A 4 year old child was brought to the pediatrician by her mother with a complaint of new onset of severe bruising on her legs. The mother could not recall any falls or bumps that would have caused the bruising. On exam, the physician also noted mucosal bleeding in the oral cavity. Questioning revealed that the patient had experienced flu like symptoms several weeks earlier. The physical exam was normal except for the bleeding. There was no family history of bleeding disorders. A CBC was ordered.
Reported CBC Results
WBC, RBC, Hgb, Hct, RBC indicies normal
Platelet count 26 x 103/μL
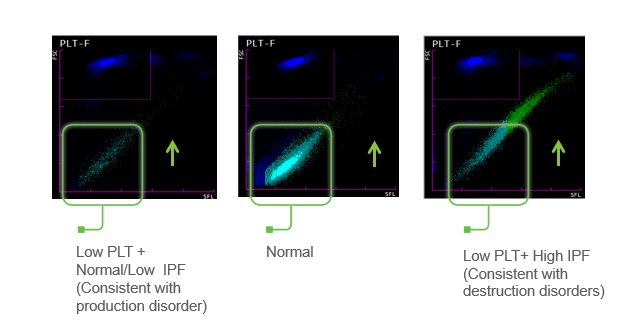
IPF 22% (reference range IPF% 1.0-7.0%) The physician evaluated the results, noting the normal CBC but decreased platelet count. The above results also show the immature platelet fraction (IPF), an additional Advanced Clinical Parameter reported from the Sysmex XN hematology analyzer. A low platelet count, as seen in this patient, will reflex a fluorescent platelet count (PLT-F). The impedance count (PLT-I) can be falsely increased if small RBCs or fragments are counted as platelets. On the other hand, in an optical platelet count, when measuring platelets by size (PLT-O), large platelets can be missed, giving a falsely low count. In this case there was a low platelet count and an instrument flag for an abnormal platelet scattergram. The PLT-F, on the other hand, uses a platelet specific dye which eliminates interference seen with other methods. The fluorescent dye labels the RNA, and forward scatter is used to determine size while side fluorescence is used to measure RNA content. With gating set based on cell volume and RNA content, the PLT-F can be measured. Therefore, the reflexed and more reliable PLT-F was the reported count.
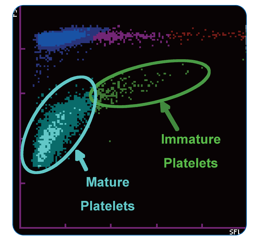
Additionally, when there is an abnormal scattergram or a low platelet count, the IPF% and IPF# are also reported. The immature platelet fraction is a measure of the youngest platelets, or reticulated platelets. These are the first circulating platelets, right out of the bone marrow. An increased IPF indicates an increase in platelet production, yet this child’s platelet count was very low. This suggests that the thrombocytopenia may be due to excessive destruction of platelets; the bone marrow was actively making platelets, but they were being destroyed, causing the low platelet count.
Diagnosis
Immune Thrombocytopenia- ITP.
Primary immune thrombocytopenia (ITP), formerly known as idiopathic thrombocytopenic purpura or immune thrombocytopenic purpura, is one of the most common bleeding disorders of children. In most cases, it presents with sudden onset of bruising and petechiae in an otherwise healthy child, with normal WBC and hemoglobin. ITP is an autoimmune bleeding disorder in which the immune system makes anti-platelet antibodies which bind to platelets and cause destruction. Even though the exact cause of ITP remains unknown, it is recognized that it can follow a viral infection or live vaccinations. While there are some similarities between pediatric ITP and ITP in adults, in children this tends to be an acute disease which is self-limiting and resolves itself in several weeks, with no treatment. However, in a small number of children, the disorder may progress to a chronic ITP. In contrast to ITP in children, a chronic form is more commonly seen in adults. It is usually a diagnosis of exclusion, does not follow a viral illness and requires treatment.
This patient recovered in a few weeks. One month after the initial episode, her PLT was 174 x 103/μL and her IPF% was 6.0%
Conclusion
An IPF reported with a CBC, in combination with a low platelet count, is fast, inexpensive, and can be extremely beneficial in aiding in a timely diagnosis. As the child’s platelet count recovered, the IPF% returned to normal range. ITP can therefore be monitored with a CBC. Thus, the IPF can be used not only to help diagnose but also as an indicator of remission.
References
- Sysmex America, 2019. www.sysmex.com/us. Used with permission
- Arshi Naz et al. Importance of Immature platelet Fraction as a predictor of immune thrombocytopenic purpura. Pak J Med Sci 2016 Vol 32 No 3:575-579
- Briggs,C. Assessment of an immature plateletfraction (IPF) in peripheral thrombocytopenia. Br J Haematol 2004Jul;126(1):93-9
- Sysmex White Paper. The role of the ImmaturePlatelet Fraction(IPF) in the differential diagnosis of thrombocytopenia. www.sysmex.com/us
- D-Orazio, JA, Neely, J, Farhoudi,N. ITP in children: pathophysiology and current treatment approaches.J Pediatr Hematol Oncol.2013 Jan;35(1): 1-13

-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
