Clinical History
A 58 year old female with no significant past medical history presented her primary care physician with chief complaint of abdominal pain. She reported continued vague abdominal symptoms for the past two months, with intermittent diarrhea and increased flatulence. No recent travel history or significant exposures were identified. An ultrasound of the right upper quadrant was unremarkable and no gallstones were present. The patient was scheduled for a screening colonoscopy. A stool specimen was submitted to the microbiology laboratory for stool culture and ova & parasite exam.
Laboratory Identification
The findings from the ova and parasite exam were consistent with Dientamoeba fragilis, an intestinal flagellate. The stool culture was negative for Salmonella, Shigella, and Escherichia coli 0157:H7. Stool enzyme immunoassays were negative for Campylobacter spp.and Shiga toxin 1 and 2.
Discussion
Dientamoeba fragilis is an intestinal flagellate with worldwide distribution and causes asymptomatic and symptomatic infections, predominantly in small children. Symptoms of infection may include intermittent diarrhea, abdominal pain, anorexia, weight loss, and flatulence. While the pathogenesis is not completely understood, transmission is thought to occur via the fecal oral route and it is hypothesized that the trophozoites are transmitted via the eggs of nematodes, Enterobius vermicularis and Ascaris lumbricoides, due to a higher incidence of co-infections between these organisms than expected.
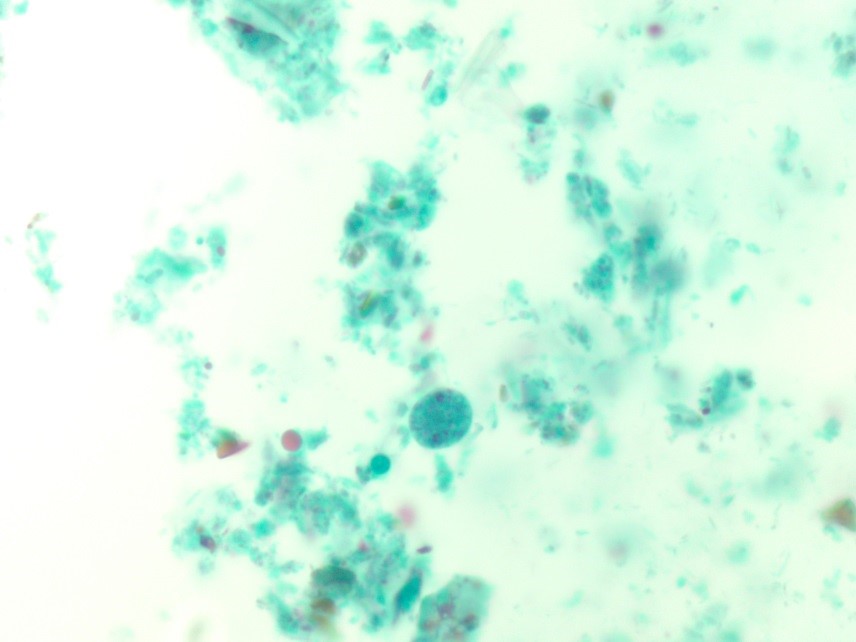
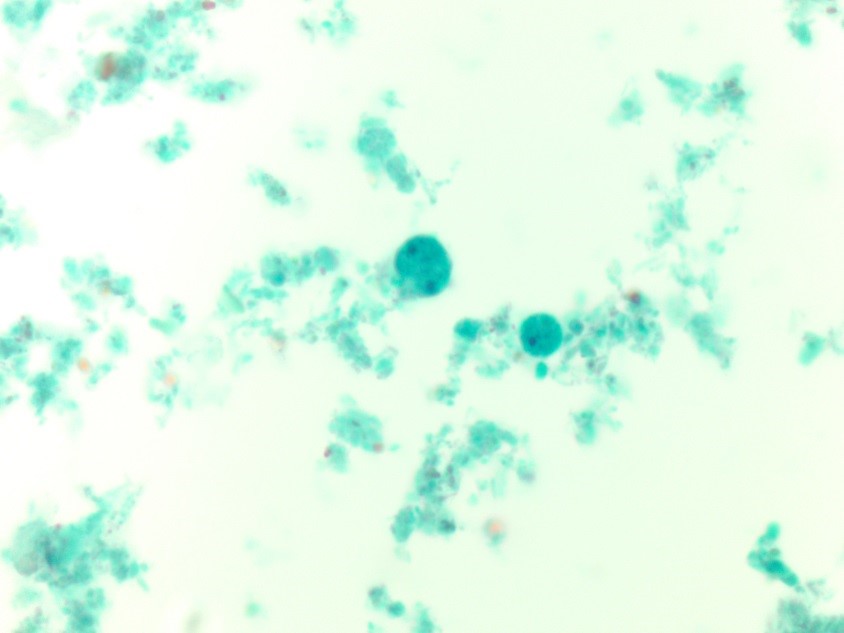
In the laboratory, the diagnosis of D. fragilis is made by ova and parasite exam. The trophozoite resembles amebae and is typically 9-12 µm. Most trophozoites are binucleate with finely granular cytoplasm and the within the nuclei there are 4-8 fragments of karyosomal granules (Figure 1). Due to the fact that 30-40% of D. fragilis trophozoites are uninucleate (Figure 2) and they lack external flagella, they must be differentiated from Endolimax nana and Entamoeba hartmanni, which are both non-pathogenic amebae. Historically, no cyst phase was known for D. fragilis; however, recent studies have identified precyst forms or putative cysts. Permanently trichrome stained slides are essential to diagnosing D. fragilis infection, as the organism is hard to detect in concentrated smears.
Since our patient was symptomatic, she was treated with iodoquinol, the drug of choice for D. fragilis infections. Her symptoms resolved and colonoscopy did not reveal additional pathology.

-Debbie Walley, MD, is a 4th year Anatomic and Clinical Pathology chief resident at the University of Mississippi Medical Center.

-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the Director of Clinical Pathology as well as the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement, and resident education.
