A 40 year old African American female with a history of sickle cell
disease presented to an outpatient clinic with fever, chills, and leg and back
pain consistent with a sickle cell crisis. Her past medical history was also
significant for asthma and seizures. She rated her pain as 10 out of 10, her vitals
showed a temperature of 101.0°F, and she was also tachycardic and hypotensive.
Her white blood cell count was 23.0 TH/cm2, hemoglobin 8.4 g/dL,
hematocrit 26.0%, and platelets 619,000 TH/cm2. In clinic, she
received pain medications and a fluid bolus, two sets of blood cultures were
collected, and she was transferred to the emergency department for further work
up.
Laboratory Identification
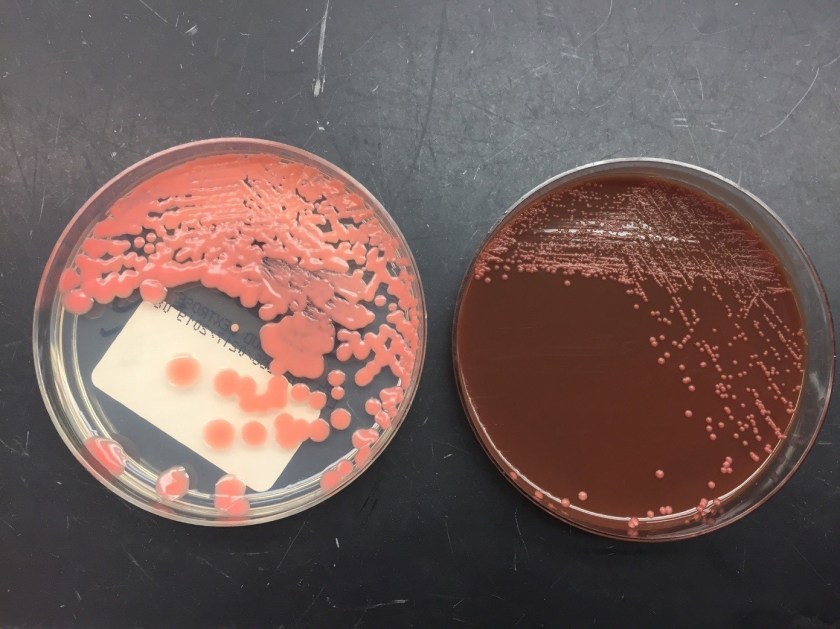
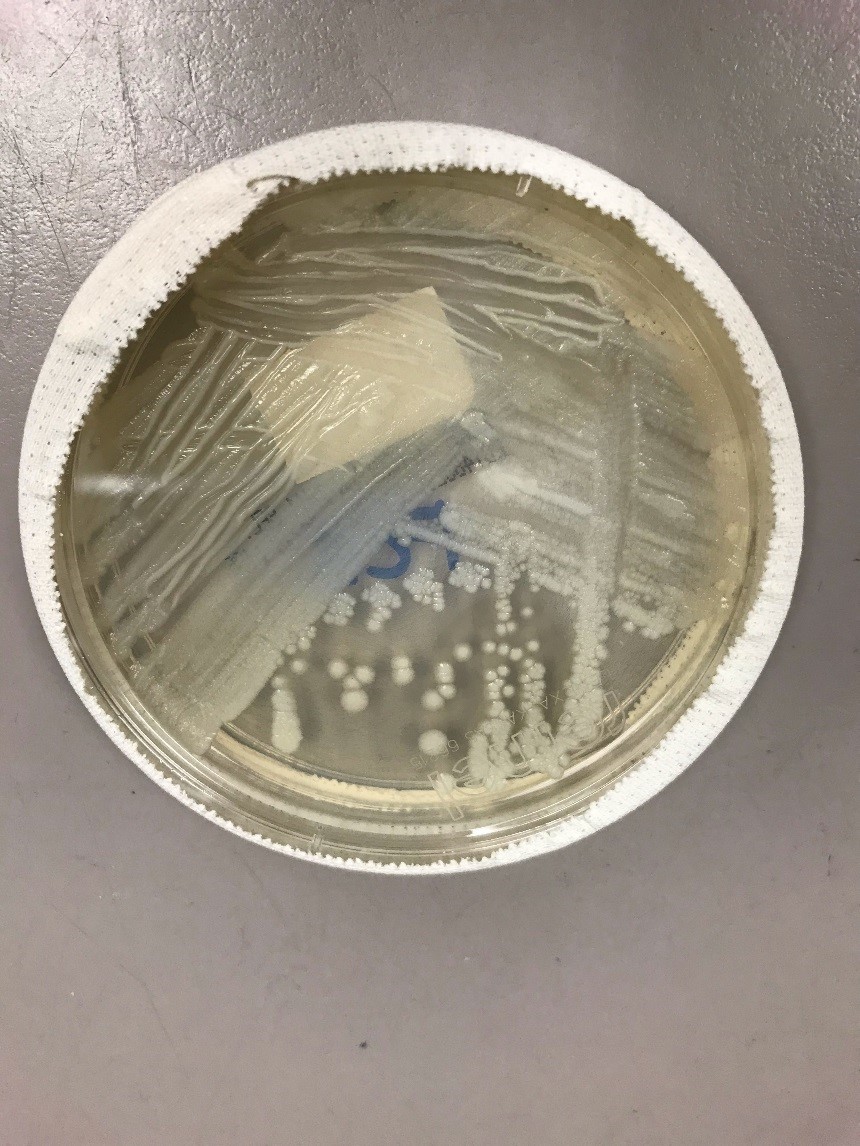
Image 1. Gram stain from a positive blood culture bottle showing small, gram positive budding yeast (1000x oil immersion). Image 2. A mucoid, salmon-colored yeast grew on Sabouraud dextrose and chocolate agars.
Blood culture bottles were positive after approximately two days on the automated instrument. The Gram stain showed small, gram positive budding yeast (Image 1). The BioFire FilmArray for blood culture identification was negative for Candida albicans, C. glabrata, C. krusei, C. parapsilosis, and C. tropicalis. At this time, she was started on micafungin for antifungal therapy. A mucoid, salmon colored yeast grew on both Sabouraud dextrose and chocolate agars (Image 2) and was identified by Vitek 2 as Rhodotorula spp.
Discussion
Rhodotorula spp. are
basidiomycetous yeasts that make up the normal microbiota on moist skin and can
be found in bathtubs and on shower curtains. Rhodotorula spp. are usually considered contaminants, but can
rarely cause fungemia in patients with central lines, endocarditis,
peritonitis, and meningitis, especially in those that are immunocompromised. R. mucilaginosa, R. glutinis, and R. minuta
are the species commonly associated with human disease.
In the laboratory, Rhodotorula
spp. grow as a mucoid, salmon colored yeast within 1-3 days of incubation. On
Gram stain or lactophenol cotton blue prep, the yeast is small and round to
oval with multilateral budding. Pseudohyphae are not usually present. Rhodotorula spp. produce urease and fail
to ferment carbohydrates. R. mucilaginosa
is negative for nitrate assimilation. Identification can also be confirmed by
commercial kits, automated systems, and MALDI-TOF mass spectrometry. Rhodotorula spp. are intrinsically
resistant to echinocandins and fluconazole.
In the case of our patient, she was switched to intravenous
amphotericin B after the identification of Rhodotorula
spp. was made. Reference laboratory testing identified the isolate as R. mucilaginosa with high minimum
inhibitory concentrations (MIC) to fluconazole and echinocandins. Amphotericin
had an MIC of 0.5 µg/ml. She successfully completed a 14 day course with close
monitoring of creatinine, electrolytes, and platelet count. Repeat blood
cultures were negative and no other focuses of infection were found on CT
scans, transthoracic echocardiogram, and ophthalmology exam.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the
University of Mississippi Medical Center in Jackson, MS. She is
certified by the American Board of Pathology in Anatomic and Clinical
Pathology as well as Medical Microbiology. She is the Director of
Clinical Pathology as well as the Microbiology and Serology
Laboratories. Her interests include infectious disease histology,
process and quality improvement, and resident education.
The patient
is a 41 year old male with a history of smoking who presents with a tender,
slowly growing mass on the angle of the left mandible for the past 1 to 1.5
years. The patient also complains of otalgia, but no dysphagia or weight loss.
A computed tomography (CT) scan was performed, which demonstrated a 3.2 x 2.6
cm enhancing mass in the superficial lobe of the left parotid gland with no
significantly enlarged lymph nodes and a patent Stensen’s duct (Image 1). A fine needle aspirate (FNA) was
performed that showed acinic and ductal cells, but was not diagnostic. The
decision was made to take the patient to surgery in order to perform a
parotidectomy.
Image 1. CT scan demonstrating the mass in the left parotid gland (red arrow)
Diagnosis
Received in
the surgical pathology laboratory for intraoperative consultation was a 0.3 x
0.2 x 0.2 cm biopsy of the left superficial lobe parotid gland mass. The tissue
was frozen, stained and read out as an “acinic cell neoplasm”. Following the
frozen diagnosis, the main specimen was received for routine processing,
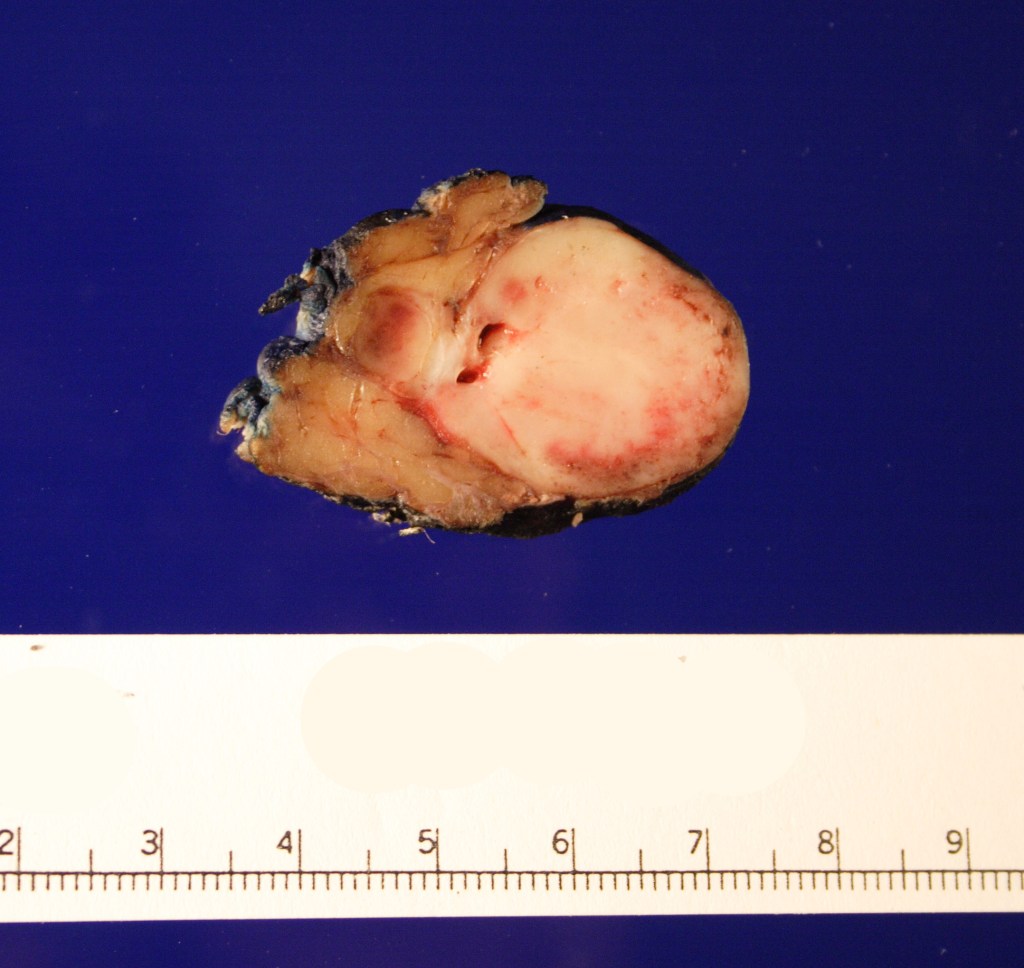
weighing 19.0 gm and measuring 4.0 x 4.0 x 3.0 cm. The specimen was unoriented
and entirely inked black. It was serially sectioned revealing a 2.5 x 2.5 x 2.4
cm tan, friable, well-circumscribed mass and surrounding tan-brown,
beefy-appearing parotid tissue (Image 2). A second tan-brown nodule measuring
1.5 x 1.0 x 0.8 cm abuts the larger tan mass. Representative sections of the
larger mass are submitted in cassettes 1-8, and the smaller nodule is entirely
submitted in cassettes 9 and 10.
Image 2. Cut surface of the parotid gland demonstrating the well-circumscribed tan mass
Microscopy
demonstrates a low-grade, very well differentiated tumor consistent with an
acinic cell carcinoma with complete inked surfaces (i.e. the mass has not been
transected and excision appears complete). There is a small focus of capsular
“disruption”/parenchymal hemorrhage, which most likely corresponds to
the area sampled for intraoperative consultation. In addition, there are two
separate benign periparotid lymph nodes.
Discussion
Acinic cell
carcinoma (ACC) is a rare tumor of the parotid gland, representing 2 to 4% of
all primary parotid gland neoplasms. It is the second most common childhood
salivary gland malignancy behind mucoepidermoid carcinoma, but has been found
throughout the age range. There is a gender predilection, as ACC is found in
females more than males in a 3:2 ratio. One of the first cases of ACC dates
back to 1892, in which the tumor was diagnosed as being a “blue dot tumor”,
thought to be called this due to the intracytoplasmic zymogen granules.
Clinically,
ACC presents as a slowing growing mass in the salivary glands, most commonly in
the parotid gland. Other symptoms are not commonly found until late in the
diagnosis, and include pain, facial nerve palsy, and nodal disease. There have
also been cases of ACC that arise in the minor salivary glands. Unlike minor
salivary gland carcinomas that arise in the palate, ACC of the minor salivary
glands will mostly be found in the buccal mucosa and upper lip.
Grossly, ACC
presents as a round, well-circumscribed to variably encapsulated mass with a
rubbery, gray-tan, solid to cystic cut surface, commonly with areas of
hemorrhage and necrosis. Histologically, the mass will be composed of acinar
type cells with basophilic granular cytoplasm, clear cells with glycogen or
mucin, intercalated ducts, non-specific glandular cells and a few mitotic
figures. ACC is defined by the World Health Organization as a malignant
epithelial neoplasm of the salivary glands in which at least some of the
neoplastic cells demonstrate serous acinar cell differentiation, which is
characterized by zymogen secretory granules, and can also include salivary
ductal cells (Image 3). It is common for sections taken of ACC to show
microscopic invasion of the capsule with nests of tumor cells outside the
capsule. There are four histologic patterns that were described by Abrams et al
in 1965 that are still applicable today: solid, microcystic, papillary cystic
and follicular. Immunohistochemical stains, if needed, will be positive for
keratin, alpha-1-antichymotrypsin and alpha amylase. It can be difficult to
distinguish ACC from normal acini or benign salivary gland tumors (leading to a
false negative result) on cytology due to the absence of any hallmark malignancy
features such as necrosis and pleomorphism, but centrally placed large nuclei, distinct
nucleoli, binucleated cells, and ill-defined cell borders can help make this
distinction. The same caution applies to aspirates because if the tumor is
cystic, it may be interpreted as being hypocellular and deemed to be a benign
salivary cyst.
Image 3. Photomicrograph demonstrating the zymogen granules within the cytoplasm of the cells
Imaging by
ultrasound, CT and magnetic resonance imaging (MRI) can prove to be worrisome
as similar with cytology, the scans can demonstrate a mass with benign
features, and thus a more favorable diagnosis. On ultrasound, ACC will appear
lobular, well-defined, hypoechoic and poorly vascularized. Ultrasound can be useful
help to determine the size and location of the mass, as well to help with
ultrasound guided fine needle biopsies. On CT, the mass will appear
non-specific with limited heterogenous enhancement but can be used to
demonstrate the relationship of the mass to the facial nerve, and to identify
any distant metastases. On MRI, ACC can have a nonspecific intensity pattern
similar to benign salivary gland neoplasms, but low T1 and T2 signals can help suggest
vascularity, fibrosis and calcification within the mass. In addition, MRI can
help in assessing the parotid gland, stylomastoid foramen, and any possible
facial nerve invasion or perineural invasion.
Risk factors
for the development of ACC include radiation exposure and familial
predisposition. Risk factors for the development of salivary gland tumors, but
not necessarily ACC, include radiation exposure, the use of iodine 131 in the
treatment of thyroid disease (isotope is concentrated in the salivary glands),
and working with materials in certain industries, such as those that use
asbestos and rubber manufacturing, metal in the plumbing industries, and
woodworking in automobile industries.
Complete
surgical excision is considered the primary treatment option, with
postoperative radiotherapy in cases of incomplete removal, recurrence,
undifferentiated ACC, positive margins, and cervical lymph node metastasis. Removal
of the facial nerve may be necessary in T3 and T4 cases, as well as a possible
neck dissection. As of now, ACC has been considered chemo-resistant, and
treatment with chemotherapy is not suggested. Around 35% of tumors will recur,
and that percentage rises to 80-90% if the tumor is incompletely excised. ACC
has a 5 year survival rate of 90%, a 10 year survival rate of 88%, and there
have even been of cases of recurrence occurring up to 30 years after the
initial procedure. If metastasis was to occur, although rare, the spread tends
to be more hematogenous than lymphatic, with the most common sites being the
lungs and bones.
References
Al-Zaher N, Obeid A, Al-Salam S, Al-Kayyali BS. Acinic cell
carcinoma of the salivary glands: a literature review. Hematol Oncol Stem Cell Ther. 2009;2(1):259-64.
Bury D, Dafalla M,
Ahmed S, Hellquist H. High grade transformation of salivary gland acinic cell
carcinoma with emphasis on histological diagnosis and clinical implication. Pathol Res Pract. 2016;212(11):1059-1063.
DOI: 10.1016/j.prp.2016.08.005.
Rosero DS, Alvarez
R, Gambó P, et al. Acinic Cell Carcinoma of the Parotid Gland with Four
Morphological Features. Iran J Pathol. 2016;11(2):181–185.
Vander
Poorten V, Triantafyllou A, Thompson LD, et al. Salivary acinic cell carcinoma:
reappraisal and update. Eur Arch
Otorhinolaryngol. 2016;273(11):3511-3531. DOI: 10.1007/s00405-015-3855-7
-Cory Nash is a board certified Pathologists’ Assistant,
specializing in surgical and gross pathology. He currently works as a
Pathologists’ Assistant at the University of Chicago Medical Center. His
job involves the macroscopic examination, dissection and tissue
submission of surgical specimens, ranging from biopsies to multi-organ
resections. Cory has a special interest in head and neck pathology, as
well as bone and soft tissue pathology. Cory can be followed on twitter
at @iplaywithorgans.
A
4 year old child was brought to the pediatrician by her mother with a complaint
of new onset of severe bruising on her legs. The mother could not recall any
falls or bumps that would have caused the bruising. On exam, the physician also
noted mucosal bleeding in the oral cavity. Questioning revealed that the
patient had experienced flu like symptoms several weeks earlier. The physical
exam was normal except for the bleeding. There was no family history of
bleeding disorders. A CBC was ordered.
Reported
CBC Results
WBC,
RBC, Hgb, Hct, RBC indicies normal
Platelet
count 26 x 103/μL
IPF
22% (reference range IPF% 1.0-7.0%)
The physician evaluated the results, noting the
normal CBC but decreased platelet count. The above results also show the
immature platelet fraction (IPF), an additional Advanced Clinical Parameter reported
from the Sysmex XN hematology analyzer. A low platelet count, as seen in this
patient, will reflex a fluorescent platelet count (PLT-F). The impedance count (PLT-I)
can be falsely increased if small RBCs or fragments are counted as platelets. On the other hand, in an optical
platelet count, when measuring platelets by size (PLT-O), large platelets can
be missed, giving a falsely low count. In this case there was a low
platelet count and an instrument flag for an abnormal platelet scattergram. The PLT-F, on the other hand, uses a
platelet specific dye which eliminates interference seen with other methods.
The fluorescent dye labels the RNA, and forward scatter is used to determine
size while side fluorescence is used to measure RNA content. With gating set
based on cell volume and RNA content, the PLT-F can be measured. Therefore,
the reflexed and more reliable
PLT-F was the reported count.
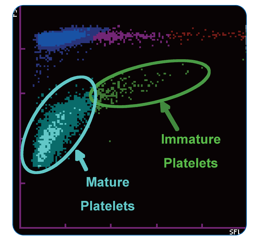
Figure 1. PLT-F scattergram. The PLT-F channel measures forward scatter (FSC) on the Y axis and side fluorescence (SFL) on the X axis.1
Additionally, when there is an abnormal
scattergram or a low platelet count, the IPF% and IPF# are also reported. The immature
platelet fraction is a measure of the youngest platelets, or reticulated
platelets. These are the first circulating platelets, right out of the bone
marrow. An increased IPF indicates an increase in platelet production, yet this
child’s platelet count was very low. This suggests that the thrombocytopenia
may be due to excessive destruction of platelets; the bone marrow was actively
making platelets, but they were being destroyed, causing the low platelet
count.
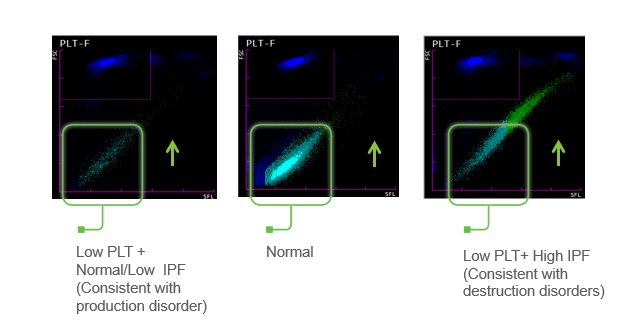
Figure 2. Platelet scattergrams from a healthy individual with a normal IPF (a) and a patient with a high IPF (b). Mature platelets appear as blue dots, green dots represent the IPF with increased cell volume and higher fluorescence intensity compared to mature platelets.1
Diagnosis
Immune Thrombocytopenia- ITP.
Primary immune thrombocytopenia (ITP), formerly
known as idiopathic thrombocytopenic purpura or immune
thrombocytopenic purpura, is one of the most common bleeding
disorders of children. In most cases, it presents with sudden onset of bruising
and petechiae in an otherwise healthy child, with normal WBC and hemoglobin. ITP is an
autoimmune bleeding disorder in which the immune system makes anti-platelet
antibodies which bind to platelets and cause destruction. Even though the exact
cause of ITP remains unknown, it is recognized that it can follow a viral
infection or live vaccinations. While there are some similarities between
pediatric ITP and ITP in adults, in children this tends to be an acute disease
which is self-limiting and resolves itself in several weeks, with no treatment.
However, in a small number of children, the disorder may progress to a chronic
ITP. In contrast to ITP in children, a chronic form is more commonly seen in
adults. It is usually a diagnosis of exclusion, does not follow a viral illness
and requires treatment.
This
patient recovered in a few weeks. One month after the initial episode, her PLT
was 174 x 103/μL and her IPF% was 6.0%
Conclusion
An IPF reported with a CBC, in combination with a low platelet count, is fast, inexpensive, and can be extremely beneficial in aiding in a timely diagnosis. As the child’s platelet count recovered, the IPF% returned to normal range. ITP can therefore be monitored with a CBC. Thus, the IPF can be used not only to help diagnose but also as an indicator of remission.
Arshi Naz et al. Importance of Immature platelet
Fraction as a predictor of immune thrombocytopenic purpura. Pak J Med Sci 2016
Vol 32 No 3:575-579
Briggs,C. Assessment of an immature plateletfraction
(IPF) in peripheral thrombocytopenia. Br J Haematol 2004Jul;126(1):93-9
Sysmex White Paper. The role of the ImmaturePlatelet
Fraction(IPF) in the differential diagnosis of thrombocytopenia. www.sysmex.com/us
D-Orazio, JA, Neely, J, Farhoudi,N. ITP in children: pathophysiology and current
treatment approaches.J Pediatr Hematol Oncol.2013 Jan;35(1): 1-13
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
A 35 year old female with a history of BRCA-positive breast
cancer (status-post right radical mastectomy February 2018) underwent
prophylactic left mastectomy and revision of right mastectomy. She received
prophylactic clindamycin and cefazolin. She was discharged on post-op day 5
with bacitracin and 3 weeks of cefadroxil. She initially healed well. On
post-op day 43 she noted drainage from the left incision site. At presentation
she was afebrile. There was a 3.0 x 2.0
cm area of induration and erythema on the right lateral aspect of her abdominal
incision with seropurulent drainage. Incision and drainage was performed in
office and a swab of the fluid was sent to microbiology. The initial gram stain
and cultures were negative for bacteria. The patient was placed on sulfamethoxazole-trimethoprim
and levofloxacin. At follow up 7 days later, another abscess was medial to the
prior site was incised and drained. A swab of the fluid was sent to
microbiology for bacterial and fungal cultures.
Laboratory
Identification
Fungal cultures grew at 36 hours on potato-flake agar. Gram
stain revealed gram-variable bacilli. Growth on 7H10 agar produced colonies at
72 hours, and Kinyoun staining was positive for acid-fast bacilli. Matrix
assisted laser desorption ionization-time of flight mass spectrometry
(MALDI-TOF) at 72 hours identified Mycobacterium
abscessus complex.
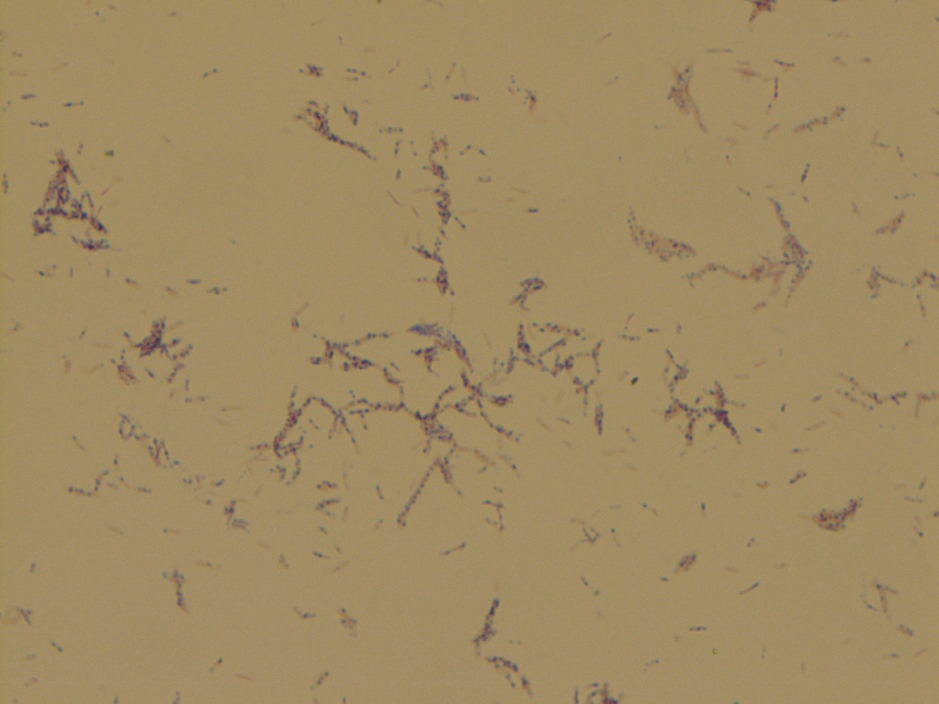
Image 1. Growth on 7H10 agar. Image 2. Gram stain from 7H10 agar showing gram variable bacilli. Image 3. Kinyoun stain showing acid-fast bacilli.
Discussion
M. abscessus complex is a group of rapidly-growing, nontuberculous mycobacteria. As such they are acid-fast bacilli that grow within 7 days when transferred from solid media to solid media. The subspecies are M. abscessus abscessus, M. abscessus massiliense, and M. abscessusbolletii. The complex is known to cause progressive pulmonary disease in patients with underlying structural lung diseases. It has been estimated to comprise up to 13% of all mycobacterial pulmonary infections. It has also been implicated in skin and soft tissue infections (SSTIs) following surgical procedures or environmental exposure (i.e. spas). SSTIs can also occur by seeding from disseminated disease. Rarer manifestations include central nervous system (CNS) and ocular involvement. Identification is by culture and molecular techniques. It is classically resistant to many drug classes with limited consensus on appropriate therapy. It can harbor the erm gene, which confers inducible erythromycin resistance. Clarithromycin, amikacin, and cefoxitin tend to have the lowest rates of resistance. Long-term multidrug regimens are recommended, based on susceptibility testing. Changes to initial therapy are usually required due to side effects or lack of efficacy. Surgical therapy is often required, when possible. Mortality post therapy is approximately 15%.
At two-week follow up, the wound had no purulent drainage or
erythema. The plan was for prolonged three-drug therapy tailored to susceptibility
data.
Griffith DE. Rapidly growing mycobacterial
infections: Mycobacteria abscessus, chelonae, and fortuitum. Von Reyn CF and B
A, eds. UpToDate. Waltham, MA: UpToDate Inc. https://www.uptodate.com (Accessed
on May 21, 2019.)
Lee MR, Sheng WH, Hung CC, Yu CJ, Lee LN, Hsueh
PR. Mycobacterium abscessus Complex Infections in Humans. Emerg Infect
Dis. 2015;21(9):1638–1646.
Novosad SA, Beekmann SE, Polgreen PM, et al.
Treatment of Mycobacterium abscessus Infection. Emerging Infectious Diseases.
2016;22(3):511-514.
-Jonathan Wilcock, MD is a 1st
year anatomic and clinical pathology resident at the University of Vermont
Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
As laboratory safety professionals, we know that an important part of the job is the ability to coach other lab team members when unsafe situations are observed. To coach someone is to confront a coworker about an issue for the sake of safety-theirs, yours, or that of a patient. Those coworkers may be fellow lab employees, supervisors, managers, or even physicians. The word “confront” might sound strong, particularly to those who may be uncomfortable with these types of encounters, but this coaching is an important and valuable skill.
Coaching your peers is no easy task, and it takes practice to be able to do it well. I recently walked into a laboratory that was unfamiliar to me, and I saw a technologist working at the bench with no lab coat, no gloves, and no face protection. At first I thought, “that would never happen in a one of my labs,” and then, “the lab safety culture here is terrible.”
I learned I was wrong on both counts, and the incident reminded me of the necessity to stop and think before forming an opinion or even speaking about a lab safety issue. I provide training often about how to coach staff who are acting unsafely while in the lab, and I have learned that how a coaching moment will go depends largely on what is in the head of the coach before he or she speaks. It is important to remember that if someone acts in a manner that displeases or disappoints you, there are several possible sources of influence acting on that person.
Psychologists have coined it the “Fundamental Attribution Error.” Humans who are disappointed usually think the other person has committed the wrong intentionally or because they are not intelligent. Neither of these conclusions is ever correct, and that thought process usually leads to a coaching session that will not be successful.
Take the scenario I mentioned above, for example. What is your gut reaction when you see someone working in a lab without PPE? Maybe that lab tech just found out a relative had passed away and they were waiting for someone to relieve them, or maybe there were no lab coats or gloves available in their size. The possibilities are endless, so you need to train yourself to be calm first and to ask questions to learn what is really happening without making assumptions. It’s more difficult to do than one would think.
The success of a safety coaching moment is determined in your head before you even speak. You have the power to make it a positive event. It is true that some people just will not accept it well no matter what we do (a reminder to ourselves to always be ready to accept coaching), but by and large a successful event starts in the mind of the person who is coaching for safety.
When you see a lab safety problem, it is vital that you confront the person. However, before you do so, ask yourself, “why would a rational person behave this way? What am I not seeing here?” If you start with that, your coaching for safety will be much more successful, and you will see a positive change in your overall lab safety culture.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
This is not your Mom’s PCR. These new kids on the block are making
PCR extremely fast. PCR (Polymerase Chain Reaction) technology won the Nobel Prize
for allowing molecular research to advance much more rapidly (for an
interesting read on the quirky Laureate who gave up science to go surfing, read
more here: Wikipedia ). It has become the most commonly used work horse of most
molecular diagnostic assays, usually in the form of real-time PCR. It is used
for a variety of purposes from detecting bacteria and viruses, identity testing
for forensics and bone marrow engraftment, cancer mutation analysis, and even
sequencing by synthesis used by Illumina for massively parallel sequencing.
This technique is still limited by requiring highly trained
technologists to perform DNA extraction, time-consuming processing, and the
time of real-time PCR itself. Overall, this process takes about a 5-8 hours. While this is much faster
than in the past, it would be unacceptable for use in the point-of-care (POC).
But why would DNA testing need to be POC? The term sounds like an
oxymoron in a field where many results have a 2-month turnaround time. There are certain circumstances where molecular
testing would impact patient care. For instance, a doctor testing a patient in
their office for a sexually transmitted infection would want to know if they
have gonorrhea/ chlamydia so they could prescribe proper antibiotics. Similarly,
POC molecular testing could be applied in a bioterrorism incident to test
samples for an infectious agent. Or POC testing would benefit low-resource
areas internationally where HIV testing could be used to manage anti-retroviral
therapy in patients many miles from a laboratory.
For PCR as a test to be useful at the POC setting, it would have
to provide a result within 10-15 minutes and be performed as a waived test. Two
recent examples the demonstrate how this is possible have been highlighted at
recent conferences of the American Association of Clinical Chemistry, which I
just got back from: Extreme PCR1
and Laser-PCR.2
Extreme PCR refers to a technique of rapidly cycling the temperature of PCR reactions. The reaction occurs in a thin slide that evenly distributes the reagents, temperature and is clear to permit easy reading of fluorescence measurements (Figure 1). DNA Polymerase enzyme and primers to amplify the target DNA are added at much higher concentrations than normal (20x).
Figure 1. Thin reaction chamber for ultra-fast PCR.
This flies in the face of traditional PCR chemistry dogma as
specificity would plummet and normal DNA could be amplified instead of target
DNA. This would create a false positive. However, let’s think about what is
actually happening with non-specific reactions. Primers are designed to match
one region of DNA, which is very unique within
the whole genome. However, the genome is so large that some segment may look
very similar and be different in just 1 or 2 of the 20 base pairs that a primer
matches. A primer could bind to this alternate region but less efficiently. So,
the binding would be weaker and take
more time to occur.
Therefore, by speeding up the cycling time to just a few seconds, only the most specific interactions can take place and non-specific binding is offset (Figure 2)!
Figure 2. Fluorescence from a dye that fluoresces when bound to double stranded DNA, which is increasing here within seconds (high point represents when the reaction temperature cools and dsDNA anneals, then low points represent heating to high temperatures).
Laser PCR does not report the use of increased reagents like Extreme PCR (it may be proprietary), but they boast a very innovative method to quickly heat and cool PCR reactions. GNA Biosciences use gold nanoparticles with many DNA adapters attached (Watch the video below for a great visual explanation!).
These adapters are short sequences of DNA that bring the target
DNA and primers together to amplify the target DNA sequence. Then as the name
implies, a laser zaps the gold beads and heats
them up in a very localized area that releases the DNA strands. The
released DNA binds another gold particle, replicates, rinses, and repeats. The
laser energy thus heats the gold in a small area that allows for quick heating and cooling within a
matter of seconds.
These new PCR methods are very interesting and can have a big
impact on changing how molecular pathology advances are brought to the patient.
On a scientific note, I hope you found them as fascinating as I did!
References
Myrick JT,
Pryor RJ, Palais RA, Ison SJ, Sanford L, Dwight ZL, et al. Integrated extreme
real-time PCR and high-speed melting analysis in 52 to 87 seconds. Clin Chem
2019;65:263–71.
G. Mike
Makrigiorgos. Extreme PCR Meets High-Speed Melting: A Step Closer to Molecular
Diagnostics “While You Wait” Clin Chem 2019.
-Jeff SoRelle, MD is a Chief Resident of Pathology at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and improving genetic variant interpretation.
A
55 year old male presented to the emergency department (ED) with altered mental
status (AMS). His past medical history includes stage 4 pancreatic cancer with
known invasion into the distal splenic vein. Currently undergoing chemotherapy,
his last infusion was one week prior to presentation. On physical exam, the
patient is a cachectic male with dry mucous membranes, scleral icterus,
hypotension (79/37), hypothermia (35o C), tachypnea (Respiratory
Rate of 20/min) and tachycardia (pulse up to 130s). Initial labs were ordered
including blood cultures and were significant for hypoglycemia (40mg/dL),
pancytopenia, mild liver function test abnormalities, an ammonia level of 80
µmol/L and lactate of 11.2 mmol/L. It was concluded that the AMS resulted as a consequence
of hypoglycemia. However, there was also concern for intracranial pathology vs.
stroke vs. metastatic disease. Brain imaging showed no obvious lesion or mass.
The cause of the hypotension was uncertain but could be a result of volume depletion
or sepsis. Empiric vancomycin and cefepime were initiated in the ED. However,
the patient decompensated, developing mid-abdominal and periumbilical
ecchymoses suspicious for a retroperitoneal hemorrhage. Despite aggressive
therapy, he expired in the ED.
Laboratory Identification
An
anaerobic blood culture bottle flagged positive at 5 hours incubation. A gram
stain showed large, boxy, gram positive rods without spores (Image 1). Brucella
blood agar was inoculated and incubated anaerobically. Following overnight incubation, the surface
of the plate showed a subtle film of growth covering the plate and detectable
hemolysis (Image 2). No discreet colonies were identified. A catalase test was
performed and was negative. Definitive identification of Clostridium septicum was
obtained by MALDI-TOF.
Image 1. Gram stain from the anaerobic blood culture bottle that flagged as positive following 5 hours of incubation. Boxy, large gram positive rods without spores are observed. Oil immersion photomicrograph (x100 objective). Image 2. Brucella agar plate following 24 hours of incubation under anaerobic conditions at 35oC. Significant bacterial growth in a haze and detectable Beta hemolysis can be observed. No discreet colonies can be identified. Identification by MALDI-TOF was Clostridium septicum.
Discussion
Clostridium septicum is an anaerobic gram positive bacillus that
can produce spores; however, spores are not frequently seen, especially in
nutrient-rich environments. Spores, when present, are typically oval and
located subterminally. Infection by C.
septicum was once thought to be extremely rare, but improvements in
anaerobic laboratory techniques have allowed for the discovery of the true
potential of this agent. C. septicum
is one of several bacteria that can cause myonecrosis (i.e., gas gangrene). Infections are typically seen in settings of immunodeficiency,
trauma, surgery, malignancy, skin infections/burns,
and septic abortions. The colon may promote
the growth of C. septicum better
than other anatomic sites due to its anaerobic conditions. As one of the
more aggressive etiologies of gas gangrene, C. septicum infection
progresses very rapidly, with a mortality rate of approximately 79% in adults,
typically occurring within 48 hours of infection. Symptoms of infection
include pain, described as a heaviness or pressure that is disproportionate to
physical findings, tachycardia, and hypotension. Tissue necrosis then causes
edema and ischemia resulting in metabolic acidosis, fever, and renal failure.
The carbon dioxide and hydrogen produced during the growth of the organism move
through tissue planes, causing their separation, producing features
characteristic of palpable emphysema (i.e., crepitus). This also results in a
magenta-bronze skin discoloration and bulla filled with a foul-smelling
serosanguinous fluid.
Four
toxins have been isolated from C.
septicum: the lethal alpha toxin, DNase beta-toxin, hyaluronidase gamma toxin, and the thiol-activated/septicolysin delta
toxin. Alpha toxin causes intravascular hemolysis and tissue necrosis and is well known as the primary virulence factor of C.
septicum.
C. septicum derived gas gangrene has shown strong correlations with increased levels
of malignancy. Patients with C. septicum infections may have an
occult colon cancer or a tumor that has metastasized to the colon. C. septicum bacteremia is also
associated with typhlitis (defined as inflammation of the cecum that can extend
proximally into the terminal ileum or distally into the ascending colon), which
can develop in patients with hematologic malignancy receiving chemotherapy.
Because the organism may be harbored in the gastrointestinal tract, the
organism may gain access to the bloodstream through the ileocecal region.
Therapy
includes antibiotics and surgical debridement (with occasional amputation). For
antibiotic selection, typical anaerobic coverage includes
piperacillin/tazobactam, ampicillin/sulbactam, metronidazole or meropenem.
Vancomycin is also effective. Susceptibility testing is not typically
performed; moreover, the CLSI makes an annual antibiogram which can be used as
a guide.
Key points
C. septicum often has swarming growth that covers the plate surface.
Spontaneous myonecrosis with C. septicum bacteremia can be an indicator of possible occult colonic malignancy.
C. septicum can be associated with typhlitis in neutropenic patients with hematologic malignancy undergoing chemotherapy.
References
Smith-Slatas CL, Bourque M, and Salazar JC (2006). Clostridium septicum infections in children: a case report and review of the literature. Pediatrics 117(4): e796-e805.
Alpern, RJ and Dowell, VR (1969). “Clostridium septicum infections and malignancy”. JAMA. 209: 385–388.
Ballard, J, Crabtree, J, Roe, BA, and Tweten, RK (1995). “The primary structure of Clostridium septicum alpha-toxin exhibits similarity with that of Aeromonas hydrophila aerolysin”. Infection and Immunity. 63 (1):340–344.
Sidhu JS, Mandal A, Virk J, and Gayam V (2019). “Early detection of colon cancer following incidental finding of Clostridium septicum bacteremia”. J Investig Med High Impact Case Rep. Jan-Dec;7:2324709619832050.
Srivastava I, Aldape MJ, Bryant AE, and Stevens DL. (2017). “Spontaneous C. septicum gas gangrene: A literature review” Anaerobe. Dec;48:165-171
–Xiang Xu, MD, PhD and Dominick Cavuoti, DO
contributed to this case.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. he has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
In 2017, Puerto Rico had a very challenging year with both
Hurricane Irma and Maria bombarding its shores. Just last month, Puerto Rico
was spared a hit from Dorian. However, a major storm (of sorts) will be hitting
Puerto Rico on September 30, 2019, regardless of what the weather says. On that
day, the Section 2005 of the Affordable Care Act expires which provided PR with
$5.4 Billion in Medicaid funding (from July 1, 2011 to September 30, 2019). If
it were any other state of the United States, the expiration of this relief
funding would not be such a challenge because of the current matching programs
afforded to those states by the federal government. However, PR is unique in
that it is only provided a block grant (i.e., a set amount of money) and that
block grant is significantly lower than what other states get overall. Based on
current estimations of costs in PR, the block grant funding will be exhausted
by March 2020. At that point (well after hurricane season), PR will have to
cover all costs for Medicaid for its citizens 100%. Why is that a problem?
In order to understand this, we have to look at PR’s
healthcare system (removing the stress, strain, and destruction on the system
delivered by Irma and Maria) in its base state. The public health care system
in PR was privatized and now includes forced managed care participation. Of the
3 million citizens living in PR (which is on the decline), more than half are
covered by Medicaid. The Medicaid eligibility limits in PR are much lower than
other states ($6,600 in PR vs. $17,236) and with other states ability to expand
coverage to 138% of the poverty line, PR can not go above 40% of the poverty
line. This leaves a significant portion of the population ineligible. The cost
of living in PR is actually higher than many mainland states while the average
income is much lower. The per enrollee Medicaid benefit in PR is $2,144
compared with the lowest mainland state ($3,342) and the median state ($6,763)
for projected 2020 budgets. If PR were afforded the same system of delegating
funds from Medicaid to its enrolled citizens (i.e., matching based on income),
the Medicaid matching rate would be 83%; however, because of the block grant
the effective matching rate is between 15 and 20% for PR. Reimbursements for
equivalent services in the mainland US are significant less in PR (for example,
as low as $10 to a physician for an office visit). Unlike other mainland
states, a US federal act (PROMESA) created an oversight board (FOMB) to manage
the island’s finances and one of the main tools of the FOMB to control costs in
PR has been to deeply cut Medicaid spending.
Given that situation, it should not be surprising that prior
to the 2017 crisis, healthcare professionals were leaving PR in large numbers
and that trend increased after 2018. In an effort to stem this exodus, Act
14-2017 was enacted (February of 2017) which reduced certain physicians’ income
tax in PR to 4% (down from 33%). This act went into effect in April of 2017 but
data show physicians continue to leave, evidence that physicians value ability
to care for their patients (i.e., resources to provide quality care) over their
own income. Jennifer Gonzalez-Colon, the resident commissioner for PR (the only
representative to Congress with limited voting rights and a marginalized role)
introduced the Puerto
Rico Integrity in Medicare Advantage Act in September of 2018 to stabilized
Medicaid payments in PR following Maria (as an amendment to XVIII of the Social
Security Act), which would have improved payments including to physician
providers. The Act died in when the 115th Congress concluded in 2019
having never been enacted.
PR’s Medicaid program is, thus, in a crisis situation which
will either need to be resolved before March 2020 or will result in potentially
increased challenges (i.e., assuming additional healthcare professionals leave
the island). With an already aging healthcare professional population (i.e.,
young professionals leave) and an aging population of patients, an enormous storm
that has been brewing for years will be unleashed in the spring. The solution
is for those controlling the healthcare finances of the island to create
equitable systems of payment to support the US citizens of PR.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
The patient is a 69 year old male who presented to the
hospital with a 3-month history of drenching night sweats, weight loss, fatigue,
and generalized lymphadenopathy. He also endorsed a very itchy rash all over
his body. He denied smoking. There was no other relevant social or family
history.
Physical examination confirmed diffuse lymphadenopathy,
hepatosplenomegaly and a mild diffuse skin rash. Notably, there was a 2.5 cm
level-1 lymph node palpated in the left neck. This was subsequently biopsied.
Biopsy
Biopsy of the level-1 neck lymph node revealed a 2.3 x 1.5 x
1.2 cm mass pink-tan and firm mass. Sectioning revealed a glossy white-tan cut surface.
H&E staining revealed a polymorphic lymphocytic infiltrate of in the interfollicular
zones. The infiltrating lymphocytes ranged from small to large cells with abundant
cytoplasm, eosinophils, and plasma cells. There was also a notable increase in
the number of high endothelial vessels lined by lymphocytes with irregular
nuclear borders and clear cytoplasmic zones.
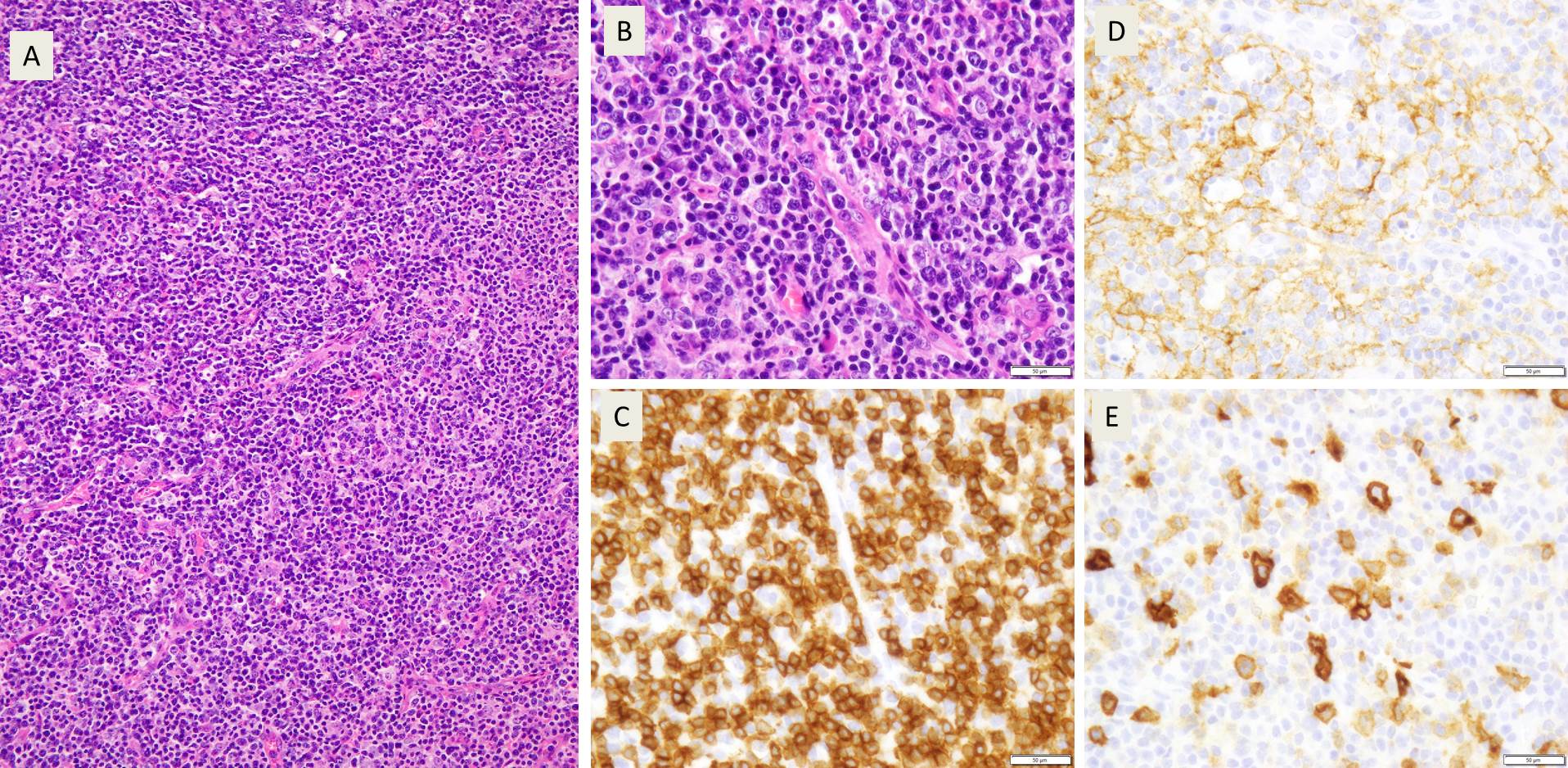
Image 1. Polymorphic infiltrate of small, mature appearing lymphocytes (A), with prominent blood vessels and clear cytoplasm (B). Most of these cells were CD3 positive T cells (C) with expanded CD21 positive FDC meshworks (D) and scattered CD30 positive immunoblasts (E)
Further characterization by immunohistochemical staining showed
the majority of the interfollicular cells to be CD3 and CD5 expressing T cells.
These were a mix of CD4 and CD8 positive cells but with marked CD4
predominance. CD7 appeared positive in a smaller population of T-cells compared
to CD3 (consistent with loss of this pan-T-cell marker). Varying numbers of the
interfollicular cells were positive for CD10, BCL-6, CXCL-13, and PD-1 with a
strong positivity for ICOS, phenotypically consistent with an expansion of Tfh
(T-follicular helper cell) cells.
Interspersed between the T cells were numerous CD20 positive
cells with prominent nucleoli that also revealed CD30 positivity. CD21 staining
revealed expanded follicular dendritic cell meshworks. EBER ISH was positive in
a rare subset of cells. Kappa and lambda ISH showed an increased number of
polytypic plasma cells.
Flow Cytometry showed the presence of a small population of
T-cells that were CD4 positive but CD3 negative. There was no evidence of
B-cell clonality. TCR-G PCR was positive.
A final diagnosis of Angioimmunoblastic T-cell lymphoma
(AITL) was rendered.
Discussion
AITL is a relatively rare neoplasm of mature T follicular
helper cells, representing about 1-2% of all non-Hodgkin lymphomas. It is;
however, one of the more common subtypes of peripheral T-cell lymphomas,
accounting for 15-30% of this subgroup. The condition was first reported in
1974 in Lancet as a non-neoplastic abnormal immune reaction1. It was
first recognized as a distinct clinical entity in in 1994 in the Revised
European American Lymphoma Classification2. The disease shows a
geological preference to Europe (28.7%) over Asia (17.9%) and North America
(16%). AITL occurs primarily in middle aged and elderly individuals and shows a
slight predominance of males over females.
The disease has a strong association with EBV infection, but
the neoplastic T-cells are almost always EBV negative, creating an interesting
question of EBV’s function in the etiology of AITL. AITL most often presents
late in the disease course with diffuse systemic involvement, including
hepatosplenomegaly, lymphadenopathy and other symptoms such as rash with
pruritis and arthritis. Lab findings include cold agglutinins, rheumatoid
factor and anti-smooth muscle antibodies. There also tends to be
immunodeficiency secondary to the neoplastic process. The clinical course of
AITL is variable, but the prognosis is poor, with the average survival time
after diagnosis being < 3 years. The histological features and genetic
findings have not been found to impact clinical course.
Microscopically, AITL presents with either partial or total
effacement of the normal lymph node architecture with perinodal infiltration.
The cells of AITL are small to medium-sized lymphocytes with clear to pale
cytoplasm, distinct cell membranes and very minimal cytological atypia. These
cells often congregate around the high endothelial venules. The T-lymphocytes
are present in a largely polymorphous inflammatory background of other
lymphocytes, histiocytes, plasma cells and eosinophils. There are 3 overlapping
sub-patterns of AITL. The first of these is similar to a reactive follicular
hyperplasia, and can only be distinguished from normal hyperplasia by use of
immunohistochemical stains to differentiate the neoplastic cells from normal
reactive cells. The second pattern has retained follicles, but they show
regressive changes. The third pattern has completely or sub totally effaced.
These three patterns seem to be on a spectrum with one another, given that
progression from the first to the third pattern has been seen on consecutive
biopsies in the same patient.
Cytologically, AITL cells express pan-T-cell markers
including CD2, CD3 and CD5 and the vast majority are CD4 positive. CD3 may be
quantitatively decreased or absent by flow cytometry. There are a variable
number of CD8 positive T-cells. The tumor cells also show the immunophenotyping
of normal T follicular helper cells including CD10, CXCL13, ICOS, BCL6 and PD1
in 60-100% of cases. CXCL13 and CD10 are the most specific, whereas PD1 and
ICOS are the most sensitive.
References
Horne, C., Fraser, R., & Petrie, J. (1974).
Angio-Immunoblastic Lymphadenopathy With Dysproteinemia. The
Lancet, 304(7875), 291. doi:10.1016/s0140-6736(74)91455-x
Harris, N.l. “A Revised European-American
Classification of Lymphoid Neoplasms: a Proposal from the International
Lymphoma Study Group.” Current Diagnostic Pathology, vol. 2, no. 1, 1994,
pp. 58–59., doi:10.1016/s0968-6053(00)80051-4.
Swerdlow, Steven H. WHO Classification of
Tumours of Haematopoietic and Lymphoid Tissues. International Agency for
Research on Cancer, 2017.
-Zachary Fattal is a 4th year medical student at the Central Michigan University College of Medicine. He is pursuing a career in pathology and has a special interest in hematopathology, cytopathology and blood bank/transfusion medicine. You can follow him on Twitter @Paraparacelsus.
–Kamran M. Mirza, MD, PhD, MLS(ASCP)CM is an Assistant Professor
of Pathology and Medical Education at Loyola University Health System. A
past top 5 honoree in ASCP’s Forty Under 40, Dr. Mirza was named to
The Pathologist’s Power List of 2018. Follow him on twitter @kmirza.