A 64 year old female with metastatic left breast cancer,
status-post chemotherapy, presented for erythema, discomfort, and oozing from
her port site for approximately one month. At presentation she was afebrile.
Her port site exhibited erythema and fluctuance. Her most recent absolute
neutrophil count was 1910/cmm. Her port was removed, and a tissue specimen was
sent for microbiologic examination.
Laboratory
Identification
Gram stain showed neutrophils without bacteria. Aerobic
cultures grew a beaded gram positive rod on blood agar at 36 hours. Kinyoun
stain was positive for acid fast bacilli. Matrix assisted laser desorption
ionization-time of flight mass spectrometry (MALDI-TOF) at that time identified
Mycobacterium fortuitum group.
Image 1. Growth on 7H10 agar. Image 2. Kinyoun stain showing acid fast bacilli.
Discussion
M. fortuitum is a
group of rapid growing mycobacteria. Within the group is M. conceptionense, M. houstonense, and M. senegalense. The group
comprises the second most-commonly isolated rapidly growing mycobacterial
respiratory isolates in patients (after M.
abscessus), generally those with underlying lung disease. Progressive
pulmonary disease is generally not seen.
It has also been associated with skin and soft tissue infections
(SSTIs), surgical wound infections, lymphadenitis, and catheter-related
infections. It is seen in the environment and represents a common contaminant.
Identification is by culture and molecular techniques. It is susceptible to
many antibiotics (typically aminoglycoside, cefoxitin, imipenem, or
levofloxacin). Therapy includes two agents based on susceptibility testing for
6 to 12 months. This is somewhat controversial in pulmonary disease as the
clinical significance is not clear.
This patient is being treated through a peripheral IV. The chest
port site at two weeks showed dehiscence of the wound with drainage.
Susceptibilities are pending.
References
Park S, Suh GY, Chung MP, Kim H, Kwon OJ, Lee
KS, Lee NY, and Koh WJ. Clinical significance of Mycobacterium fortuitum isolated from respiratory specimens. Respiratory Medicine. March
2008;102(3):437-442.
Sethi S, Arora S, Gupta V, Kumar S. Cutaneous Mycobacterium fortuitum Infection:
Successfully Treated with Amikacin and Ofloxacin Combination. Indian J Dermatol.
2014;59(4):383–384.
-Jonathan Wilcock, MD is a 1st
year anatomic and clinical pathology resident at the University of Vermont
Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
Adebowale Adeniran, MD is a surgical pathologist and
cytopathologist currently practicing at Yale University and serves as the
Director of Cytopathology there. He completed his medical school training in
Nigeria and moved to the United States to complete a residency and fellowship.
I am fortunate enough to know him as my future attending, as
I will be joining the cytopathology fellowship program at Yale in 2020. I also
know him through attending last year’s Friends of Africa meeting at USCAP,
where he gave a presentation about the status of pathology services in Africa.
His points were compelling and he spoke with passion and heart about the issue.
He is a true global health advocate and I was delighted to have the chance to
talk with him about the work that he is doing in Africa and learn more about
the USCAP Friends of Africa group. Read on to be inspired by his commitment to
global health and learn how you can also get involved!
Q: How did you recognize the need to contribute to
improving pathology services in Africa?
A: Being from Nigeria and having worked there for a
short time as a House Officer, I knew that there were improvements to be made
in the healthcare delivery system, but I hadn’t thought of improving pathology
services specifically. It wasn’t until I was in my second fellowship at
Memorial Sloan Kettering that I had the opportunity to meet Dr. Brian West. He
told me about the USCAP Friends of Africa group in which he was an active part
and had been since the start. He was involved in education initiatives and
would routinely travel to Africa to give lectures and educational seminars.
I went to the next Friends of Africa meeting at the annual
USCAP meeting and was able to speak to others doing similar work to Dr. West.
This inspired me to also get involved and have been participating in the group
ever since. I learned that pathologists practicing back home in Nigeria, and in
most other countries in Sub Saharan Africa, face challenges in practicing
pathology that we don’t have in the US. It only takes seeing the situation once
to realize the great need there is. There are a range of problems, from
outdated equipment, to supply shortages, to all of the things that we take for
granted like consistent access to electricity and water supply. In general,
governments tend to be apathetic to funding healthcare and especially pathology
services, which results in compromised patient care with very few pathologists
to read cases, long turnaround times, and limited diagnoses. The training
programs are usually working with few or old textbooks and limited exposure to
advanced testing modalities. You see these problems and your heart bleeds; you
feel compelled to get involved and give back.
Q: What is the mission of the USCAP Friends of Africa?
A: The organization has evolved and expanded over the
years to increase their outreach to Sub Saharan Africa with the aim of
improving pathology services there. The main leaders in the group, Drs.
Adekunle Adesina, Patrick Adegboyega, Kunle Adesokan, and Jaiye Ogunniyi-Thomas
have made big strides since the start and pathology has come a long way because
of it. The group is supported by the USCAP Foundation and they work to
distribute free educational materials to pathologists and training programs.
They also work with the East and West African divisions of the IAP in developing
and hosting teaching projects called “Schools of Pathology”, which are special
yearly meetings. They are usually around a weeklong of intensive teaching and
mentoring, and they will be held in different countries in West and East Africa
to equalize the opportunities for people to participate. Pathologists from across
the regions travel to be a part of it.
Q: What ways have you found to contribute to improving
pathology services in Africa?
A: For the last five or six years, I’ve worked most
frequently in Nigeria in my medical school alma mater, where I travel back
yearly to give lectures and teach residents with slide sessions. It’s also a
good opportunity for me to review any difficult cases with the department and
offer an outside consultation. I also send journals and reading materials they
don’t have access to otherwise. I’ve also had opportunity to work with three other
medical schools in the area in similar ways.
Volunteering with USCAP Friends of Africa, I participated in
last year’s School of Pathology
meeting that was held in Lagos, Nigeria. This was the first time that I was
able to teach in that program and it was a very good experience.
Q: In what ways can the pathology community get involved
with global health?
A: One very simple and easy way to contribute is to
give a donation to the USCAP
Foundation Global Partners. Every year since 2015, they sponsor
pathologists from low and middle income countries to travel to the USCAP
meeting through a scholarship, the Global
Partners Travel Award. This supports those who often don’t have easy access
to attending academic conferences and who cannot afford the travel cost and
meeting registration fees to travel to USCAP.
Another is by attending the USCAP Friends of Africa meeting
at the annual USCAP meeting and signing up for the many ways you can volunteer
your time and expertise. Anyone who has the desire and ability to go and teach,
organize slide sessions, or collaborate on research projects, has the
opportunity to do so through this organization. These things go a long way and
are really appreciated.
Donations of textbooks, supplies, and equipment such as
cryostats are also needed. Developing the laboratory services in these
countries is really needed and I would encourage those who can to set up
private pathology laboratories to help meet the need.
Academic institutions in the US can offer ways of enhancing training opportunities for African pathologists and trainees by offering short- or long-term exchange programs. This helps to bridge the gap between practiced based learning in resource limited vs. US institutions.
-Dana Razzano, MD is a Chief Resident in her third year in anatomic and clinical pathology at New York Medical College at Westchester Medical Center and will be starting her fellowship in Cytopathology at Yale University in 2020. She was a top 5 honoree in ASCP’s Forty Under 40 2018 and was named to The Pathologist’s Power List of 2018. Follow Dr. Razzano on twitter @Dr_DR_Cells.
Hi everybody! Welcome back. Thanks for following along last
month’s update on Zika epidemiology and clinical lab crossovers. This time
I’ve got a story to tell…
This is my last month of medical school! And, as such, I
decided to go out with a bang and finish up with my last rotation in Emergency
Medicine at The Brooklyn Hospital Center. It was a fantastic month! One would
think that EM and Path are two very distant specialties, but they are more
alike than you might realize. That could be a whole separate article but
consider this: managing critical situations, ensuring fast-paced accurate
response times, engaging in high-stakes algorithms, and making sure mistakes
are caught early. Sounds to me like there’s lots of overlap…remember my
discussion on high
reliability organizations or the critical
role interdisciplinary medicine plays in creating good patient outcomes?
All things aside, all clinicians have a critical role to play, but what happens
when you put an (almost) pathologist in an emergency room?
Basically, you get me having a fun four weeks—I used to be
an EMT and help teach EMS courses, so I do like this stuff. But something else
happened this month that really made this experience special…
Image 1. Typically, med students have minor roles to play in real-life critical codes, but some of our duties include managing monitor attachments for vital signs, securing peripheral IV access, obtaining emergency labs, and other supportive measures while the rest of the code team manages…well, the resuscitation efforts. Source: Life in the Fast Lane.
Saturday, July 27th. I got to sleep in because I
was on the night shift for four days. No big deal. When I finally got to the
hospital, there was pandemonium. Extra ambulances in the loading bay, a couple
squad cars outside, a stab wound victim in the trauma bay, lots of noise and
folks everywhere—what was routine hospital stuff somehow seemed like I was in
the middle of filming an actual episode of ER. (I’m obviously
partial to particular shows…okay, maybe Chicago Med?) When I report to
my team, I learn that the computers have been down. All day. No electronic
health records, no charting, no histories, no internet to look up
guidelines/recommendations on UpToDate—and most tragically: no lab results.
Ok. This is it. I’m on the other (read: clinical) side of an
awful downtime shift. I’ve experienced plenty of downtime in the lab, but this
night I took a deep breath, reminded myself its going to be okay, and did my
best to label things right. But a problem appears that’s more serious than
labeling type and screens the right way without a computer: results are
backlogged for hours! I’m talking no blood gases, no lactic acids, no pregnancy
confirmations! I overheard senior residents and my attending that night talk
about how the lab is struggling and they didn’t have enough people to figure
out this downtime debacle.
This was a moment. It’s not often med students get to be
literally useful in any clinical situation but after high-speed thinking about
it, I interjected and made my elevator pitch:
“Dr. X, Dr. Y – I’ve got several years of hospital lab
experience and lots of background in managing crises and downtime situations,
if you want I’ll head over to the lab and see if I can help this situation at
all, at least for the ER…”
There was a short pause. Then an enthusiastic wave of
approval with hands waving me to go help out our laboratorian colleagues.
Please note: the instances where tidbits of knowledge as a medical laboratory
scientist prove useful as a medical student on rounds are far and few between
for their ability to really captivate a group of doctors who identify
themselves far from any lab medicine; so, this was a win. Explaining the
importance of order of draw, or why sensitivity goes down when you don’t
adequately fill blood cultures, or why peripheral
smears should come with some interdisciplinary caveats aren’t quite as sexy
as an emergency room, on metaphorical fire, with no one but you knowing
anything about how labs work.
So, I ran on over to the laboratory, fully intending to do
what I could to help in my unofficial just-a-friendly-neighborhood-med student
capacity. That’s when I met Jalissa Hall!
I walked into the main lab area and asked if I could talk to
the supervisor, thinking I would just explain my experience and offer what I
could to their staff who I’m sure were buried in downtime SOPs and make sure I
got critical results back to my team in the ER—a win-win! When I asked who was
in charge, a very busy Ms. Hall walked out from behind the chemistry
section and said, “you can talk to me. What’s going on?” I’m sure she thought I
was there to complain, seemingly like many other clinicians were, but I stopped
and gave her the same elevator speech I delivered moments ago with the
postscript: “what can I do for you?” I remember she stopped, thought about if
for roughly 10 seconds, and presented me with her situation briefing:
Computers have been down since roughly 05:00 am
There’s a computer virus that had all servers
shut down indefinitely
There’s no communication between the hospitals
EHR and the labs LIS
Moreover, no patient information is coming
across to the analyzers (MRNs, specimen IDs, etc.)
There are 4-5 critical units (ER, OR, ICU, OB,
NICU) that require STAT results
Clinicians have been coming to the lab all day
looking for informal results reporting
The limited lab staff has had to manually print
results on paper and work to match them with barcodes, specimens, and manual
requisitions before releasing results
Image 2. Jalissa Hall, MLS(ASCP) (left) and a very tired me (right) after a great night of solving lab-related communication problems! Anyone else need an emergency room pathologist? Sounds like a new clinical specialty/fellowship to me…
Deal. I know I can’t jump on the analyzers because New York
is one of
the states that requires clinical laboratory licensure (which I do not
hold). In my informal survey I noted three medical lab scientists (including
Ms. Hall), someone in specimen processing, and someone in blood bank.
Basically, in order to make sure the lab could operate at peak performance with
what they had, I helped alleviate the “paper problem” for them at least for the
ER specimens. I matched requisitions with instrument raw data, made copies for
downtime recording, delivered copied results to the ER, rinsed, lathered, and
repeated—for eight hours! I obviously had to toe the line for the ER results,
but there were other nurses and doctors who came in for the other areas’
results. No one worked more than the folks in that lab that night, and no one
more so than Jalissa. After things cooled down a bit, I got the chance to
connect with her and talk about her career and asked if she had anything to
share with all of you—she definitely did.
Lablogatory family: please meet Jalissa Hall, MLS (ASCP)! (Responses paraphrased because,
honestly it was late, and downtime was busy, and we were tired, ok?)
Jalissa has been working for about five years as a
generalist, with two jobs—like most of us have done. She works at The Brooklyn
Hospital Center as a generalist and at NYU Hospital Lab in their hematology
section. She is a graduate from the excellent MLS program at Stony Brook
University in NY. She’s got ambitious career goals that are aimed at climbing
as high as she can in laboratory medicine, and she’s got the enthusiasm and
work ethic to match! I got the chance to ask her some real questions, during a
real down-time crisis. This is what she had to say:
What made you go into laboratory medicine?
JH: I really want to help people. I love the
behind-the-scenes aspect of being a medical laboratory scientist, but I think
sometimes it can be too behind the scenes…
What did you think of tonight’s downtime issues?
JH: …it could have gone better. There seems to have been
some panic, people kept walking in and shuffling the papers around. I tried my
best to organize by floor, have two copies of each result (one for us and one
to send upstairs), and requisitions match orders, but it was difficult. We have
a downtime protocol, but we just couldn’t keep up with the volume and extent of
how long it’s been down for. There’s really been no help outside the lab to
work with us during this time so it’s a challenge.
What could have happened better?
JH: No outside help meant no room to breathe. On the
inside, supervisors off duty tonight called staff in but none were available to
come in. We don’t have an on-call person. We’re understaffed or short-staffed
like so many labs out there; it’s problematic.
How is this going to look tomorrow?
JH: It’s not looking good, haha! Morning draw is
definitely going to have a hard time. Catching up with these backlogs is one
thing, but if orders can’t come across the LIS we’ll have to address that
problem for sure. We’ve got a great staff though, so I’m sure it’s going to be
fine.
What would be your “top tips” for all our fellow
laboratorians reading this?
JH: First and foremost, being
driven matters. If you want to get ahead, if you want to excel and climb high
within an organization or in our profession, you have to work hard and keep
working toward your goals.
Pro-tip #1: One of the biggest issues is
“vertical cooperation.” Basically, some call it administration-buy-in, but it
means administration working with employees in the lab to make the best
decisions for our patients. If employees are burned out or if there aren’t enough
resources to effectively perform our responsibilities it creates risks! It all
comes down to patients, and making sure we’re in the best position to deliver
diagnostic data for them means considering all aspects of lab management.
Pro-tip#2: If we want to fix the
workforce shortages our labs regularly experience, we have to increase our
efforts in advocacy within our profession. Having programs increase awareness
of this job as a profession increases the pull and interest of potential new
partners to work with. My school did it, other schools do this; increasing the
number of programs that expose students to career opportunities in lab medicine
would address our short-staffing problems everywhere!
Pro-tip #3: TELL OTHERS ABOUT OUR
PROFESSION! I talked about our role being too behind the scenes…well the way to
fix that is professional PRIDE! Own our accomplishments, share our role,
advocate for our recognition, celebrate our peers!
Pro-tip #4: The future is not scary. Lots
of folks shy away from tech advancement, fearing that automation and other
developments mean losing jobs—it doesn’t. Why can’t today’s lab scientists
become tomorrows experts on automation, LIS software, and other aspects of our
cutting-edge field?
It was a pleasure to meet Jalissa
and even better to work alongside her and learn about her passions and goals
within the field we both care about! It was particularly special for me to be
able to use my knowledge and experience to really contribute to my clinical
team and bring laboratory medicine to the forefront where it doesn’t often
shine!
Image 3. In a fantastic book I read recently, the authors of You’re It: Crisis, Change, and How to Lead When it Matters Most talk about leadership as a moment—a moment where you step up to a situation because you have skills and experiences which make you uniquely qualified to serve in a role which aims at a positive outcome. I had a small version of that in front of my attending (important for evaluations in medical school of course), but that downtime night was Jalissa’s “you’re it” moment for sure! (Source: Google)
Signing off from any new clinical
rotations because this guy’s done with his medical school clerkships! Now I’ve
gotta knock out some board exams and go on some residency interviews…wish me
luck! I’ll check in with you next month after the 2019 ASCP Annual Meeting in
Phoenix, Arizona—hope to see some of you there!
See you all next time and thanks
for reading!
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola
University Chicago with a BS in Molecular Biology and Bioethics and then
Rush University with an MS in Medical Laboratory Science. He is
currently a medical student actively involved in public health and
laboratory medicine, conducting clinicals at Bronx-Care Hospital Center
in New York City.
An 18 year old male presented to the
emergency department (ED) with fever, chills, and generalized lower abdominal
pain. He noted the fever began 6 days ago and had been intermittent since that
time. He also reported nausea and vomiting with a decrease in appetite. The
patient was from India and was treated for malaria 8 months ago, directly prior
to arrival in the United States. He stated he received three days of intravenous
medications with resolution of symptoms. In the ED, his vitals were blood
pressure 129/75, heart rate 133, temperature 104.1°F, respirations 20, and 99%
oxygen saturation on room air. On physical exam, patient had mild jaundice and
scleral icterus and severe right lower quadrant pain on palpation. CT scan of
the abdomen showed mesenteric adenitis, but no appendicitis. Initial laboratory
testing showed a mild anemia and thrombocytopenia (hemoglobin 12.1 g/dL,
hematocrit 35.9%, platelets 78,000 TH/cm2) and increased indirect
bilirubin (2.67 mg/dL). The patient received piperacillin-tazobactam while
blood and urine cultures as well as a malaria smear were pending.
Laboratory
Identification
The BinaxNOW lateral flow
immunochromatographic assay for Plasmodium
spp. was performed.
Image 1. The BinaxNOW assay was positive for malaria protein antigen, representing P. vivax, P. ovale, P. malariae, or a mix of these species.
Image 2. A thin smear showed amoeboid gametocytes in enlarged red blood cells as compared to uninfected cells (Giemsa stain, 100x oil immersion). Image 3. A thin smear showed very rare trophozoites with thick chromatin bands and single, large chromatin dots (Giemsa stain, 100x oil immersion).
The positive BinaxNOW results and
morphologic findings on smear review were most consistent with a P. vivax infection. The level of
parasitemia was approximately 0.2%. Blood and urine cultures were negative.
Discussion
Malaria classically presents with fever
and chills, weakness, headache, myalgias, nausea, and vomiting in patients who
live in tropical and subtropical regions. The four most common species that
infect humans through transmission by the female Anopheles mosquito include P.
falciparum, P. vivax, P. ovale, and P. malariae. If malaria is not diagnosed and treated in a timely
manner, complications including anemia, thrombocytopenia, renal failure, acute
respiratory distress syndrome (ARDS), and cerebral malaria can result. P. falciparum is the most deadly species
due to the parasite’s ability to cause high levels of parasitemia.
In laboratories in the United States, malaria
testing often times incorporates Plasmodium
spp. antigen detection via the BinaxNOW assay and peripheral blood smears. While
the performance of the BinaxNOW is acceptable, particularly for P. falciparum, thick and thin peripheral
blood smears remain the gold standard for malaria diagnosis, especially when
the parasitemia level is low. The thick blood smear allows for screening a
large amount of blood for malarial parasites and the thin smear allows for
species identification and assessment of parasitemia. Ideally, multiple blood
smears obtained from different times of the day should be collected in order to
exclude the diagnosis. The window prior to a febrile spike is the best time to
obtain the specimen, as the number of circulating parasites is greatest.
Clinically, the most important
distinction is between P. falciparum
and all other species. A number of features including the morphology of the
trophozoites, schizonts, and gametocytes, size of the infected red cells, the
presence of multiply infected red blood cells, and the region that the patient
lives in or traveled to are helpful in determining species level
identification.
P.
vivax infects enlarged, young red
blood cells and multiple trophozoites may be present in one red blood cell. The
trophozoites have thick, blue cytoplasm and usually one, large chromatin dot.
The schizont can contain 12 to 24 merozoites and the gametocyte is large and
oval in shape. Schuffner’s stippling and malarial pigment are common. It is important
to correctly identify P. vivax and P. ovale as they have hypnozoite forms
in the liver and patients can relapse unless they are treated with an
additional medication to eradicate these forms.
In the case of our patient, he received
chloroquine, the treatment of choice for P.
vivax arising in India. Primaquine and tafenoquine are both options for
eradication of the hypnozoite form in the liver. These medications can cause
hemolytic anemia in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency
so quantification of the enzyme is required prior to administering therapy. Our
patient had normal G6PD levels and received tafenoquine as well.
-Karla
Perrizo, MD, is a clinical pathology resident at the University of Mississippi
Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the
University of Mississippi Medical Center in Jackson, MS. She is
certified by the American Board of Pathology in Anatomic and Clinical
Pathology as well as Medical Microbiology. She is the Director of
Clinical Pathology as well as the Microbiology and Serology
Laboratories. Her interests include infectious disease histology,
process and quality improvement, and resident education.
Last
month we reviewed the different federal regulatory agencies responsible for
establishing laboratory testing guidelines, and a brief overview of the
different roles each department has. This month we’ll attempt to demystify
testing complexity (waived, non-waived, PPM) and why testing classification
matters. Still to come, we’ll review the optional accreditations available to
labs, and how accreditation differs from certification.
For all
in vitro diagnostic tests, the FDA is responsible for categorizing each test
based on their perceived complexity during the pre-market approval process.
From least to most complex, the categorizations are waived, moderate
complexity, and high complexity. The reason this is important is because with
each jump in test category, the CLIA rules associated with performing testing
will change – as will the permit designation required to perform testing. This
includes things such as QC requirements, validation testing, and personnel
requirements to define who can perform testing in the first place.
Waived tests are considered easy to use,
with little to no chance that the test result will provide wrong information or
cause harm if it is done incorrectly. This includes over-the-counter tests such
as home use urine pregnancy kits, where if the sample is applied incorrectly or
in insufficient volume there will simply be no result obtained at all. Many
Point of Care tests fall under this category, with testing performed in a wide
variety of locations including physician offices, urgent care clinics, imaging
centers and nursing homes. Locations performing waived testing only are still
required to obtain an appropriate CLIA Certificate of Waiver. (See the reference links at the end for a
list of all FDA approved CLIA-Waived tests.)
For
waived testing, laboratories must follow the manufacturer’s instructions for
testing, including the stated FDA approved intended use, without any deviation.
If the procedure is modified, or the test is used with specimens not approved
by the FDA – the complexity classification of the test will change from waived
to high complexity. A common situation where this occurs is with fingerstick
whole blood glucometers. Most device manufacturers on the market today for
point of care glucose testing are not FDA approved for use with
critically ill patients. Using these waived meters for patients deemed
“critically ill” based on your local institution’s designation would change the
complexity of testing from waived, to high, for this population of patients as
it would be considered “off-label use” – meaning you are using it against FDA
recommendations and approved forms of use for the test/instrument.
Another
caveat to be mindful of is your local state regulations. Certain states (NY,
especially) have very strict rules regarding testing complexity designation. In
NY, all tests performed within the same designated laboratory space will have
the same testing complexity designation. Meaning that if you have a moderate
complexity CBC analyzer in the same room you perform your waived urine
pregnancy tests – both are now considered moderate complexity. Even though
you’re following the manufacturer’s instructions for the pregnancy kit, using
only approved specimen types, and the kit is on the FDA approved CLIA-Waived list
– that test is now moderate complexity just because it is in the same room as
other higher complexity tests. That same pregnancy kit is considered waived
when kept separate in the emergency department, but becomes moderate complexity
(or higher) when used in the central laboratory.
Nonwaived tests refer to both moderate and
high complexity testing. After the FDA has approved a marketing submission,
their CLIA categorization of the test follows by utilizing a scorecard to grade
the test complexity on 7 different criteria. All phases of testing
(preanalytic, analytic and postanalytic) are evaluated in these steps:
Knowledge
– low scores require minimal scientific and technical knowledge to perform the
test, and knowledge needed can be easily obtained through on-the-job
instruction.
Training
& Experience – low scores require minimal training and limited experience
to perform the test.
Reagents
& Materials Preparation – low scores have stable and reliable reagents, and
require no special handling, precautions, or storage conditions. They typically
come prepackaged, premeasured, and ready for use; whereas high scores may
include manual steps such as volumetric measurements and/or reconstitution.
Characteristics
of Operational Steps – low scores have automatically executed steps (such as
dispensing specific volumes of sample/reagent, temperature monitoring, or
timing of steps); high scores require close monitoring or control, precise
temperatures or timing, accurate pipetting or extensive calculations.
Calibration,
Quality Control, and Proficiency Testing Materials – low scores have all
required reagents, controls and PT material commercially available and products
are stable.
Test
System Troubleshooting & Equipment Maintenance – low scores have automatic
troubleshooting or self-correction of errors (failed internal QC will
automatically repeat), or requires minimal judgement. Equipment maintenance
will be performed by the manufacturer or is minimal and easily performed,
whereas high scores require decision-making and direct intervention to resolve
most issues, or maintenance tasks require special skills and abilities.
Interpretation
& Judgement – low scores require minimal interpretation and judgement for
resolution of problems or determination of test results.
Low
scores indicate low complexity, with tests obtaining a total score of ≤12 being
categorized as moderate complexity. Tests with final scores >12 are
categorized as high complexity.
PPM: Within the category of nonwaived
tests is a subcategory referred to as Provider Performed Microscopy (PPM).
These are tests that are performed directly by a clinician during a patient
visit, and require the use of a microscope limited to bright-field or
phase-contrast microscopy. Based on the nature of the sample obtained, testing
must be performed immediately at the time of collection as delays could
compromise the accuracy of test results. As controls are typically not
commercially available for these tests, the testing is restricted to clinicians
only as knowledge and judgment is required to confirm testing accuracy and
correlation to the clinical presentation.
Tests
allowed under a PPM certificate are mostly related to OB/GYN procedures, with a
full list available through CMS here:
So the
next time you receive a request to add a new test at your laboratory, you’ll be
armed with a fairly long list of the requirements that come with that test
based on its complexity. Coming up next month we’ll discuss the difference
between laboratory certification and accreditation, along with the benefits of
obtaining accreditation for your lab.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s
2018 Top 5 in the 40 Under Forty recognition program. She has worked in
the medical laboratory profession for over 18 years. In her current
position, she transitions between performing laboratory audits across
the entire Northwell Health System on Long Island, NY, consulting for
at-risk laboratories outside of Northwell Health, bringing laboratories
up to regulatory standards, and acting as supervisor and mentor in labs
with management gaps.
In my July post, “Blood Bank Case Study:
What’s Your Type?” I discussed some of the dilemmas when dealing with a weak D
phenotype and the fact that there is no standard or general consensus as to the testing
performed or terminology to be used in resulting a weak D patient. Results
obtained on patient testing also vary depending on the method used, and the
anti-D reagent and enhancement used in testing. This can be confusing to medical
technologists, physicians and to patients.
For anyone who has not been in the Blood bank for a while, the Du variant was first
recognized in 1946 and renamed weak D in 1992. To
review last month’s blog, serologic studies have distinguished three broad
categories of D variants, weak D, partial D, and DEL, from conventional D. A
serologic weak D phenotype is one that has no or weak reactivity (≤2+) of RBCs
with an anti‐D reagent at immediate spin, but does agglutinate with antihuman
globulin. Since there is no general consensus on how labs perform
and report patient testing for weak D, it is left up to individual
interpretation as to what type blood these patients should receive, and, if
pregnant, if they should receive Rh D immune globulin (Rhogam). Last month I
focused on testing, resulting, donors and blood administration. In this blog I
will focus on issues concerning weak D in the obstetric population and how labs
can move forward now and in the future towards the best patient care and blood
management.
About 15% of
Caucasians are RhD negative. About 3% are weak D phenotypes.In the genral
population, this means that about 0.2% to
1.0% inherit RHD genes that code for serologic weak
D phenotypes.2 In Europe
and the US, weak D phenotypes are the most common D variants found, but we also know that the
prevalence of weak D phenotypes varies by race and ethnicity. Today we have
much more information about D antigen expression than we had in the past, because
we have the availability to genotype these weak D RBCs. We know that more than
84 weak D types have been identified, but types 1, 2, and 3 account for more
than 90% of these in people of European ethnicity.1 Currently,
with the mixed ethnicity population in the US, about 80% of people who inherit RHD genes for serologic weak D
phenotypes are found to be weak D
type 1, 2, or 3.3 We also know that
types 1, 2 and 3 are unlikely
to become alloimmunized to anti-D, so they can safely be treated as RhD
positive and receive RhD positive units.
The introduction of RhD immune globulin in 1968is one of the great success
stories in obstetrics. Rhogam has been used very successfully in developed
countries in the prevention and treatment of hemolytic disease of the fetus and
newborn due to RhD alloimmunization. The routine recommendation is that women
who are candidates for Rhogam receive one dose at approximately 28 weeks’
gestation and a second dose after the delivery of an Rh pos baby. Additional recommendations are for administration
of Rhogam after threatened miscarriage, abdominal trauma during pregnancy and
before invasive diagnostic procedures.
But,
who is a candidate? Any unsensitized woman who is RhD negative and who may be
carrying or who delivers an RhD positive baby is a candidate for Rhogam. And,
that brings us back to the problem that we have no standardization for the
reporting of serological weak D phenotypes.
As
an example, let’s look at a patient who has 3 children. Many labs do not do
weak D testing on patients and report anyone who is RhD negative at immediate
spin as RhD negative. This patient was typed at such a lab (Lab #1) as RhD
negative, and received Rhogam for her first pregnancy. During her 2nd
pregnancy, she had moved to a different state, and went to another lab (Lab #2)
for prenatal testing. This lab performed serologic weak D testing and found
this patient to be weak D positive and reported her type as RhD positive.
Rhogam was not further discussed during this pregnancy and the patient did not
receive Rhogam. The patient had blood drawn during her 3rd pregnancy
at yet a third hospital (Lab #3). Some labs distinguish women who are pregnant
or of childbearing age from the general population, and have different procedures
on the reporting of RhD type on these women. This hospital’s procedure was to
do weak D testing on all patients, but, in women of childbearing age, if weak D
positive, they report these women as RhD negative. The patient was told she was
RhD negative and would be a candidate for Rhogam. At this time the woman
thought she remembered that she didn’t get Rhogam with her second pregnancy and
was a little confused, but with 2 young children and pregnant with her 3rd,
she simply followed the doctor’s recommendation and didn’t question further.
When her 3rd child was 4 months old, she attended a Red Cross blood
drive at work and donated a unit of blood. Soon she received a blood donor card
in the mail that said she was RhD positive. At this point she was thoroughly
confused and questioned all the lab results she had had done over the past 6
years. On her next visit to the doctor she questioned her obstetrician. The
obstetrician recommended RhD genotyping. The woman was found to be weak D type
2. The doctor explained to her that all blood donors who are weak D are treated
as RhD positive, but, that as a patient, policies and procedures vary. However,
he also informed her that now that they had her genotype, she would be
considered RhD positive. He explained that the genotype was DNA testing, would
not need to be repeated, she would not need Rhogam for any future pregnancies
and she could safely receive RhD positive blood products.
The
American College of Obstetricians and Gynecologists (ACOG) guidance practice
bulletin of 1981 recommended that recommended that RhD‐negative women “whether Du positive or
Du negative” were candidates for Rhogam. Shortly
afterwards, that recommendation was
reversed and revised to read “[a]
woman who is genetically Du‐positive is Rh‐positive and
administration of Rh immune globulin is unnecessary.1 This remained the recommendation of the
group until the latest version of this publication in 2017. The 2017 ACOG
guidelines recommend giving Rhogam to weak D positive patients, “in appropriate
clinical situations, until further studies are available.”3 Another comparative
study published in 2018 reported inconsistency between national groups over how
to treat weak D phenotypes and recommended the creation of international
guidelines.4
Thus,
the controversy over whether a pregnant woman who is weak D positive is RHD
positive or RHD negative continues. The latest recommendations, and those of
ACOG, are for a move to genotyping patients with a serological weak D
phenotype. There are several benefits to this. As we can see from my case study
example, genotyping put this woman at ease and gave her definitive answers
about her blood type. It also can do the same thing for medical technologists
and physicians. RHD genotyping only needs to be performed once on a
patient. If performed at the first prenatal appointment, this would alleviate
much confusion as to procedures and how to report the results. I have in blood
bank, that whenever we have a weak D on a prenatal patient, there are questions
about how to result them, and we refer to the SOPs. We also occasionally get a
patient who had previously been typed elsewhere where the reporting procedures
were different and there is therefore an apparent discrepancy between the
current and historical typing. This causes frequent phone calls from physicians
and nurses asking for clarifications on weak D types, and questions about
Rhogam. Lastly, RHD genotyping could avoid confusion which could lead to
transcription and computer entry errors when entering types on these patients. RHD
genotyping would solve all of these problems and eliminate confusion.
Additional
benefits of RHD genotyping are, if RHD genotyping was performed
on all weak D transfusion recipients, we could save as many as 47,700 units of
RHD negative RBCs annually.3 With the availabilityof
molecular testing, there is no reason to administer RhD negative units to
patients who can use RhD positive units. This could help alleviate the constant
shortage of RHD negative units. With RHD molecular testing, these
critical units could be reserved for patients who are truly RhD negative.
It may not be feasible for all laboratories to perform molecular testing for RHD genotypes, but reference laboratories should offer affordable testing for the most prevalent and clinically relevant RHD genotypes. From a study done of over 3100 laboratories, it was found that, at this time in the US, most labs are managing weak D phenotypes as RhD negative. Laboratories not performing weak D testing are essentially avoiding their detection. Clinical laboratories should instead increase the detection of serological weak D and interpret these with the use of RHD genotyping. Rhogam shortages exists, and RHD genotyping could save thousands of injections of Rhogam annually in the US alone, and at the same time, avoid the unnecessary administration of products to patients. The work group study calculated that annually, approximately 24,700 doses of unnecessary Rhogam could be avoided.1 It is time to move forwards to molecular testing for the best patient care and blood management.
References
Sandler SG, Flegel, WA, Westhoff CM, et al. It’s time to phase in RHD genotyping for patients with a serologic weak D phenotype. Transfusion 2015;55:680‐9
Garratty G. Do we need to be more concerned about weak D antigens? Transfusion 2005;45:1547‐1551.
Practice Bulletin No. 181: Prevention of Rh D AlloimmunizationObstetrics & Gynecology: August 2017 – Volume 130 – Issue 2 – p e57-e70 doi: 10.1097/AOG.0000000000002232
Sperling, JD et al. Prevention of RhD Alloimmunization: A Comparison of Four National Guidelines. Am J Perinatol. 35(2):110-119. doi: 10.1055/s-0037-1606609. Epub 2017 Sep 14.
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated
from Merrimack College in N. Andover, Massachusetts with a BS in
Medical Technology and completed her MS in Clinical Laboratory Sciences
at the University of Massachusetts, Lowell. She has worked as a Medical
Technologist for over 30 years. She’s worked in all areas of the
clinical laboratory, but has a special interest in Hematology and Blood
Banking. When she’s not busy being a mad scientist, she can be found
outside riding her bicycle.
A 57 year old male with a recent history of a left above the
knee amputation developed a fever during the same admission of 101.1°F. His
amputation had been complicated by poor wound healing, and he had a
simultaneous right leg abscess that grew methicillin-sensitive Staphylococcus aureus. Examination of
his wound showed serosanguinous drainage with no erythema or purulence. Blood
cultures and a wound swab were sent for microbiological analysis.
Laboratory Findings
Wound cultures grew methicillin-resistant Staphyloccocus aureus thought to
represent colonization rather than true infection. Blood cultures flagged
positive in one anaerobic bottle only at 30 hours. A gram smear showed
gram-negative cocci (Image 1). Anaerobic blood plates grew pinpoint colonies
(Image 2). MALDI-TOF identified the bacteria as a Veillonella species.
Image 1. Gram stain from anaerobic culture showing gram negative cocci.Image 2. Growth on anaerobic blood plate.
Discussion
Veillonella species
are gram negative cocci. They are lactate fermenting, obligate anaerobes and
are considered normal flora of the intestines and oral mucosa. As such, they
are usually regarded as a contaminant. They have, however, been implicated in
osteomyelitis, prosthesis infections, and endocarditis. They are particularly
associated with poor oral hygiene, chronic periodontitis, and smoking. They have
important implications in dental disease due to their ability to form biofilms.
They are frequently resistant to ampicillin and have also been noted to be
resistant to tetracyclines in periodontal patients. Identification is done by
molecular methods, typically MALDI-TOF. PCR has also been developed, but is not
routinely used.
This was considered a contamination due the absence of
symptoms and isolation in one bottle only. A follow up blood culture was
negative. Routine wound care was resumed.
References
Rovery C, Etienne A, Foucault C, Berger P, Brouqui P.
Veillonella montpellierensis endocarditis. Emerg Infect Dis.
2005;11(7):1112–1114.
Mashima I, Theodorea CF, Thaweboon B, Thaweboon
S, Nakazawa F. Identification of Veillonella Species in the Tongue Biofilm by
Using a Novel One-Step Polymerase Chain Reaction Method. PLoS One. 2016;11(6):e0157516. Published 2016 Jun 21.
-Jonathan Wilcock, MD is a 1st
year anatomic and clinical pathology resident at the University of Vermont
Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
The patient is a 6 year old who developed abdominal pain 2
days prior to admission. The patient was in school when the abdominal pain
began, resulting in the patient doubling over in pain. The pain resolved within
1 hour, however, because the initial presentation was an unremitting abdominal
pain, the patient was taken to an outside hospital for evaluation. There was no
vomiting, diarrhea, or constipation. On
physical exam, the patient was very tender to palpation in the right lower quadrant and was unable to tolerate
deep palpation. A computed tomography scan was subsequently ordered which
showed a large mass in the pelvic peritoneum. The patient was admitted to
surgery for an exploratory laparotomy, with resection of the pelvic mass.
Diagnosis
Received fresh in the Surgical Pathology
laboratory is a 162.5 gm, 10.2 x 7.5 x 4.0 cm lobulated, ovoid mass of
pink-tan, rubbery tissue that appears encapsulated by a thin translucent
membrane. The margins are inked black and the specimen is serially sectioned
revealing glistening, gray-tan soft tissue with focal areas of yellow
discoloration and softening. Along one edge of the specimen, there is a 4.0 x
1.5 cm rim of dark red-brown, rubbery tissue (Figure 1). Portions of the fresh
specimen are submitted in glutaraldehyde for electron microscopy if needed,
RPMI for cytogenetics, and are snap-frozen as well. Touch preparations are also
made and gross photographs are taken. Representative sections are submitted as follows:
Cassette 1-7: Sections of mass including inked
capsule
Cassette 8-10: Representative sections from central
portion of mass including areas of softening and discoloration
Cassette 11-13: Additional representative
sections of the mass
Image 1. Cut surface of a gray-tan mass with yellow areas of discoloration and hemorrhage around periphery.
Histologically, the mass is composed of sheets
and nests
of small round cells along thin
fibrous septa, giant multinucleated cells, and rare strap cells. Necrosis less
than 5%. The margins are positive, although the specimen is unoriented. Venous
and lymphatic invasion is absent. Immunohistochemical (IHC) stains are ordered
and the results are listed below:
Positive IHC stains: Myogenin, desmin, CD56
and Bcl-2
Negative IHC stains: S-100, keratin AE1/AE3,
CAM 5.2, SMA, CD99, Fli-1, WT-1, and EMA
In addition to the IHC stains, a portion of
tissue was sent for cytogenetics testing, which showed a chromosomal translocation
at t(2;13)(q35;q14). Based on the histologic appearance, IHC stains, and
cytogenetic testing, the specimen was signed out as an alveolar
rhabdomyosarcoma with a pathologic stageof pT2b, N0, MX.
Following the diagnosis, the patient was
placed on a chemotherapy regimen of Vincristine, Adriamycin, Etoposide and
Cytoxan, as well as radiation therapy.
Discussion
Rhabdomyosarcoma is the most common malignant soft tissue
tumor in children and is the most common malignant solid tumor in children
after neuroblastoma and Wilms tumor, accounting for 5-10% of all childhood
tumors. 90% of these tumors occur in patients under the age of 25, and
approximately 70% occur in children under 10 years of age. The most common
locations of rhabdomyosarcoma are in the head and neck region, followed by the
genitourinary system, extremities and then torso.
The 2013 World Health Organization classification of skeletal
muscle tumors divided rhabdomyosarcoma into four types based on histology:
Embryonal rhabdomyosarcoma (botryoides and
anaplastic variant)
Alveolar rhabdomyosarcoma (solid and anaplastic
variant)
Pleomorphic rhabdomyosarcoma
Spindle cell/sclerosing rhabdomyosarcoma
Alveolar rhabdomyosarcoma (ARMS) accounts for approximately
20-30% of all rhabdomyosarcoma tumors, with no genetic predisposition. Although
it is most common in teenagers, ARMS affects all ages. Most patients will present
with a painless soft tissue mass, but based on the size and location of the
mass, it may cause mass effect. A quarter of patients will have metastasis at
the time of diagnosis, most commonly to the bone marrow, bones, and lymph
nodes.
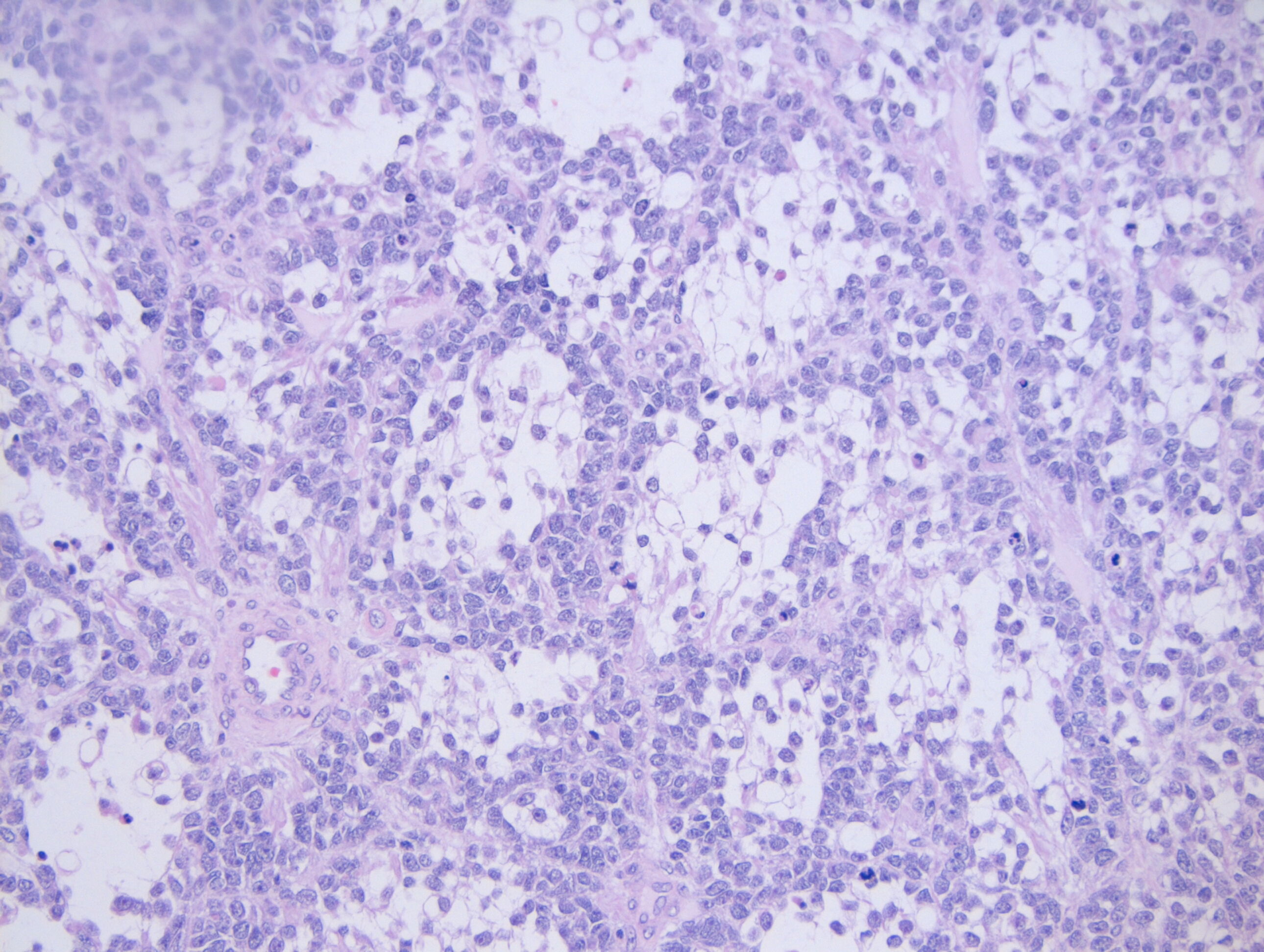
Grossly, ARMS presents as a solid, well-defined mass with a fleshy, tan-gray cut surface. Histologically, it is composed of small, blue, round cells and occasional round to spindle shaped rhabdomyoblasts. When compared to embryonal rhabdomyosarcoma, the rhabdomyoblasts in ARMS are slightly larger. ARMS is broken down into two subtypes: the classic subtype and the solid subtype. In the classic subtype, the tumor is composed of nests of cells that adhere to the edges of fibrous septa, resembling pulmonary alveoli (hence the name alveolar rhabdomyosarcoma). Multinucleated giant cells with a peripherally located nuclei may also be present. In the solid subtype, there will be nests and sheets of neoplastic cells that are separated by thin fibrovascular septa, but will not form in the classic alveolar pattern (Image 2).
Image 2. 20x photomicrograph demonstrating the neoplastic cells lining up along thin fibrous septa, giving the appearance of pulmonary alveoli
Due to the various appearances of rhabdomyosarcoma, it has
become important to integrate immunohistochemical (IHC) stains and molecular
testing into the diagnosis. The most common IHC stains that are used to
determine the rhabdomyoblastic differentiation of a sarcoma is through the use
of Myogenin and Myogenic differentiation 1 (MyoD1) stains, in which both stains
will be positive in rhabdomyosarcoma. These two stains can be furthered used to
help narrow down a diagnosis of ARMS because if more than 50% of the neoplastic
cells express Myogenin, this is highly suggestive of a diagnosis of ARMS
(Figure 3). In ARMS, the MyoD1 will have a variable expression. Additional
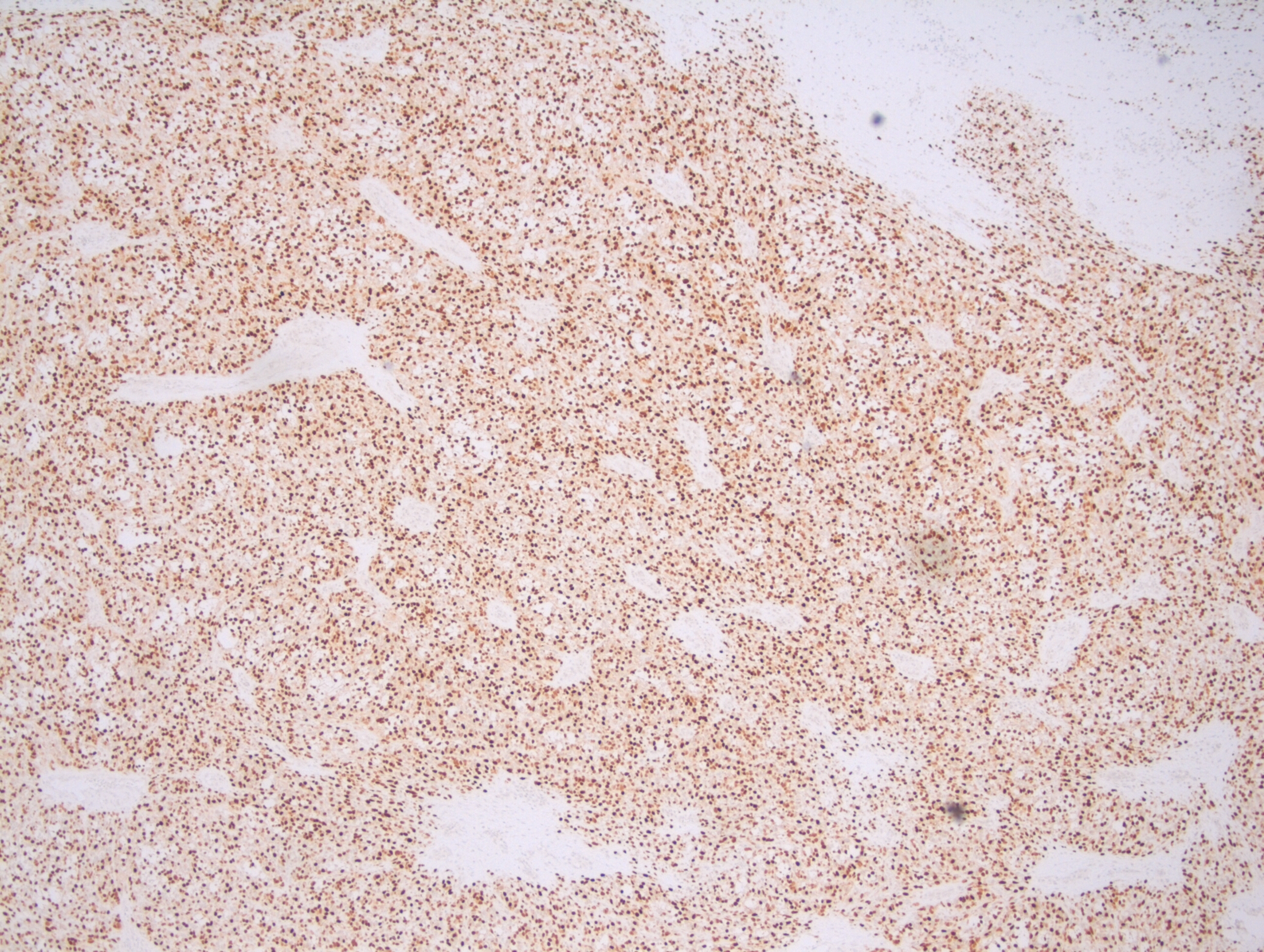
positive IHC stains for ARMS can include: desmin, P-cadherin, and bcl-2.
Image 3. Myogenin IHC stain demonstrating a strong, homogenous expression
To go along with IHC stains, molecular testing has been shown
to be affective with determining the type of rhabdomyosarcoma. There have been
two translocations that have been identified in ARMS. The first is at
t(2;13)(q35;q14), which results in a fusion of the PAX3 gene with the FOXO1
gene (previously known as the FKHR gene). This translocation is present in 60%
of all ARMS cases, and has been found to occur mostly in older children and
younger adults. The second translocation is at t(1;13)(p36;q14), which results
in a fusion of the PAX7 gene with FOXO1, and is present in approximately 20% of
all ARMS cases. The remaining 20% are fusion negative, and are associated with
the solid subtype histologically. There is early preliminary data that shows a
less aggressive disease course in patients with the PAX7-FOXO1 fusion, compared
to those with the PAX3-FOXO1 fusion.
In order to determine the best treatment course, patients who
are diagnosed with rhabdomyosarcoma are divided into a low risk, intermediate
risk or high risk group based on the pathologic stage, clinical stage and
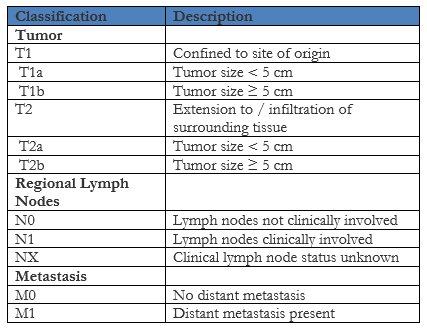
clinical group. The pathologic stage is determined using the Pretreatment TNM
Staging System that was set forth by the Intergroup Rhabdomyosarcoma Study (IRS)
group (not the same as the TNM staging system put out by the American Joint
Committee on Cancer) below:
The clinical stage is then determined using the TNM staging
above and the Pretreatment Clinical Staging System below that is also put out
by the IRS group:
In the above Clinical Staging System, a favorable site is
defined as occurring in the orbit, biliary tract, head and neck region
(excluding parameningeal) and genitourinary region (excluding prostate and
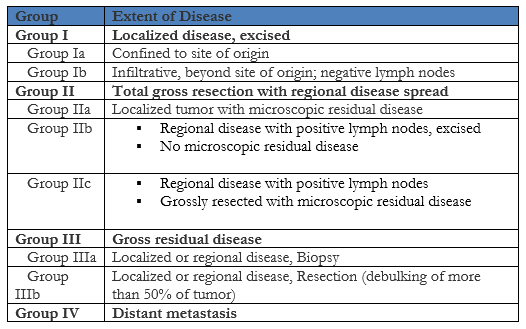
bladder). Any other site not listed is considered unfavorable. Next, a clinical
group is assigned based on the extent of the disease using the Clinical
Grouping System below, which again is put out by the IRS group:
Lastly, based on the clinical stage and clinical group
determined above, the patient is assigned a risk group of either low risk,
intermediate risk, or high risk using the Children’s Oncology Group guidelines
listed below:
When compared to embryonal rhabdomyosarcoma, which is the
most common type of rhabdomyosarcoma, ARMS has a worst prognosis. The IRS group
clinical group and stage can help to predict the overall outcome of the
patient, with the standard treatment regimen composed of surgery, radiation
therapy and chemotherapy.
References
Dziuba I, Kurzawa P, Dopierala M, Larque A,
Januszkiewicz-Lewandowska D. Rhabdomyosarcoma in Children – Current Pathologic
and Molecular Classification. Pol J
Pathol. 2018;69(1):20-32. doi:10.5114/pjp.2018.75333
Liu H, Zhao W, Huang M, Zhou X, Gong Y, Lu Y. Alveolar
rhabdomyosarcoma of nasopharynx and paranasal sinuses with metastasis to breast
in a middle-aged woman: a case report and literature review. Int J Clin
Exp Pathol. 2015;8(11):15316–15321. Published 2015 Nov 1.
Owosho AA B Ch D, Huang SC Md, Chen S Mbbs, et al. A
clinicopathologic study of head and neck rhabdomyosarcomas showing FOXO1
fusion-positive alveolar and MYOD1-mutant sclerosing are associated with
unfavorable outcome. Oral Oncol. 2016;61:89–97.
doi:10.1016/j.oraloncology.2016.08.017
Rudzinski ER, Anderson JR, Hawkins DS, Skapek SX, Parham DM,
Teot LA. The World Health Organization Classification of Skeletal Muscle Tumors
in Pediatric Rhabdomyosarcoma: A Report From the Children’s Oncology
Group. Arch Pathol Lab Med. 2015;139(10):1281–1287.
doi:10.5858/arpa.2014-0475-OA
-Cory Nash is a board certified Pathologists’ Assistant,
specializing in surgical and gross pathology. He currently works as a
Pathologists’ Assistant at the University of Chicago Medical Center. His
job involves the macroscopic examination, dissection and tissue
submission of surgical specimens, ranging from biopsies to multi-organ
resections. Cory has a special interest in head and neck pathology, as
well as bone and soft tissue pathology. Cory can be followed on twitter
at @iplaywithorgans.
For most people working in laboratory
medicine, their first encounter with transgender patients likely arose from an
issue involving the Electronic Health Record (HER). For me, I was called into
the reference lab, because an abnormally high estradiol result was found by the
referring lab. They were concerned this might be coming from a hormone
secreting tumor, but inspection of the patient’s record revealed they had been
taking higher than recommended doses of their feminizing hormones.
Today I will share stories from issues
that arise in EMR when gender doesn’t equal sex. While these may not
specifically happen to all of you, I hope they can be informative or help you
anticipate future problems.
Transgender issues came up at one of our
institutions when providers were getting dozens of messages in their in-baskets
about new flagged lab results for multiple patients. This is very annoying,
because they have to address each of these messages or they are out of
compliance with the hospital. An investigation revealed that all of the
patients involved were transgender patients. In order to get estradiol, sold as
oral contraception pills, the pharmacy had to administratively change their sex
in the EHR for approval, then change it back.
This moved their corresponding reference
ranges out of sync, which triggered a new results flag. Changing the sex back
triggered other flags and more messages. This was finally resolved after a
committee was convened and several meetings occurred, but no one would have
anticipated this type of issue arising from a simple action to get patients
their medicine.
Sometimes transgender patients have their
sex changed legally. If an EHR only includes one sex entry instead of gender
and sex assigned at birth, then certain lab errors may prevent processing of
important samples. The pregnancy test for a transgender man could be
auto-rejected. This can be an issue even for providers in front of the patient
as was recently reported in a case to the NEJM about a transman who was
mistaken as obese instead of pregnant and miscarried their child.
Similarly, a prostate biopsy from a
transgender woman could be auto-rejected by a surgical pathology system as an
inappropriate specimen type for the patient. Even further, an EHR could fail to
prompt a provider from making a prostate cancer risk assessment in a
transgender woman, which could result in improper screening.
I would recommend that EHR includes three
separate fields (sex assigned at birth, gender, and legal sex) to fully
recognize transgender patients and provide optimal personalized healthcare to
them.
References
Gupta S, Imborek KL, Krasowski MD. Challenges in Transgender Healthcare: The Pathology Perspective. Lab Med. 2016 Aug; 47(3):180-188.
Stroumsa D, Roberts EFS, Kinnear H, Harris LH. The Power and Limits of Classification – A 32-YearOld Man with Abdominal Pain. N Engl J Med. 2019 May 16;380(20):1885-1888. doi:10.1056/NEJMp1811491.
-Jeff SoRelle, MD is a Chief Resident of Pathology at the
University of Texas Southwestern Medical Center in Dallas, TX. His
clinical research interests include understanding how the lab intersects
with transgender healthcare and improving genetic variant
interpretation.
There are multiple types of risk assessments required when
managing a laboratory safety program. OSHA’s Bloodborne and Airborne pathogens
standards require assessing the risk of employees’ exposure to particular lab
hazards. Risk assessments can be used to determine whether or not to add an
emergency eyewash station, and all lab chemicals need to be assessed for the
hazards they pose. These are just some assessments that are needed, and there
are particular steps to take when performing them. But what about the lab
emergency management plan? Should the lab perform a risk assessment for that?
The answer is yes, although the terminology used may be different. To prepare a
disaster readiness plan for the lab, the risk assessment that is needed is
known as a Hazard Vulnerability Analysis (HVA).
The Centers for Medicare & Medicaid Services (CMS)
requires that all healthcare facilities use an “all-hazards” approach when
considering emergency preparedness and planning. While some laboratories may be
included with the facility-wide disaster plan, the lab should absolutely have
its own plan with specific instructions that apply directly to the department.
That means the lab should also consider an all-hazards approach.
It may seem daunting to try to consider every possible
disaster that could occur in the department, but that is not exactly what the
directive from CMS dictates. An all-hazards approach means that emergency plans
should be scalable or flexible so that it can be used for many types of
disasters. The plan should focus on the lab’s ability to continue to offer
services, especially those deemed critical, as a disaster situation unfolds.
The first step to the plan creation is the risk assessment-
the Hazard Vulnerability Analysis. The HVA can be a table that lists all of the
potential types of disaster; natural, man-made, facility-specific, etc. List as
many as you can think of, and be sure to include specific disasters that may be
particular to your locale (earthquakes, blizzards, etc.). Rate each disaster
type by probability, severity of impact, and level of readiness of the lab to
respond. Using that data, you can calculate the risk percentage for each
emergency type.
One other requirement imposed by CMS is that facilities must
include emerging infectious diseases as one potential type of hazard class.
With the advent of particular diseases in the past years like Ebola, Zika, and
certain influenza types, it is important to consider how an outbreak would
affect lab operations and staffing. The risk level of infectious diseases may
vary as incidents and outbreaks occur in particular geographic regions or if
pandemics arise.
The HVA should be reviewed and updated as necessary each
year. Things change that can affect what is on your HVA list. The addition of a
nearby airport might make you consider adding airline disaster to the HVA. A
change in weather patterns could occur as well. In 2011 a surprise earthquake
in Virginia made state facilities re-look at their HVA list of possible emergency
situations. Also, the actual list of disasters might not change, but there may
be a change in the potential of a particular incident occurring.
If your lab or facility has not yet performed the HVA risk
assessment, there is no need to panic. There are several model HVA tools
available on line that can be used. As with any risk assessment, be sure to
keep documentation readily available, review it each year, and make sure staff
are trained about not only the HVA process, but in how to use the emergency
management plan as well. There is a great amount of work that can go into
preparing for a disaster, and training and drills for your staff will help to
facilitate a smoother activation of the plan when the real emergency situation
occurs.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years
experience as a certified medical technologist. Today he is the
Laboratory Safety Officer for Sentara Healthcare, a system of seven
hospitals and over 20 laboratories and draw sites in the Tidewater area
of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.