Case History
A middle aged male presented to the emergency department with a several day history of altered mental status, insomnia, and lethargy. His family stated that he also had possibly had a seizure. Upon arrival to the emergency department he was febrile to 102°F, hypoxic, but denied shortness of breath, cough, nausea, and vomiting. While in the care of the emergency department he had several witnessed seizures requiring Ativan treatment, so the decision was made to admit the patient for 24-hour EEG monitoring. Past medical history was unremarkable. The patient is a smoker. His hobbies include working as a mechanic and working outdoors in his garden.
Initial brain imaging on MRI demonstrated cortical thickening/gyral swelling with associated signal abnormality within bilateral mesial temporal lobes that is seen with mild associated diffusion abnormality. A lumbar puncture was ordered and his CSF analysis demonstrated normal glucose (73 mg/dL [reference range: 40-80 mg/dL]), normal protein (32 mg/dL [reference range: 15-45 mg/dL]), and normal nucleated cells [reference range: 0-8/mm3]. Bacterial, fungal, and AFB culture as well as PCR for herpes simplex virus and varicella zoster virus were ordered. The CSF bacterial, fungal, and AFB cultures showed no growth of any microorganisms, and PCR results were negative for HSV and VZV. What additional infectious etiologies would you like to test for?
Discussion
Serology studies were ordered which demonstrated positive IgM and IgG antibodies for West Nile virus.
West Nile virus is a member of the Flavivirus genus. It is spread through mosquito bites, and birds are the primary reservoir for this virus. The incubation period for West Nile virus is 4-10 days. Typically, about 80% of those infected with the virus will be asymptomatic. In 20% of cases, the patient will develop a febrile illness, with possible symptoms of headaches, body aches, weakness, joint pain, and fatigue. About 1 in 150 of those infected will develop illness involving the central nervous system. In these cases, symptoms can include high fever, headache, neck stiffness, confusion, seizures, and coma. Death occurs in 10% of those with involvement of the central nervous system. The most important risk factor for death is age with patients over 70 years of age being most at risk.
Diagnosis of West Nile virus generally made by detection of IgM and IgG in the serum and/or CSF. IgM can be detected 3-8 days post symptom onset and remains positive for 2-3 months in the CSF, and occasionally longer in the serum. Diagnosis is made by detection of IgM antibodies or conversion of IgG antibodies, while detection of IgG antibodies in isolation indicates a prior infection. False-positive results can occur in CSF specimens contaminated with blood that is IgM antibody positive. Patients who have been infected with or vaccinated against other flaviviruses can have false-positive serum antibodies. Plaque reduction neutralization test (PRNT) assay can be performed to rule out cross-reactivity with other flaviviruses. RT-PCR testing on CSF is also available for detection of West Nile virus RNA. The sensitivity of CSF RT-PCR is low in immunocompetent patients, but increased in immunocompromised patients due to prolonged viremia.
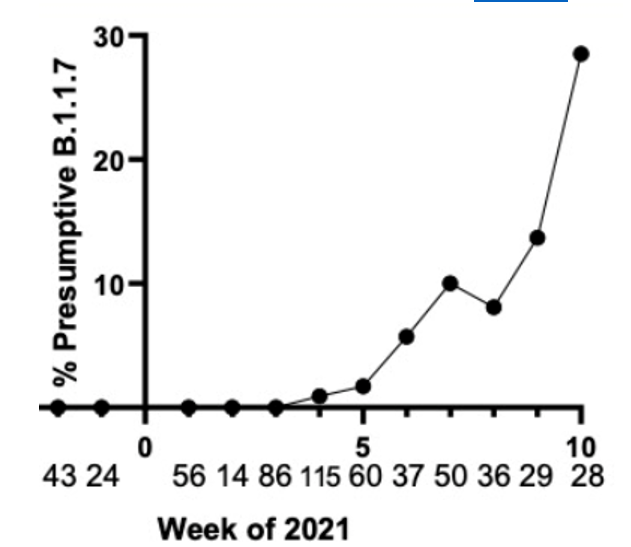
West Nile virus cases could increase in the future as a consequence of climate change. Currently, most cases of West Nile virus occur between June and September and cases have been reported in all 48 lower states. As climate change progresses, average temperatures are expected to increase around the world. As temperature increases, summers become longer, which means a longer season for mosquitoes. Laboratory studies also demonstrate that the virus replicates faster in warmer temperatures. Precipitation patterns are also expected to change in the future. The effect of precipitation is not as clear as that of temperature, but it can still play a role. In areas with more precipitation, increasing amounts of water could provide new breeding grounds for mosquitoes. On the other hand, extra rain can dilute some of the nutrients that the mosquitoes need. In areas with less precipitation, drought conditions can cause rivers to dry up, creating the pools of standing water that give rise to mosquitoes. In addition, as bodies of water become smaller, birds and mosquitoes will be in closer proximity, facilitating faster spread of the virus. We must be prepared for the possibility that West Nile virus cases may be on the rise in the future.
The patient continued to suffer from seizures and required continuous sedation with phenobarbital. For seizure prophylaxis he was given a combination of Keppra and Vimpat, with the dosage adjusted as needed. Throughout his entire hospital course he was monitored on EEG. For the first week of his stay, his EEG results demonstrated seizure like activity, requiring continued use of anti-seizure medication and sedation. After about one week, his seizure activity began to show improvement, and the process of decreasing his medication had begun.
After several days of improvement, his recover was complicated by abdominal compartment syndrome requiring laparotomy. After this, the patient’s seizure activity began to worsen. Within a few days, the patient became hypotensive, and broad spectrum antibiotics were given to protect against infection. Cultures were taken but no infection was identified. The patient ultimately developed shock and passed away.
References
- Paz, S. (2015). Climate change impacts on West Nile virus transmission in a global context. The Royal Society. doi:https://royalsocietypublishing.org/doi/10.1098/rstb.2013.0561
- Murray, P. R., Rosenthal, K. S., & Pfaller, M. A. (2021). Togaviruses and Flaviviruses. In Medical microbiology. Edinburgh: Elsevier.
- Miller, J. Michael, et al. “A guide to utilization of the microbiology laboratory for diagnosis of infectious diseases: 2018 update by the Infectious Diseases Society of America and the American Society for Microbiology.” Clinical Infectious Diseases 67.6 (2018): e1-e94.
-Robert Toelke, MD is a 1st year clinical and anatomic pathology resident at University of Chicago (NorthShore).

-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.