Preparedness Programs at the 2019 Caribbean Conference of Disaster Medicine. Disasters are bad on their own, but think about what happens months after flooding, hurricanes, or destruction—transmittable diseases. And that includes standing-water-borne mosquito viruses!
The take home message: collaboration is key, both inside and
out of the lab. Schubert’s piece in The Pathologist created a fantastic
dialogue in addressing the clinical needs for interdisciplinary collaboration.
The best testing means finding out exactly where the needs are and using
data-driven decisions to implement change or action. In the lab, that means
constantly working for higher quality and better patient outcomes in every
test, result, report, and (mosquito) byte of data. In the field, it means the
same thing, but instead of metrics like sensitivity, specificity, and TAT it’s
about cultural humility, attainable goals, and dynamic timing.
Thanks for reading! Hope most of our national heat wave spared you, but if it didn’t remember: don’t keep standing water around, wear light loose clothing, and use appropriate insect repellent!
See you next time!
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola
University Chicago with a BS in Molecular Biology and Bioethics and then
Rush University with an MS in Medical Laboratory Science. He is
currently a medical student actively involved in public health and
laboratory medicine, conducting clinicals at Bronx-Care Hospital Center
in New York City.
Everyone
who works in a laboratory knows that there are certain rules and regulations to
be followed to ensure accuracy in testing, and the safety of both the patient
and testing personnel. With all the acronyms floating around (CLIA, FDA, CAP,
CMS, TJC) it can get confusing to keep track of who controls what, and which
rules apply to your specific lab. In the first installment of this 3-part
series on regulations, we’ll review the different federal agencies responsible
for oversight and moderation of the laboratory. In part 2 we’ll go further
in-depth to demystify testing complexity (waived, non-waived, PPM) and why it’s
important to know the correct classification for the tests you perform. Lastly,
we’ll review the optional accreditations available to labs, and how
accreditation differs from certification.
CLIA
CLIA
refers to the Clinical Laboratory Improvement Amendments of 1988. These
amendments were drafted to the Public Health Services Act, in which the federal
program was revised to include certification and oversight of clinical
laboratory testing. Although there have been two additional amendments made
after 1988 (1997, 2012), the law still continues to be cited as CLIA ’88 as it
is named within legislation.
These
CLIA regulations helped to establish quality standards for all U.S. laboratory
testing performed on human specimens (except for research) for the purpose of
assessment of health, or the diagnosis, prevention, or treatment of disease.
The regulations cover all aspects of testing including general laboratory
requirements, quality monitors, pre-analytics, analytic performance,
post-analytics, and personnel requirements.
In
addition to setting the basic ground rules for performing quality laboratory
testing, the CLIA regulations also require clinical laboratories to be
certified by their state as well as the Center for Medicare & Medicaid
Services (CMS) before accepting human samples for diagnostic testing.
Laboratories can obtain multiple types of CLIA certificates, based on the kinds
of diagnostic tests they perform. In order for laboratories to receive payments
from Medicare or Medicaid, laboratories must be properly certified for the
testing they are performing and billing for.
There are
3 federal agencies responsible for enforcing the CLIA regulations: The Food
& Drug Administration (FDA), Center for Medicaid Services (CMS) and the
Center for Disease Control and Prevention (CDC). Each agency has a unique role
in assuring quality laboratory testing.
CMS
The
Centers for Medicare & Medicaid Services (CMS) is the federal agency
responsible for ensuring that the CLIA standards are upheld and enforced. Their
responsibilities include the following:
Issuing
laboratory certificates
Collecting
user fees
Conducting
inspections and enforcing regulatory compliance
Approving
private accreditation organizations (such as CAP) for performing inspections,
and approves state exemptions
Monitoring
laboratory performance on Proficiency Testing (PT) and approving PT programs
Publishing
CLIA rules and regulations
FDA
The Food
& Drug Administration (FDA) is primarily responsible for reviewing and
approving new tests, instruments, and equipment used in diagnostic laboratories.
They also perform the following tasks:
Categorize
tests based on complexity
Review
requests for Waiver by Application from manufacturers
Develop
rules/guidance for CLIA complexity categorization
CDC
The Center
for Disease Control and Prevention (CDC) responsibilities include the following
tasks:
Provide
analysis, research, and technical assistance
Develop
technical standards and laboratory practice guidelines, including standards and
guidelines for cytology
Conduct
laboratory quality improvement studies
Monitor
proficiency testing practices
Develop
and distribute professional information and educational resources
Manage
the Clinical Laboratory Improvement Advisory Committee (CLIAC)
To
summarize, CLIA establishes the rules and guidelines that laboratories must
follow to ensure they are providing accurate laboratory results. Federal
agencies then work together to support the CLIA amendments and enforce
compliance. All certified laboratories will be subject to inspection by
regulatory agencies to ensure compliance with the rules. In some cases, your
local state Department of Health (DOH) or accrediting agency may be more
stringent or have additional requirements to be followed – always go with the
stricter requirement to ensure compliance with all agencies.
Coming
up next we’ll review how the FDA decides the complexity of each test, and how
this designation will affect the CLIA rules to be followed.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s
2018 Top 5 in the 40 Under Forty recognition program. She has worked in
the medical laboratory profession for over 18 years. In her current
position, she transitions between performing laboratory audits across
the entire Northwell Health System on Long Island, NY, consulting for
at-risk laboratories outside of Northwell Health, bringing laboratories
up to regulatory standards, and acting as supervisor and mentor in labs
with management gaps.
The general public doesn’t always know a lot about laboratory
testing in general, but most people know a little about blood types, even if
it’s what they have learned from TV! Blood types do seem to come up in casual
conversation. We might hear a conversation about blood type after someone has
donated blood, or between family members comparing notes, who ask “What’s your
type?” Yet, even with medical technologists, there can still be some confusion
about blood types and blood typing, particularly if one has not worked in Blood
Bank in many years. I recently received an email from a colleague who had a few
questions about blood types, as she has not worked in Blood Bank for over 40
years. I always tell my students that no question is a bad question, and indeed,
she asked some very good questions, which I will address with this case study.
What blood type is listed on a patient’s chart if they type “O
Du”?
What blood type is recorded on a donated unit of blood typed “O
Du”?
What type of blood does an “O Du” patient receive?
Can an “O Du” patient have a transfusion reaction if they are
transfused with O positive blood? Would she need to receive O negative blood in
a transfusion?
Does an “O Du” patient need to receive RhoGAM if she pregnant and
her husband is Rh positive?
If you have ever wondered or can’t remember details about any of
these questions, you’re in the right place. So, what’s new, if anything, with
blood types?
Landsteiner discovered the ABO blood group system in 1901, and
identified A, B and O blood types, using experiments performed on blood from
coworkers in his laboratory. The discovery of the codominant AB blood type soon
followed, but it was not until around 1940 that the Rh blood group was first described.
In 1946, Coombs and coworkers described the use of the antihuman globulin (AHG)
to identify weak forms of Rh antibodies in serum. For us old blood bankers, the
original name for this test was the Coombs’ test. (You will still find
physicians ordering a Coombs’ test!) The current and proper name for this is
the direct antibody test (DAT), which is used to detect in vivo sensitization
of RBCs. AHG can also be used to detect in- vitro sensitization of RBCs using
the 2 stage indirect antibody test (IAT).
Since Landsteiner’s work, we have not discovered any new blood groups
that are part of the routine blood type. The ABO and Rh blood groups are still
the most significant in transfusion medicine, and are the only groups consistently
reported. However, we currently recognize 346 RBC antigens in 36 systems.1 Serological tests determine RBC
phenotypes. Yet, today we can also determine genotype with family studies or
molecular testing. This case study and 2 part blog reviews some terminology in
phenotyping, some difficulties and differences encountered, and explores the
possibility of RHD genotyping to assess a patient’s true D status.
Our case study involves a 31 year old woman who is newly married.
She is not currently pregnant, has never been pregnant, is not scheduled for
surgery but has had a prior surgery 15 years ago, and has never received any
blood products. She and her husband recently donated blood and, as first time
blood donors, just got their American Red Cross (ARC) blood donor cards in the
mail. The husband noted that his card says that he is type O pos. The woman
opens her card, and, with a puzzled look on her face, says “My card says I’m an
O Pos, too. There must be a mistake.” She knows she has been typed before and
checks her MyChart online. Sure enough, her blood type performed at a local
hospital is listed in her online MyChart as O negative. She further checks
older printed records and discovers that 15 years ago, before surgery, she was
typed at a different hospital as “O Du”. She is very upset, wondering how she
can have 3 different blood types. She is additionally concerned because they
are planning to have children and recalls being told that because she is Rh
negative, that she would need Rhogam. Is she Rh negative or positive, and what
does Du mean? Will she need Rhogam when pregnant? She has many questions and calls
the ARC donor center for an explanation.
What blood type is listed on a patient’s chart
if they type “O Du”?
What is happening here, what is this woman’s actual blood type, and what testing can be done to ensure accuracy in Rh typing? From the patient reports, it appears that this woman has what today we call a “weak D.” Du is an older terminology that should no longer be used, and that has been replaced by the term “weak D.” But, why does she have records that show her to be an O neg, a type O, Du (today, this would be written O weak D), and now, a card from ARC stating she is O pos?
RhD negative phenotypes are ones that
lack detectable D antigen. The most common Rh negative phenotype results from
the complete deletion of the RHD gene. Serologic testing with anti-D is usually
expected to produce a strong 3+ to 4+ reaction. A patient with a negative
anti-D at IS and at IAT would be Rh negative. If the patient has less than 2+ strong
reaction at immediate spin (IS), but reacts at IAT, they would be said to have
a serologically weak D.1 Historically, weak D red blood cells (RBCs)
are defined as having decreased D antigen levels which require the IAT for
detection. Today’s reagents can detect many weak D
types that may have been missed in the past, without the need for IAT. However,
sometimes IAT is still necessary to detect a weak D. When this is necessary is
dependent on lab SOPs and whether this is donor testing or patient testing. The
reported blood type of this patient also depends on the SOPs of the laboratory
that does the testing. And, the terminology used for reporting is also lab
dependent. It is not required by AABB to test patient samples for weak D
(except for babies of a mother who is D negative). There is also no general
consensus as to the terminology to be used in reporting a weak D. Some labs would
result this patient as O negative, weak D pos. Some labs may result O pos, weak
D pos. Others may show the individual reactions but the resulted type would be
O pos. Labs who do not perform weak D testing would report this patient as O, Rh
negative. The following chart explains why this patient appears to have 3 types
on record.
Figure 1. Tube typing results of same patient from different labs with different SOPs.
What blood type is recorded on a donated unit
of blood typed “O Du?”
AABB Standards for Blood Banks and
Transfusion Services requires all donor blood to be tested using a method that
is designed to detect weak D. This can be met through IAT testing or another
method that detects weak D. If the test is positive, the unit must be labeled
Rh positive. This is an important step to prevent alloimmunization in a
recipient because weak D RBCs can cause the production of anti-D in the
recipient. This also explains why the ARC donor card this patient received
lists her type as O pos.
What type
of blood does an “O Du” patient receive?
Historically, weak D red blood cells
(RBCs) were defined as having decreased D antigen levels which require the IAT
for detection. A patient who is serologic weak D has the D antigen, just in
fewer numbers. This type of weak D expression primarily results from
single-point mutation in the RHD gene that encodes for a single amino acid
change. The amino acid change causes a reduced number of D antigen sites on the
RBCs. Today we know more about D antigen expression because we have the
availability to genotype these weak D RBCs. More than 84 weak D types have been
identified, but types 1, 2, and 3 represent more than 90% of all weak D types
in people of European ethnicity.2 An Rh negative patient has no D
antigen and should, under normal circumstances, only receive Rh negative blood.
Yet, there has been a long history of transfusing weak D patients with Rh
positive RBCs. 90% of weak D patients genotype as Type 1, 2 or 3 and may
receive Rh positive transfusions because they rarely make anti-D. 2
It is now known that weak D can actually
arise from several mechanisms including quantitative, as described above, position
effect, and partial D antigen. Molecular testing would be needed to
differentiate the types, but, with the position effect, the D antigen is
complete and therefore the patient may receive Rh positive blood with no
adverse effects. On the other hand, a partial D patient may type serologically
as Rh negative or Rh positive and can be classified with molecular testing. It
is important to note that these partial D patients are usually only discovered
because they are producing anti-D. If anti-D is found, the patient should
receive Rh negative blood for any future transfusions.
Thus, 3 scenarios can come from typing
the same patient. With a negative antibody screen, and because 90% of weak D
patients have been found to be Type 1, 2 or 3 when genotyped, many labs do not routinely
genotype patients and will report the blood type as Rh pos and transfuse Rh pos
products. However, depending on the lab medical director and the lab’s SOPs,
these same patients may be labeled Rh neg, weak D and receive Rh negative
products. There is no general consensus on the handling and testing of weak D
samples. The 3rd scenario is that many labs do not test for weak D
in patients at all, and a negative D typing at IS would result in reporting the
patient as Rh neg, with no further testing. In this case, the patient would be
transfused with Rh negative products.
Can an “O
Du” patient have a transfusion reaction if they are transfused with O positive
blood? Would she need to receive O negative blood in a transfusion?
This question was covered
somewhat in the above discussion. Policies regarding the selection of blood for
transfusion are lab dependent, dictated by the lab medical director, and are
based on the patient population, risk of developing anti-D, and the
availability or lack of availability of Rh negative blood products. Anti-D is
very immunogenic. Less than 1 ml of Rh pos blood transfused to an Rh negative
person can stimulate the production of anti-D. However, not all patients
transfused with Rh positive blood will make and anti-D. As discussed above, 90%
of weak D patients are types 1, 2 or 3, would be unlikely to become
alloimmunized to anti-D. If a weak D patient with a negative antibody screen
receives a unit of D pos RBCs, there is a very small possibility that they are
a genotype who could become alloimmunized to the D antigen and produce anti-D. However,
as stated above, the majority of weak D patients can be
transfused with D positive RBCs. Thus, with few exceptions, from a historical
perspective, one can safely classify the weak D as D positive.
This question gets a little trickier
when dealing with females of childbearing age. We particularly want to avoid
giving Rh positive blood to females to avoid anti-D and the complications of
Hemolytic Disease of the Fetus and Newborn. Therefore, when dealing with these
patients, lab policies and physicians tend to be more conservative in their
approach to transfusion. The consequences, however, in males and older females
are less serious and these patients could be given Rh positive blood if there
exists a shortage of Rh negative units. Any patient who becomes alloimmunized
to the D antigen, would thereafter be transfused with Rh negative products.
Does an “O
Du” patient need to receive RhoGAM if she pregnant and her husband is Rh
positive?
This, again, would be up to the medical
director, the lab’s SOPs or the patient’s physician. Depending on lab practice,
the lab may or may not perform weak D testing. If the lab does not perform weak
D and results this patient as Rh neg, the patient would get Rhogam. If the lab
does do weak D testing and finds a weak D phenotype, the decision whether or
not to give Rhogam would be up to lab practices and the practitioners involved.
The lab’s policy on terminology used in resulting the type may also reflect the
decision whether or not to give Rhogam. This brings up a lot of questions in
the lab because we know that a patient who would not make anti-D would not need
Rhogam. So, what is the best course of action? Read my next blog to learn more
about troubleshooting and resolving D typing discrepancies!
From the discrepancies in reported type in this individual, and putting all the pieces of the puzzle together, we can conclude that this patient is a weak D phenotype. However, the type reported and the terminology used varies from lab to lab. Molecular testing is available, yet most labs are still using serological testing for blood types for both donors and patients. This is based on several factors within the lab setting. Stay tuned for my next Blood Bank blog exploring D typing discrepancies and the financial aspects of performing genotype on pregnant patients to clarify Rh type.
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated
from Merrimack College in N. Andover, Massachusetts with a BS in
Medical Technology and completed her MS in Clinical Laboratory Sciences
at the University of Massachusetts, Lowell. She has worked as a Medical
Technologist for over 30 years. She’s worked in all areas of the
clinical laboratory, but has a special interest in Hematology and Blood
Banking. When she’s not busy being a mad scientist, she can be found
outside riding her bicycle.
A 15 year old male with a past medical history significant
for Tetralogy of Fallot (congenital heart defect), multiple valve replacements,
chronic kidney disease, and prior Bartonella endocarditis. He presented with a
“flu-like” illness including muscle aches, fevers, fatigue, and night sweats. His
symptoms slowly dissipated after about three days. However, he had labs drawn
including multiple blood culture sets which were all positive for growth.
Laboratory Findings
Gram stain showed gram positive bacilli and culture plates grew two morphologies of slow growing gray, granular and opaque colonies.This organism was identified by MALDI-TOF as Corynebacterium pseudodiphtheriticum.
Image 1. Gram stain with gram positive bacilli .Image 2. Culture with small, grayish colonies with granular appearance and opaque centers (growth at day 2).
Discussion
The
genus Corynebacterium comprises a
collection of irregular-formed, rod-shaped or coccoid bacteria that are
non-motile, catalase-positive, and non-spore-forming.
Corynebacterium
pseudodiphtheriticum
(previously designated as Corynebacterium
hofmannii) is a nonlipophilic, nonfermentive, urease- and nitrate-positive Corynebacterium species.1C. pseudodiphtheriticum is part of the
usual oropharyngeal bacterial flora, including the nares and throat. It appears
to play a role in preventing colonization of oropharyngeal epithelia by
pathogenic bacteria.
Most
commonly, C. pseduodiptheriticum is a
pathogen of the respiratory tract with cases of nosocomial and
community-acquired pneumonia, bronchitis, tracheitis, pharyngitis, and
rhinosinusitis. Endocarditis is the second most common infection site, although
very rare. Cases of urinary tract and wound infections have also been reported.
Treatment
is usually with penicillin alone or in combination with aminoglycosides. Antibiotic
susceptibility profiling of C.
pseudodiphtheriticum isolates showed that resistance to oxacillin,
erythromycin, clindamycin, and macrolides are common.1
-Nicole Mendelson, MD
is a 1st year Anatomic and Clinical Pathology resident at the
University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.