Case History
A 36 year old female underwent thyroidectomy for multinodular goitre that led to the fortuitous discovery of a neck mass. The neck mass specimen submitted comprised two lymph nodes measuring 2.2 cm and 1.3 cm in the greatest dimensions, with a fleshy tan cut surface.
Biopsy Findings
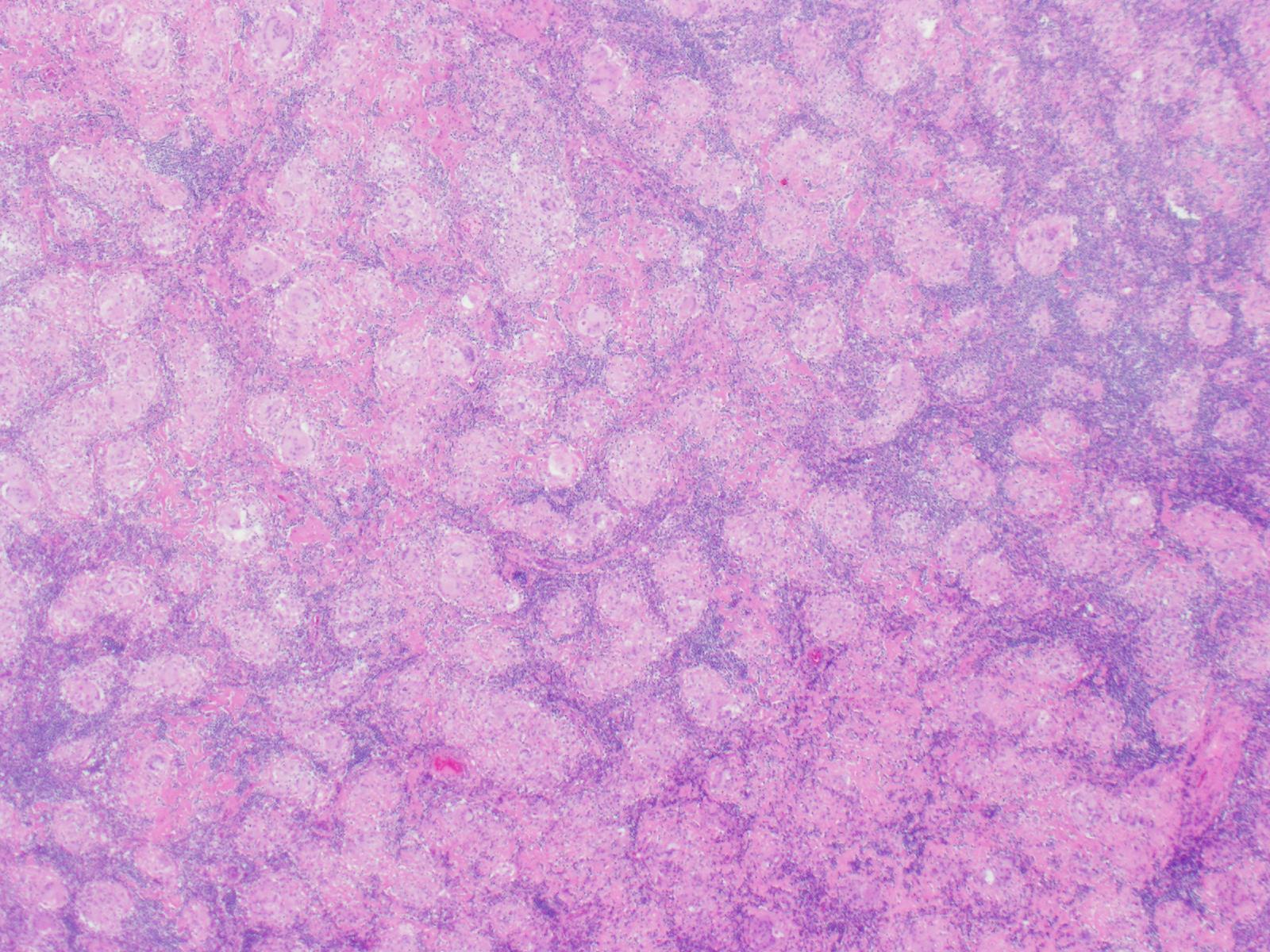

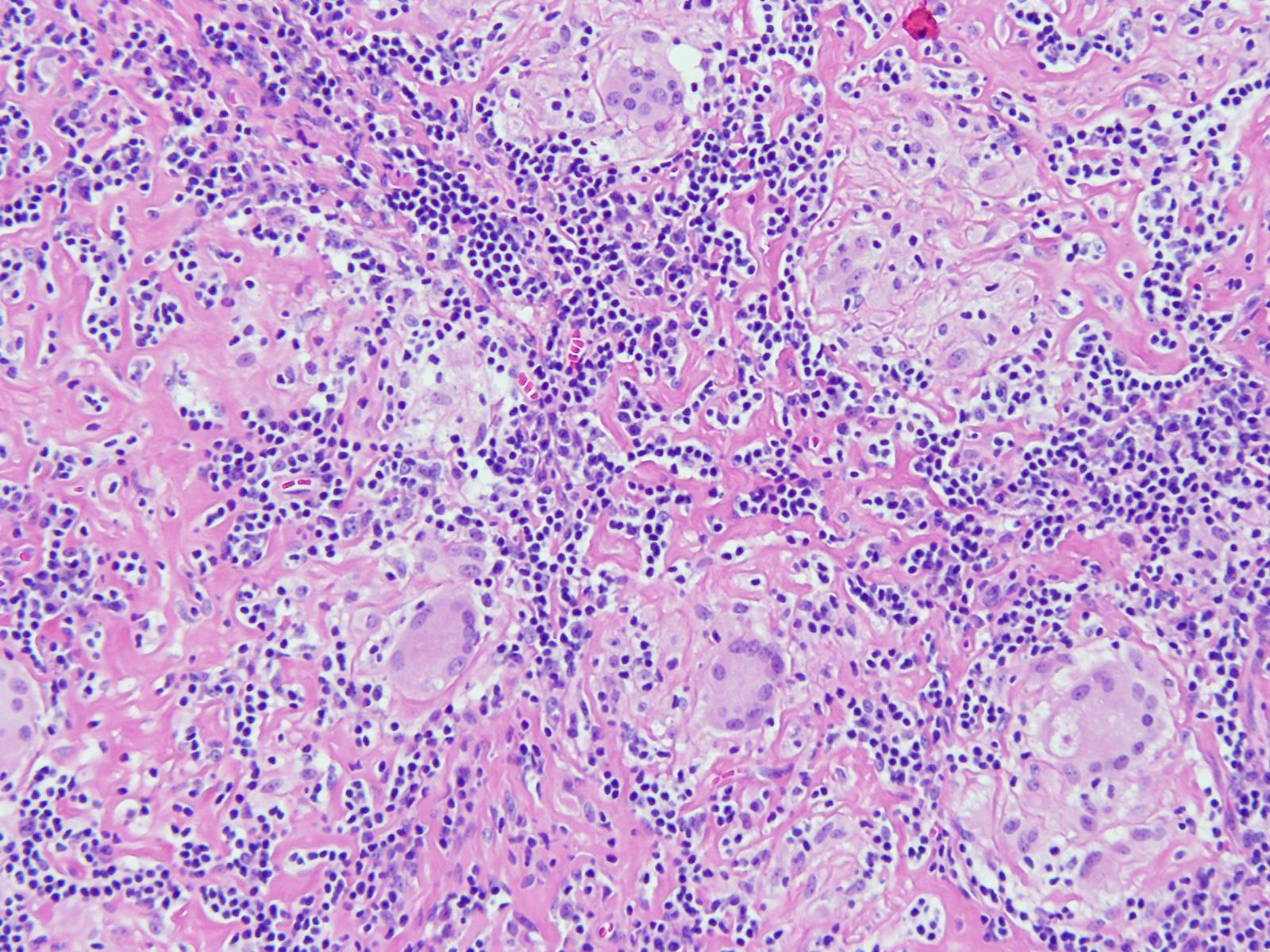
H&E stained sections revealed numerous non-necrotizing granulomas effacing and replacing normal lymph node architecture. These consisted of pale epithelioid histiocytes and Langhans type of giant cells. The granulomas lacked a peripheral rim of lymphocytes. AFB and GMS stains were negative for microorganisms
Diagnosis
A diagnosis of non-necrotizing granulomatous lymphadenitis was rendered noting that in the correct clinical context the findings could represent sarcoidosis.
Discussion
Granulomatous inflammation is a special type of chronic inflammatory response characterised by the formation of discrete collections of histiocytes called granulomas. Activated histiocytes appear as epithelioid cells with round to oval nuclei, often with irregular contours and abundant granular eosinophilic cytoplasm with indistinct cell borders. They may coalesce to form multinucleated giant cells. When found in the lymph node, the reaction pattern is called granulomatous lymphadenitis. It can be caused by a variety of different conditions, and therefore, requires thorough workup to come to a conclusive diagnosis.
On the basis of presence or absence of necrosis, granulomatous lymphadenitis can be classified as necrotizing or non-necrotizing. Additionally, the presence of an abscess, usually central, indicates a suppurative lymphadenitis.
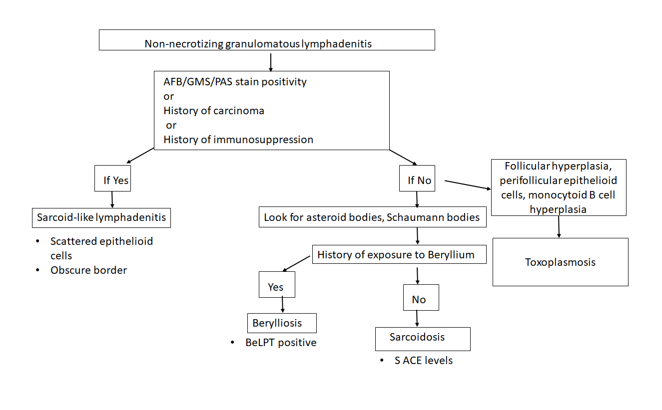
Non-necrotizing granulomatous lymphadenitis:
Sarcoidosis lymphadenitis is the prototype of non-necrotizing granulomatous lymphadenitis. It shows the presence of discrete granulomas without a peripheral rim of lymphocytes, called “naked granulomas”. The early phase shows follicular hyperplasia and sinus histiocytosis, followed by appearance of epithelioid cell nodules toward the end of this phase. The peak phase shows well-demarcated granulomas composed of epithelioid cells with scattered multinucleated giant cells observed throughout the lymph node. Granulomas may occasionally coalesce. In the late phase, increased collagen fibers result in fibrosis and hyalinization. There are no neutrophils and it is uncommon to find small foci of central necrosis. Numerous inclusions such as asteroid, Schaumann, or Hamazaki-Wesenberg bodies can be seen. In this case, we observed well-demarcated granulomas throughout the lymph node, typical of the peak phase without any caseous necrosis or suppuration.
Other causes of granulomatous lymphadenitis can be ruled out as follows.
Sarcoid-like lymphadenitis: It shows a similar pattern of non-necrotizing lymphadenitis like sarcoidosis. However, classically sarcoid like reaction shows scattered small epithelioid granulomas with sparsely arranged epithelioid cells. The border of the granulomas is usually obscure. The CD4:CD8 ratio ranges from 0.8 to 2.25 while in sarcoidosis, it is >3.5. These findings help distinguish sarcoid-like lymphadenitis from sarcoidosis.
Sarcoid-like adenitis may be seen in numerous conditions such as carcinoma, Toxoplasmosis, fungal infections, tuberculosis, immunocompromised states, pneumoconiosis etc. The fact that tuberculosis and fungal infections can present with a non-necrotizing granulomatous lymphadenitis highlights the importance of performing fungal (PAS & GMS) and AFB (Ziehl Neelson) stains in non-necrotizing lymphadenitis as well. In this case, the granulomas had distinct borders, numerous epithelioid cells, no organisms were identified on special stains, nor was there any history of immune compromise; ruling out a sarcoid-like reaction.
Berylliosis: The lymph node picture in Berylliosis is identical to that of sarcoidosis. We may even see asteroid bodies or Schaumann bodies. A diagnosis can be established by eliciting a history of chronic exposure to Beryllium. Beryllium lymphocyte proliferation test (BeLPT) is a test that measures Beryllium sensitization and is very specific for Beryllium exposure. There was no known history of exposure to Beryllium in this case.
Toxoplasmosis: A classic triad of follicular hyperplasia, small granulomas composed of epithelioid cells within and around hyperplastic follicles and, monocytoid B cell hyperplasia, is observed in toxoplasmosis lymphadenitis. This case did not show follicular hyperplasia, ruling out toxoplasmosis.
Necrotizing granulomatous lymphadenitis
Even though we did not find any necrosis in this case, yet, it is worthwhile to review briefly the various causes of necrotizing lymphadenitis.
- Non-suppurative
Tuberculosis: Histology of a tuberculous lymph node is characterised by central caseous necrosis surrounded by an epithelioid cell layer. The outermost layer is comprised of lymphocytes and fibrosis. Plasma cells are not observed. Diagnosis can be established by performing an AFB stain that demonstrates acid fast rod shaped bacteria in the areas of necrosis. Organisms can also be detected by PCR.
BCG lymphadenitis: About 0.7 to 2.3% of BCG vaccinated children may develop BCG lymphadenitis that is smaller than tuberculous lymphadenitis. Early phase shows follicular hyperplasia and sinus histiocytosis. Later, there is development of micronodules of epithelioid granulomas without necrosis and epithelioid cell granulomas with central caseous necrosis. Langhans giant cells are rare.
Fungal infections: Fungal infections by Histoplasma, Cryptococcus, coccidiodomycosis, pneumocystis may also cause a necrotizing granulomatous inflammation. There are numerous neutrophils, and fungal structures can be seen. GMS and PAS can be used in cases where it is difficult to the find the fungal elements on H&E.
- Suppurative
Tularemia: There are three forms of histological changes, Abscess form, showing abscess with central necrosis and mononuclear cells, Abscess-granulomatous form with granulomas with central necrosis, which form large lesions with central abscesses, and granulomatous form with caseating necrosis at the centre of the granulomas.
Cat Scratch disease: Similar to tularemia, there are three phases of histologic presentation, an early phase of follicular hyperplasia, intermediate phase of microabscess, and a late phase of granulomatous inflammation. Monocytoid B cell clusters are observed close to the abscess.
Conclusion
Sarcoidosis is usually diagnosed by excluding other causes of granulomatous inflammation, as we did in this case. Characteristic non-necrotizing, discrete granulomas were seen throughout the lymph node. The age of the patient and female gender epidemiologically support the diagnosis. This case reflects an example work up of a granulomatous lymphadenitis that is a morphologic presentation of myriad diseases.

-Swati Bhardwaj, MD has a special interest in surgical pathology and hematopathology. Follow her on Twitter at @Bhardwaj_swat.

–Kamran M. Mirza, MD, PhD, MLS(ASCP)CM is an Assistant Professor of Pathology and Medical Education at Loyola University Health System. A past top 5 honoree in ASCP’s Forty Under 40, Dr. Mirza was named to The Pathologist’s Power List of 2018. Follow him on twitter @kmirza.
