I’ve appreciated some amazing feedback from my previous post discussing how doctors can sometimes be patients too, and the challenges one might face in different roles within our health care system. Not only a challenge of roles, but those that struggle with invisible illness have unique perspectives on patient care.
That said, this month let me take a break from all the fun content found between cases, concepts, and trends in pathology and laboratory medicine, and celebrate our amazingly successful (and virtual) Annual ASCP Meeting!
Image 1. Just look at this virtual lobby! Set aside that in-person connectivity dissapointment and just appreciate the quality put into this visually! More of my oggling to come in further images…
It was awesome. But don’t just take my word for it, we’re all people of science here, right? So let’s do it by the numbers!
133 educational sessions
3 general sessions
4 named lectures
36 round table sessions which included topics like wellness, problem-solving, collaborative solutions, and “birds of a feather” breakout discussions
9 virtual video microscopy sessions
8 session dedicated to laboratory professionals covering hematology, chemistry, microbiology, and blood banking
6 resident board review sessions
15 companion society sessions
14 sessions related to wellness
4 sessions discussing diversity and inclusion
10 COVID-focused sessions
20 grant funded sessions
4 virtual patient symposia (more on this topic below…) and
And 300+ posters!
Image 2. More visual appreciation here: virtual sessions felt like you were really in a large, collective meeting of enthusiastic, like-minded laboratory professionals all learning, collaborating, and networking together!Image 3. I was fortunate enough to to speak on this amazing panel regarding direct patient-and-pathologist interactions, making laboratory medicine and the overal healthcare experience, safer, more accessible, more interdisciplinary, and better equiped at dealing with the forefront of medical diagnostics!Image 4. So, the session went well! Just look at that social media data: 36 million impressions over 3.5 days! That’s 1 million people engaging ASCP topics a day, or 12 people per second! All actively discussing and collaborating topics in pathology and laboratory medicine.Image 5. How could I (of all people) ignore the fact that #ASCP2020 featured an amazing social (media) lounge where people from all over could connect, chat, network, and relax! There were interactive, virtual sessions covering all kinds of non-lab med stuff: yoga, meditation, mixology, and cooking! I hope this is a permanent addition to future (hopefully) hybrid in-person/virtual meetings.
What more could you ask for? The folks that run the logistics and planning for the ASCP Annual Meeting outdid themselves again. Sure this content would excite anyone in the field for 3 dedicated days of immersive learning and networking, but all this and more are still available online for virtual on-demand recorded viewing! Missed a session? No worries, it’s still waiting for you for about 6 months (through March of 2021). All the buzz aside from ASCP members having free access to all of this content, the excitement started months before the meeting went live. Estimates are still coming in, but membership grew by a couple hundred in the weeks leading up to the meeting—not surprising: free access for members? That was an excellent deal, so choice.
Image 6. The start of the #ASCPSoMeTeam’s amazing trajectory culminated at #ASCP2019 in Arizona, the more we work together the more we can accomplish for our profession and our patients, #StrongerTogether.Image 7. ASCP’s Resident & Pathologist Councils are invaluable assets to promoting and advancing all of our professional development. #ASCP2020 was no different! From virtual fellowship fairs to online, interactive resident council sessions, there was a lot to take it—still available online!Image 8. I’ve talked about previous ASCP Annual Meetings here and here, and while I can’t list every single aspect of what made this meeting (virtually) amazing, members can check in for about 6 months and see for themselves the quality and attention to detail that comes directly from our collective passion to make pathology and laboratory medicine better, for everyone. Kudos to the ASCP leadership and logistics teams that made this all possible!
Great to see you all at the meeting!
Thanks for reading! See you next time!
-Constantine E. Kanakis MD, MSc, MLS (ASCP)CM is a new first year resident physician in the Pathology and Laboratory Medicine Department at Loyola University Medical Center in Chicago with interests in hematopathology, transfusion medicine, bioethics, public health, and graphic medicine. His posts focus on the broader issues important to the practice of clinical laboratory medicine and their applications to global/public health, outreach/education, and advancing medical science. He is actively involved in public health and education, advocating for visibility and advancement of pathology and lab medicine. Watch his TEDx talk entitled “Unrecognizable Medicine” and follow him on Twitter @CEKanakisMD.
If you read my last blog, you heard the about the story “if You Give a Mouse a Cookie” by Laura Numeroff.4 The curious little mouse has a mind that never rests. As his mind wanders and hops from one thing to another, he keeps discovering more things to check out along the way. Medical laboratory lcientists are a lot like this. We’re a curious bunch, and, in investigations, one thing often leads to the next. Well folks, the mouse has struck again! We were given another cookie in the form of these beautiful cells.
Image 1. Lymphocytes with intracytoplasmic inclusions.
These cells were found by my coworker Liz Marr, MLS(ASCP), and the adventure began! First, we wanted to know what those were, and then we needed to find out more about them, and then, mostly, I wanted to know why in almost 40 years of working in and teaching hematology that I have never before seen this!
The story begins with our case history. We received a CBC from a 71 year old female with a 4 year history of untreated chronic lymphocytic leukemia/ small lymphocytic lymphoma(CLL/SLL). The patient’s recent history included a myocardial infarction(MI) 5 months prior. The patient was found to have leukocytosis (WBC 25.38 x 103/μL) and absolute lymphocytosis (18.25 x 103/μL) with normal hemoglobin and hematocrit (Hgb 13.4 g/dL, Hct 40.8%) and normal platelet count (272 x 103/μL). The differential had 71.9% lymphocytes with many abnormal forms noted. The slide was sent for a pathology review. The pathologist reported “Atypical lymphocytosis consistent with patient’s known chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) Filament-like inclusions are present in the cytoplasm which has been previously reported in patients with CLL.”
Image 2. Lymphocytes with crystalline-like inclusions.
A curious tech can’t stop at just that description. If you tell me they are filament-like inclusions, I will have all kinds of questions. What are these filaments made of? Are they crystals, or something else? How common are these? Are these diagnostic of CLL? Are these only seen in CLL? What is their significance? And, of course, the most puzzling question, why have I never seen these before??
CLL is a form of non-Hodgkin lymphoma and is the most common leukemia in the Western world. It is generally a leukemia of older age with a median age at diagnosis around 67-72. The disease is widely variable, with some patients asymptomatic and requiring no treatment for many years, while others have a more rapidly progressive course of disease requiring treatment. About 60% of patients are diagnosed before they exhibit any symptoms. CLL and SLL are considered to be different manifestations of the same disease. In CLL, the abnormal B lymphocytes are found mostly in the peripheral blood and bone marrow, but in SLL, there is lymph node involvement, with abnormal cells mostly found in the lymph nodes. CLL is diagnosed based on absolute B lymphocyte counts ≥5 x 109/L. Flow cytometry typically reveals a distinctive cell immunophenotype with expression of CD19, CD5, CD23, and Κ/λ; and weak expression of CD20, CD79b, and surface immunoglobulin.1
The most recent flow cytometry report on our patient was from one year ago. An 8 color analysis with CD45/SSC gating was performed by LabCorp. The flow revealed an abnormal cell population representing 56% of total cells. Two monoclonal B cell populations were detected with identical phenotypes except for light chain expression. These cells expressed CD45, CD19, CD20, CD22, CD5, and CD23., CD38-. This phenotype was consistent with her previous diagnosis of CLL/SLL.
A literature search revealed only a few articles about intracytoplasmic inclusions in CLL. Cytoplasmic inclusions in lymphomas are uncommon, but have been noted as vacuoles, crystals, and pseudocrystals. These crystalline inclusions represent immunoglobulin(Ig) heavy and light chain that precipitate in the cytoplasm. Using electron microscopy it has been found that theses Ig deposits localize in the rough endoplasmic reticulum (RER).5 When surface Ig can be demonstrated on the B lymphocytes, it has been found to be same as Ig in the inclusions.6
In two published studies that describe these crystal like inclusions, photographs are very similar to the ones we found on our patient.3,5 It is interesting to note that, in these two studies, neither of the subjects was a known CLL patient. The inclusions were noted in the patients’ cells and the peripheral blood was subsequently sent for flow. Phenotypes reported confirmed monoclonal B-cells representing a large percentage of cells. Huang reported monoclonal B-cells which expressed CD45, CD19, CD20, CD22, CD79b, CD5, CD23, CD148 and CD200(hi), with partial expression lambda, and negative for FMC7, CD10, CD11c, CD49d, CD103, CD38, CD25, CD160, IgM, CD81, kappa and Ki67.3 In the Ramlal case study, phenotype was CD5, CD19, CD20, CD23, positive, CD10, FMC7 negative.5 On the basis of flow, along with the CBC results, the patients were diagnosed with CLL.
Of course, while researching this, the little mouse in me kept asking questions and finding more questions to ask. One question that I still had questions about was if these inclusions have any prognostic value. In three recent studies3,5,6 it was indicated that these inclusions can be used to help with diagnosis, but are not prognostic for course of disease. Rodriguez followed a patient with asymptomatic Rai stage 0 CLL. This patient consistently had inclusions noted in lymphocytes for 9 years before any progression of disease was noted.6 In the medical field even if one study reports no prognostic significance, this opinion could change in the future with more studies. Could these crystalline inclusions be used to forecast time to first treatment (TFT) or overall survival?(OS). So far, because of the rarity of these cytoplasmic inclusions, there is no evidence of prognostic value. As well, the mechanism related to their formation and their role in CLL is yet to be determined.
Our case study patient and the various reports found in literature had common flow cytometry immunophenotypes. Patients were all either previously diagnosed with CLL or lymphocytic lymphoma, or were diagnosed at the time of the findings of these inclusions. While these crystalline inclusions alone are not considered diagnostic for CLL, their recognition can be used to assist in a prompt diagnosis of a lymphoproliferative disease. And they are so pretty! What medical laboratory scientist doesn’t love pretty cells? Be like that mouse. Be curious, keep your eyes open, and be on the lookout for these interesting cells in CLL patients, but, more importantly, in patients with lymphocytosis without a known diagnosis of a lymphoproliferative disorder.
References
AJMC, January 7, 2019
Chronic Lymphocytic Leukemia: An Overview of Diagnosis, Prognosis, and Treatment
Numeroff, Laura If You Give a Mouse a Cookie. 1986
Ramlal, B, DiGiuseppe, JA. Intracytoplasmic crystalline inclusions in chronic lymphocytic leukemia. Clin Case Rep. 2019; 7: 1460– 1461. https://doi.org/10.1002/ccr3.2250
Cecilia M. Rodríguez, Carmen Stanganelli, Claudio Bussi, Daniela Arroyo, Darío Sastre, Viviana Heller, Pablo Iribarren & Irma Slavutsky (2018)Intracytoplasmic filamentous inclusions and IGHV rearrangements in a patient with chronic lymphocytic leukemia, Leukemia & Lymphoma, 59:5,1239-1243, DOI: 10.1080/10428194.2017.1370549
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
In my previous post here on Lablogatory, I discussed the diagnosis and comparison of two mediastinal fine needle aspiration (FNA) cases – thymoma and thymic carcinoma. I tooted my own horn of how I instantly recognized the tumors on Rapid On-Site Evaluation (ROSE), as the characteristics were exactly how I remembered them from my cytology knowledge bank formulated in grad school. Here’s a case that completely threw me off my game. I had never seen this type of tumor nor heard of it, at least not to my memory, but that’s the beauty of lab medicine—we’re continuously learning.
A 43 year old female with hypertension and no cancer history presented to a vascular surgery clinic for treatment of varicose veins, and an ultrasound was performed, noting a mass in the left inguinal region. The patient subsequently had an MRI, which demonstrated a predominantly fatty mass in that area with enhancement and probable necrosis within the lesion. The differential diagnosis determined by imaging was fat necrosis versus liposarcoma. With this risk of malignancy, the patient came to our institution for biopsy and further guidance. The ultrasound department visualized the left inguinal mass of mixed echogenicity, measuring 3 centimeters with a focal area of central necrosis.
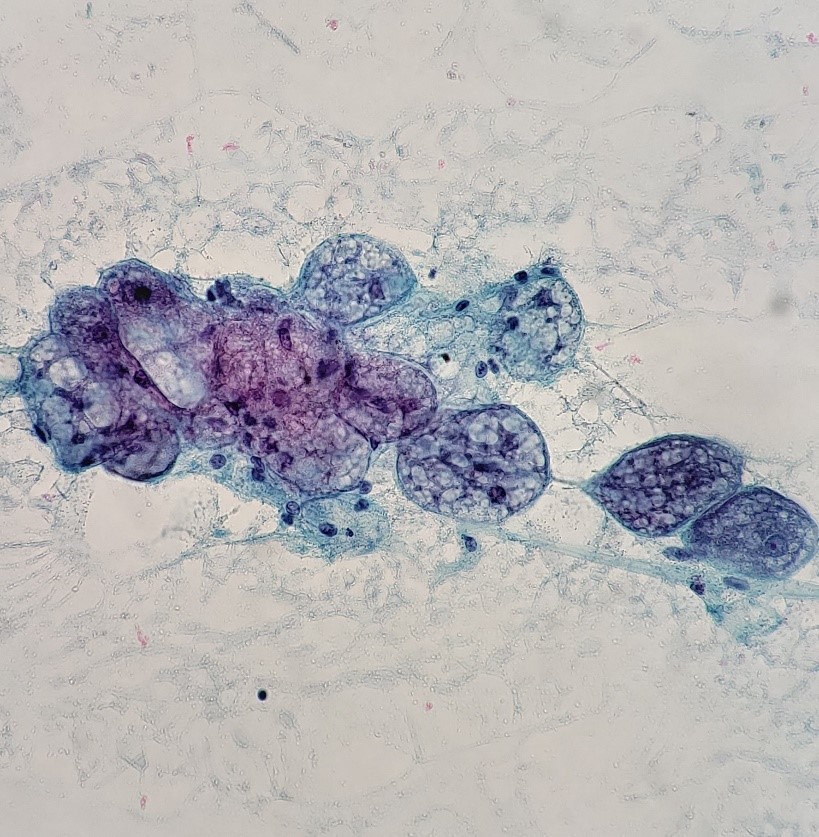
After receiving two FNA passes of the patient’s left inguinal mass from the radiologist, I made mirror-image smears of the samples, air-drying one slide for Rapid On-Site Evaluation (ROSE), fixing the other in 95% Ethanol, and rinsing the needles in Hanks Balanced Salt Solution to later make a FFPE-Cell Block.
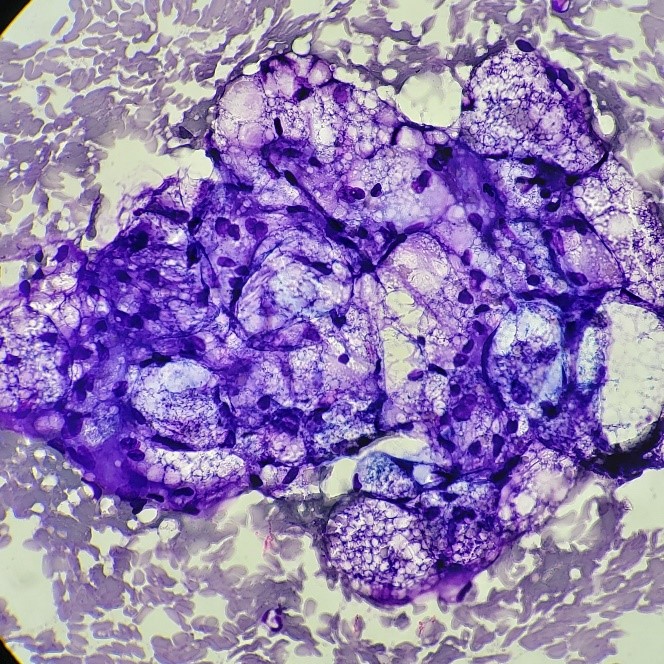
Image 1. Left inguinal FNA, DQ-stained smear. Image 2. Left inguinal FNA, Pap stained smear. Image 3. Left inguinal FNA. H&E cell block section.
I remember my differentials – Lipomatous tumor of unknown etiology versus clear cell renal cell carcinoma versus adrenal cortical carcinoma. I knew it was a neoplasm of sorts and that we had adequate material for a diagnosis. But I could not make a definitive diagnosis, and it mind-boggled me. That’s when my cytopathology director reviewed the case with me, and I went straight to the cytology encyclopedias.
The FNA specimen was signed out as a “Benign-appearing adipose tissue neoplasm, consistent with hibernoma.
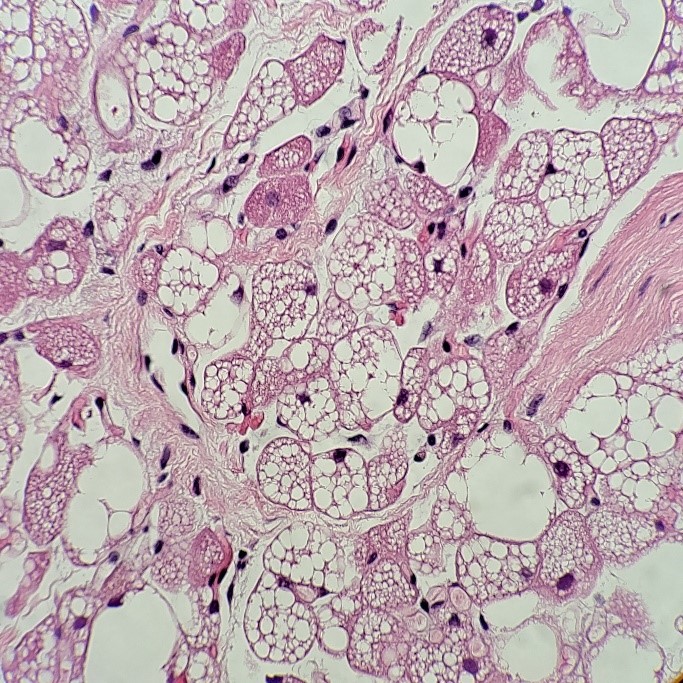
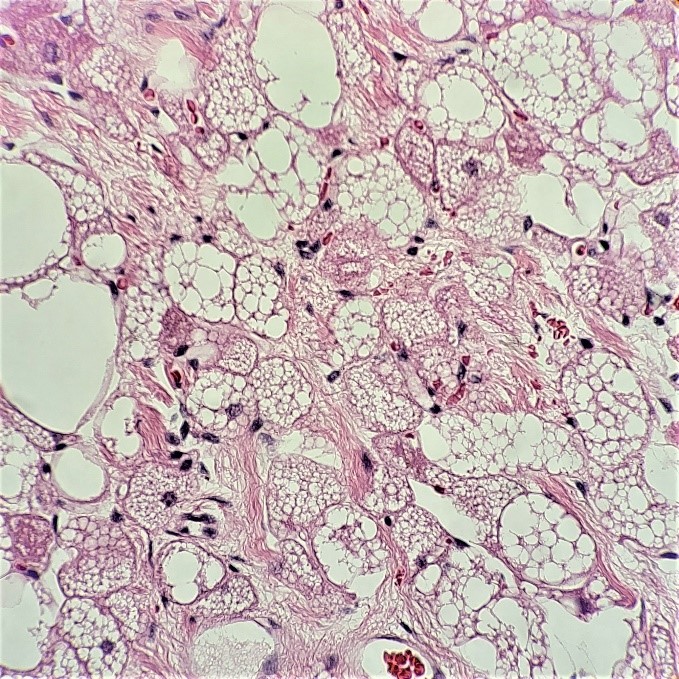
Image 4. Left inguinal core biopsy, H&E section 100X. Image 5. Left inguinal core biopsy, H&E section 400x.
Hibernoma was also diagnosed on the concurrent core biopsy specimen by the surgical pathologist on service.
Hibernomas are rare brown fat tumors that typically develop where brown fat is normally distributed throughout the body, such as the upper back, thigh, and retroperitoneum.2 Brown fat, or brown adipose tissue is responsible for non-shivering, mitochondria-rich thermogenesis.3 From the cytology images, one can appreciate the small, eccentric nuclei and capillaries, featuring three cell types: mature adipocytes (think lipoma), lipoblast-like cells (think liposarcoma), and hibernoma cells, which appear to be highly, but uniformly vacuolated adipocytes with granular cytoplasm.
Two months after the initial biopsy, the patient underwent a radical resection of her left thigh hibernoma en bloc with a portion of the iliopsoas muscle and femoral nerve neurolysis. The intraoperative findings showed a 5.2 centimeter well-circumscribed mass directly beneath the femoral vessels, beginning at the common femoral artery and extending to the level of bifurcation of the superficial femoral artery and profunda. The mass was adherent to the posterior wall of the vessel, but fortunately did not involve the adventitial layer. The mass, however, was more adherent to the pectineus muscle and inseparable from the middle portion of the iliopsoas muscle. The mass was also adherent to the hip, and in order to clear the mass from that space, an arthrotomy was made.
Image 6. Left inguinal resection, H&E section 100 x. Image 7. Left inguinal mass resection, H&E section 400x.
The surgical pathologist signed out the case as follows:
– Hibernoma with focal myxoid changes, 5.3. cm. The inked margins showed no tumor.
In the middle of the hibernoma, there was a nodular myxoid lesion with spindle cells. Due to a question of liposarcoma, cytogenomic microarray analysis (CMA) was performed which was negative for genomic imbalances. Immunostain performed on a frozen section of tissue showed that the atypical cells were positive for Desmin, confirming that they are skeletal muscle.
If this case was diagnosed as a liposarcoma rather than hibernoma, one would see atypical lipoblasts with more prominent capillaries, like a well-differentiated liposarcoma. Depending on the type of liposarcoma, one might also identify a myxoid stroma or round cells.2
Hibernomas are a unique kind of tumor where the consensus on how to manage them remains split – some favor observation, while others suggest surgical intervention. From the literature, there are no reports to suggest metastasis or malignant degeneration/transformation, but many do favor a resection if feasible.1
References
AlQattan, A. S., Al Abdrabalnabi, A. A., Al Duhileb, M. A., Ewies, T., Mashhour, M., & Abbas, A. (2020). A Diagnostic Dilemma of a Subcutaneous Hibernoma: Case Report. American Journal of Case Reports, 21, 1–5. https://doi.org/10.12659/ajcr.921447
Cibas, E. S., & Ducatman, B. S. (2009). Cytology: Diagnostic Principles and Clinical Correlates, Expert Consult – Online and Print (3rd ed.). Saunders.
Cypress, A., & Khan, C. (2010). The Role and Importance of Brown Adipose Tissue in Energy Homeostasis. Curr Opin Pediatr, 22(4), 478–484. https://doi.org/10.1097/MOP.0b013e32833a8d6e
Taryn Waraksa, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
Working bacteriology benches in the clinical microbiology laboratory often comes with its fair share of questions about the susceptibility of patient isolates. In training, we are taught about breakpoints – clinically essential values which determine if an organism is susceptible, resistant, or somewhere in-between for a given drug. These values are readily accessible to us in guidance documents (e.g., CLSI M100, FDA website), and are programmed into instruments to allow for automated interpretation. But, have you ever wondered how these values are derived? Raw microbiological and pharmacological data, patient outcomes, and regulatory considerations must be examined through multiple lenses, and by many different entities, before these values ever make it to the printed page and used clinically. Here, we will highlight some of the “moving parts” of breakpoint determination an effort to demystify this process and gain a better understanding and appreciation of the clinical application of these life-saving measurements. To help, I’ve recruited two of our outstanding infectious disease pharmacists from UT Southwestern Medical Center to enhance this discussion. It’s my hope we will all learn something in the process!
Breakpoint Breakdown – The ABC’s of MICs and ECVs, plus Pharmacology 101!
A breakpoint represents a defined antibiotic concentration or zone of inhibition diameter that serves as a gatekeeper for antimicrobial use. This value categorizes organisms as susceptible, susceptible-dose dependent, intermediate, resistant, or nonsusceptible to various antimicrobials. As such, is an indispensable component of appropriate and effective antimicrobial prescribing.1 Breakpoints are set through a rigorous examination of data by various national and international organizations which we will discuss in a later post. Determining the optimal value at which a breakpoint should be set is multifactorial, requiring a multidisciplinary approach to incorporate data from bench and bedside. Now, if that introduction sounded daunting, don’t panic! We’re going start at the beginning with basic biological measurements of susceptibility that are needed to begin to establish a breakpoint. For those not currently working in microbiology (or if it’s been a while), a basic understanding of susceptibility testing mechanisms is necessary and we will briefly review here. Bacteria will be the focus for this discussion, but many of these concepts are also broadly applicable to fungi as well.
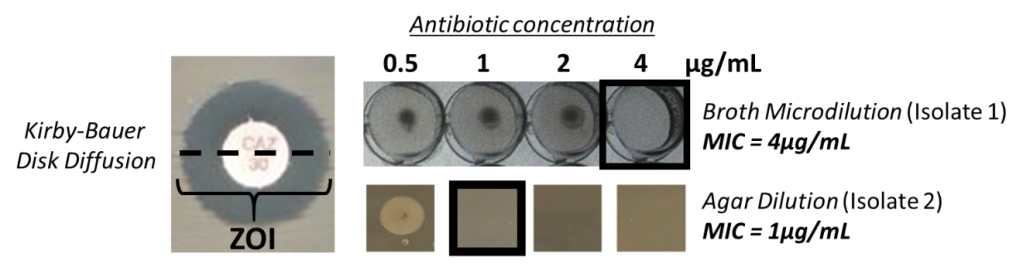
Determination of susceptibility to an antibiotic can be evaluated by examining the response of a bacterial isolate to antimicrobial exposure. In the laboratory, this is usually achieved through dilution, whereby an isolate may grow at some drug concentrations, and growth is inhibited at others. Dilution of the antimicrobial can come either through directly applying the antibiotic at defined concentrations uniformly to growth media (i.e. broth dilution, agar dilution), or utilizing a diffusion gradient through media when an antibiotic is applied at a single source (i.e. disk diffusion) (Image 1). Application of defined antibiotic concentrations to the growth media allows for a minimal inhibitory concentration (MIC) to be determined, while a diffusion gradient allows for a zone of inhibition to be measured (ZOI). An MIC is the lowest concentration of antimicrobial that inhibits organism growth of an isolate. This value is unique to the isolate that is being tested. However, when establishing a broad measurement which will encompass all isolates of that species (or group of species) such as a breakpoint, it’s easy to imagine that significantly more data is needed.
Image 1. Three methods of antimicrobial susceptibility testing. Kirby-Bauer disk diffusion generates a zone of inhibition – the diameter of that zone is measured and correlated with MIC data to establish breakpoints. Broth and agar dilution are two dilution methods which directly generate an MIC as an endpoint; the lowest concentration of antibiotic in which growth is inhibited. In the broth microdilution experiment, isolate 1 has an MIC of 4μg/mL. In the agar dilution experiment, isolate 2 has an MIC of 1μg/mL.
Thus, a first step in setting an optimal breakpoint begins with an antimicrobial’s in vitro activity against an organism. A descriptive summary of the MIC range across a given species helps define the MIC distribution. This analysis usually includes MICs from hundreds of tested isolates! This MIC distribution helps to define epidemiologic cutoff values (ECV or ECOFF). Like a breakpoint, these values separate the MIC distribution into bacterial populations that are either wild-type, and those with resistance. The wild-type MIC distribution aims to exclude outlier MICs that may represent organisms with acquired resistance (either through mutation or acquisition of resistance determinants) reflected by elevated MICs. An isolate in the population with an MIC above the ECV is likely to have acquired resistance, whereas an isolate with an MIC lower than the ECV likely originates from the wild-type distribution and lacks mechanisms of acquired resistance or reduced susceptibility.2 So great, we have an experimental MIC value which separates wild-type organisms from ones that have acquired resistance, why not just stop there and call it a breakpoint? The answer is the ECV does not account for host responses, clinical outcomes, site of infection, pharmacokinetics/pharmacodynamics, dosing, and a number of other important variables which go into establishing a clinical breakpoint. Thus, using ECVs for clinical decision making is challenging.
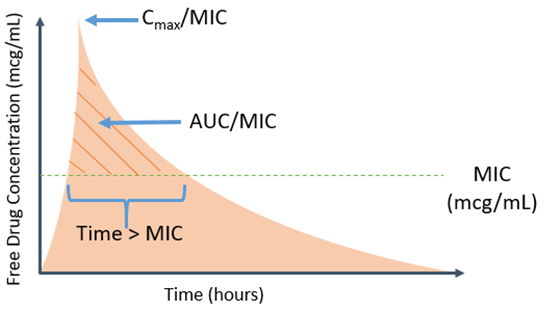
Now that we have considered some aspects of the microbiological side of the equation, let’s switch gears and look at the host and other factors not addressed by an ECV. Pharmacokinetic (PK) and pharmacodynamic (PD) parameters are key to assessing the clinical applicability of a breakpoint. PK parameters represent how the body handles the antimicrobial, including absorption, distribution, metabolism and elimination, whereas PD parameters represent the effect between the drug and bug. Taken together, PK/PD parameters represent the relationship between drug concentration (PK) and antimicrobial effect (PD) over time. Different antimicrobials have distinct PK and PD characteristics, thus several PK/PD indices are utilized to determine optimal target concentrations or exposures that improve antibacterial efficacy. Common PK/PD indices are the percent of time the free drug concentration remains above an organism’s MIC (fT > MIC), the ratio of free max drug concentration (or peak) to MIC (fCmax/MIC), and the ratio of free drug exposure (area under the curve, AUC) over a 24-hour period to MIC (fAUC/MIC) (Image 2).3
Image 2. Common PK/PD Indices
For example, β-lactam antimicrobials require 40-60% fT > MIC for maximum antibacterial efficacy; however, the exact fT > MIC (or other exposure) required for optimal efficacy varies between different β-lactam antimicrobials and bacterial species. Importantly, the desired antimicrobial exposure should be obtainable based on the established breakpoint, meaning the β-lactam of interest should achieve 40-60% fT > breakpoint. Various strategies are employed to optimize PK/PD parameters relative to a given breakpoint (more on that to come in Part 2 of this series). These target exposures are calculated from data for each bug-drug combination.
Of note, the antimicrobial exposure in relation to MIC is often based on antimicrobial blood concentrations. However, this is obviously not always the site of infection. The same bug-drug combination can have multiple breakpoints specific to infection site. For example, central nervous system (CNS) infections may have lower established breakpoints compared with non-CNS infections. The use of a lower breakpoint improves PK/PD target attainment in areas where there may be low drug concentrations, such as the CNS. For CNS-specific breakpoints, only organisms with MICs within the lower range of the MIC distribution will be deemed susceptible. With a lower MIC, the PK/PD exposure may be more obtainable given the potential poor drug penetration to the site of infection.
Outcomes from clinical data are often deemed the most important factor used to determine breakpoints. Treatment successes or failures of an antimicrobial against a specific MIC may provide validity to an established breakpoint or support revision. For example, the piperacillin-tazobactam breakpoint for Pseudomonas aeruginosa, was lowered from 64/4 mcg/mL to 16/4 mcg/mL due to an increase in mortality observed in patients who had organisms with MICs 32 or 64 mcg/mL.4 Unfortunately, clinical outcome data is often influenced by other confounders beyond antimicrobial therapy and the organism’s MIC, such as source control and other therapeutic interventions. Furthermore, clinical data for “resistant” organisms may not be available, limiting the assessment of the antimicrobial against organisms with high MICs.
Finally, it is important to remember that breakpoints are not set in stone and change regularly as more data become available. Common reasons for breakpoint revisions include: 1) new PK/PD data suggesting the breakpoint is too low or high based on antimicrobial exposure, 2) identification of novel resistance mechanisms, and 3) new clinical data to suggest poor correlation of clinical response with the established breakpoint. Furthermore, microbiological methods may become more accurate and ultimately affect quantification of the MIC.5
In summary, establishing a breakpoint is not a straightforward process and requires an aggregate of information. We are really only scratching the surface of the very complex process here, but hope that this sheds some light on where these important values originate. Various types of data; microbiological, pharmacological, in vitro, in vivo, they all create the story. However, a complete picture is often not available at the time of breakpoint creation, resulting in the need to constantly review and update breakpoints as more data becomes available.
Next post we will discuss how breakpoints are used at the bedside.
References
Clinical and Laboratory Standards Institute. Development of In Vitro Susceptibility Testing Criteria and Quality Control Parameters, 5th Edition (M23).
Craig WA. Pharmacokinetic/pharmacodynamic parameters: rationale for antibacterial dosing of mice and men. Clin Infect Dis. 1998 Jan;26(1):1-10; quiz 11-2. doi: 10.1086/516284.
Tam V, et al. Outcomes of bacteremia due to Pseudomonas aeruginosa with reduced susceptibility to piperacillin-tazobactam: implications on the appropriateness of the resistance breakpoint. Clin Infect Dis. 2008 Mar 15;46(6):862-7.
Humphries RM, Abbott A, Hindler JA. Understanding and Addressing CLSI Breakpoint Revisions: a Primer for Clinical Laboratories. J Clin Microbiol. 2019 May 24;57(6):e00203-19.
-Marguerite Monogue, PharmD is an infectious diseases pharmacy specialist and assistant professor at the University of Texas Southwestern Medical Center in Dallas, Texas. She is interested in antimicrobial pharmacokinetics/pharmacodynamics and multi-drug resistant Gram-negative bacteria.
-James Sanders, PharmD, PhD, is an infectious diseases pharmacy specialist and assistant professor at the University of Texas Southwestern Medical Center in Dallas, Texas. His academic and research interests are focused on multi-drug resistant Gram-negative bacteria, surgical site infections and HIV pharmacotherapy.
-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.
A 35 year old man presented to the Emergency Department (ED) with intermittent chest pain for 3-4 days, abdominal pain, fatigue, and lightheadedness over the same time period. Additionally, his family reported symptoms of progressive malaise for about a month, worse over the last week. In the ED, he was found to have ST elevations in the inferior leads of the electrocardiogram, which can be indicative of a heart attack. He was given 325 mg of aspirin and was emergently taken to the catheterization lab. He was found to have multiple complete occlusions in the distal left anterior descending artery (LAD), posterior descending artery (PDA), and posterior left ventricular artery (PLV). He underwent aspiration thrombectomy and the resulting clots were thought to be emboli; segments were sent to pathology for histopathologic evaluation and to microbiology for culture. There was no evidence of underlying plaque. He was admitted for management of ST-elevation myocardial infarction (STEMI). While in the ED, he was found to have white blood cell count of 23,000 and tachycardia to 110 beats per minute. A transthoracic echocardiogram demonstrated thickened aortic valve leaflets with evidence of leaflet destruction, severe aortic insufficiency, and right coronary cusp perforation which are consistent with endocarditis. Blood cultures were obtained and he was started on broad spectrum antibiotics (Vancomycin and Cefepime).
He has a past medical history significant for previous shoulder abscess with Methicillin-resistant Staphylococcus aureus (MRSA) and intravenous drug use (IVDU) (heroin, last use ~6 days prior to admission).
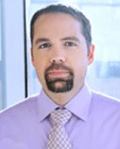
Computed tomography (CT) of his abdomen and pelvis revealed multiple renal infarctions and a splenic infarction (Image 1). In addition, the CT of the brain showed: “Multifocal scattered supratentorial and infratentorial subarachnoid hemorrhages and findings suggestive of evolving ischemic infarct involving the right inferior frontal gyrus, without evidence of hemorrhagic transformation currently. No midline shift or other complication identified.”
Image 1. Computed tomography of the abdomen demonstrating multiple renal infarctions (left, circled) and a splenic infarction (right, circled).
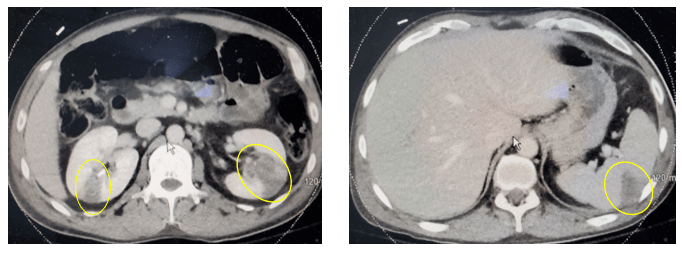
On hospital day 1 (HD1), both sets of initial blood cultures turned positive with gram positive cocci (GPC) in clusters and thrombectomy cultures were also growing GPC in clusters (Image 2). On HD2, the GPC in the thrombectomy culture was identified as Rothia mucilaginosa. GPC growing in the blood cultures were also Rothia mucilaginosa (Image 2). The patient was continued on Vancomycin. Repeat blood cultures were obtained after catheterization on HD0, and HD2, which were negative. On HD2, the pathology of the initial clots showed “fibrinopurulent debris and fibrin plaques with innumerable cocci in clusters” (Image 3).
Image 2. Microscopic and culture morphology of Rothia mucilaginosa. Left: Gram stain from a blood culture demonstrating groups of Gram-positive cocci in small clusters (1000x magfication, oil immersion). Right: Blood agar plate with mucoid light pink-gray colonies.Image 3. Hematoxylin and eosin stained slide of formalin fixed paraffin embedded tissue of the thrombus removed during the initial emergent catheterization procedure. Sections demonstrate fibrinous material with entrapped white cells and innumerable cocci. Top: 100x magnification; Bottom: 400x magnification.
On HD3, the patient developed 10/10 chest pain with troponin elevation and T-wave inversion. He was taken back to the catheterization lab for another procedure where he was found to have recurrent, complete occlusion of the PDA with unsuccessful recanalization due to the dense thrombus. On HD6, he developed tamponade physiology due to a large pericardial effusion that was drained. Cultures of the pericardial fluid were negative. Given the recurrent embolization events, the patient was transferred to another hospital to undergo aortic valve replacement surgery and coronary artery bypass graft surgery. Cultures taken at the time of the valve replacement surgery were negative and the valve tissue was not sent for pathologic evaluation.
Discussion
We present an uncommon case of extensive Rothia mucilaginosa sepsis with septic emboli and endocarditis. Rothia mucilaginosa has experienced the scientific name-change game over the last several decades. It was first identified as Micrococcus mucilaginosus, then became Stomatococcus mucilaginosus, was also known as Staphylococcus salivarius before finally arriving to today’s name of Rothia mucilaginosa.1,2R. mucilaginosa is a normal inhabitant of the oropharynx and is often associated with dental caries.3R. mucilaginosa can cause invasive infections, typically in patients with compromised immune systems, disrupted mucosal barriers or injection drug use.4
R. mucilaginosa is a facultatively anaerobic, gram positive, non-fastidious coccus that is coagulase negative but with variable catalase positivity. Colony morphology is usually white to gray nonhemolytic colonies with a mucoid appearance. Although the variable catalase reaction may point toward a Streptococcus spp., the Gram stain morphology of clusters helps to rule it out. Although not all strains are mucoid, the classic colony morphology is wet and is due to polysaccharide capsule.
The organism is generally susceptible to antibiotics designed to target gram positive bacteria including, penicillin, ampicillin, cefotaxime, rifampin and vancomycin.4 It is important to note that R. mucilaginosa is not predictably susceptible to clindamycin, trimethoprim-sulfamethoxazole or ciprofloxacin.5 The patient presented in this case received intravenous vancomycin in part due to the extensive disease on presentation, but also because he was at risk for methicillin-resistant Staphylococcus aureus (MRSA) sepsis and had a previously documented abscess from MRSA.
References
Bergan T, Kocur M. 1982. Stomatococcus mucilaginosus gen. nov., sp.nov., ep. Rev., a member of the family Micrococcaceae. Int. J. Syst.Bacteriol. 32:374-377
Collins MD, Hutson RA, Baverud V, Falsen E. 2000. Characterization of a Rothia-like organism from a mouse: description of Rothia nasimurium sp.nov. and reclassification of Stomatococcus mucilaginosus as Rothia mucilaginosa comb.nov. Int. J. Syst. Evol. Microbiol. 3:1247-1251.
Trivedi MN, Malhotra P. Rothia prosthetic knee joint infection. 2015. J. Microbiol. Immunol. Infect. 48(4):453-455.
Bruminhent J, Tokarczyk MJ, Jungkind D, DeSimone JA. Rothia mucilaginosa Prosthetic Device Infections: A Case of Prosthetic Valve Endocarditis. J. Clin. Microbiol. 5;15:1629-1632.
Kaasch AJ, Saxler G, Seifert H. 2011. Septic arthritis due to Rothia mucilaginosa. Infection. 39:81-82.
-Doreen Palsgrove, MD is a board certified Anatomic and Clinical Pathologist who joined the faculty at UT Southwestern as an Assistant Professor in 2019. She specializes in head and neck and genitourinary pathology.
–Dominick Cavuoti, DO is a professor of AP and CP at UT Southwestern, specializing in infectious disease pathology, cytology and medical microbiology.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
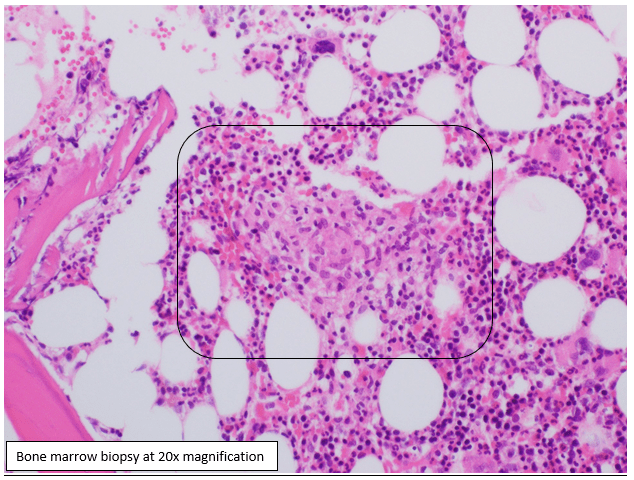
Case History An 83 year old male with bladder cancer was treated with Mycobacterium bovis Bacillus Calmette-Guérin (BCG), his last treatment occurring 1.5 months prior to presentation. He has a past medical history of chronic obstructive pulmonary disease, hypertension, obstructive sleep apnea, obesity, and diabetes. The patient has been hospitalized four times over the last two months and his symptoms include generalized weakness, malaise, shortness of breath and recurrent fever. He was found to have patchy lung infiltrates and he was diagnosed with pneumonia, COPD exacerbation and symptoms of heart filature. He was treated previously with antibiotics, steroids and fluid management which would temporarily relieve his symptoms. He presents to the hospital again, four days after his last hospital discharge, with generalized weakness, malaise, shortness of breath and recurrent fever. On initial evaluation he was found to be pancytopenic.
Laboratory Identification
Blood cultures were negative. A bone marrow biopsy was performed for fever of unknown origin and pancytopenia. The biopsy showed non-caseating granulomas which were negative for acid-fast bacilli (AFB) by Ziehl-Neelsen stain and fungal elements by Gomori Methenamine Silver Stain (GMS). A laboratory-develped PCR test for Mycobacterium tuberculosis complex (MTBC) was performed on the bone marrow and was negative. AFB culture of bone marrow was positive for after 30 days of incubation and the organism was confirmed to be acid-fast bacilli by auramine-rhodamine fluorescent dye and Kinyoun stain. A second laboratory-developed test that uses heat shock protein (HSP) 2 and HSP3 to determine species level identification of Mycobacteria identified the organism as M. tuberculosis complex. Due to the patient’s history, further identification was performed at a reference lab using specific oligonucleotides targeting the gyrb DNA sequence polymorphisms which is able to separate different members of the MTBC. The patient’s isolate contained a RD1 deletion which is specific for Mycobacterium bovis bacillus Calmette-Guérin (BCG).
Discussion
Mycobacterium bovis is a slow growing mycobacterium which produces rough, dry colonies on growth solid media. It is one of the species in the MTBC with a natural host of domestic and wild animals. Routine molecular tests will not accurately differentiate between members of the MTBC. For definitive identification of M. bovis, 16S rRNA and gyrB gene sequencing is necessary. Safe handling procedures should be followed prior to molecular testing of MTBC.
Mycobacterium bovis BCG is a live, attenuated strain of Mycobacterium bovis that was created for vaccine and is used in the treatment of superficial bladder cancer. The treatment may cause localized symptoms including hematuria, fever, nausea, and dysuria which are marker of anti-tumor effect. Serious complications occur in <5% of patients with complications including sepsis, pneumonitis, hepatitis, lymphocytic meningitis, bone marrow involvement, and mycotic aneurysms. The cardinal sign of BCG infection is a relapsing fever with drenching night sweats persisting beyond 48 hours. Disseminated infection can occur days to years after the therapy. Clinical suspicion should be high for M. bovis BCG dissemination if there are symptoms and a high grade fever ≥72 hours. Treatment includes a regiment of isoniazid, rifampin and ethambutol. Most isolates of M. bovis are resistant to pyrazinamide.
References
Lamm DL. Efficacy and safety of bacille Calmette-Guérin immunotherapy in superficial bladder cancer. Clin Infect Dis 2000; 31 Suppl 3:S86.
Shelley MD, Court JB, Kynaston H, et al. Intravesical Bacillus Calmette-Guerin in Ta and T1 Bladder Cancer. Cochrane Database Syst Rev 2000; :CD001986.
Richter E, Weizenegger M, Rusch-Gerdes S, Niemann S. Evaluation of Genotype MTBC Assay for Differentiation of Clinical Mycobacterium tuberculosis Complex Isolates. Journal of Clinical Microbiology 2003; 41(6): 2672-2675
UpToDate
-Crystal Bockoven, MD is a 4th year anatomic pathology resident at University of Chicago (NorthShore). Crystal has an interest in and will be doing a fellowship in pediatric and perinatal pathology. In her spare time, she enjoys reading, hiking and biking.
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.
A High Reliability Organization (HRO) is one that works with complex and hazardous systems every day and yet retains a high level of safety and an error free environment. The first recognized HRO industries were the United States Navy nuclear aircraft carriers , the Federal Aviation Administration’s Air Traffic Control systems, and nuclear power plant operations. These industries operate using highly complicated and dangerous processes, yet they have the fewest safety incidents.
The use of checklists is an important part of keeping safety incidents to a minimum. They can help employees avoid safety issues, avert disasters, and even aid in incident response. In aviation, a pre-flight safety checklist is a list of tasks that must be performed by pilots and crew before a take-off. Pilots also use checklists for both normal and non-normal operations, for landings, take-offs, and also for malfunctions, and emergencies. Checklists are usually printed on a card, and one card may be divided into as many as a dozen of separate checklists, each of which will be read aloud depending on the phase of a flight. Nuclear power plant operations also involve the use of many safety checklists.
A functional safety checklist features specific characteristics that aid the user in avoiding safety mishaps. Checklists should have defined pause points so users can determine when the list should be used and when new tasks should begin. Checklists types are also important, and the style used may vary depending on the task and the experience of the user. For example, a “do-confirm” list is generally used when users are experienced with the process and have gone through the necessary steps on the list and simply run through it to ensure the process is complete. A “read-do” checklist means employees perform the tasks as they read through each list item.
Most checklists should not be lengthy as it may tempt experienced users to take shortcuts or to ‘pencil-whip’ responses. Make sure the list includes crucial and potentially overlooked steps. These may be the things that can cause the greatest harm if not checked. Use language that is simple, precise, and use terminology that is familiar to the lab staff using the list. Lastly. Test the checklist to see that it fits the criteria above, and that it accomplishes the task set for it. The real goal of using a safety checklist is to create a cultural change by enhancing teamwork, increasing safety communication and changing the understanding of responsibility for safety within the department.
There are quite a few published lab safety checklists available for use. Here are just a few:
Your lab may have its own specific needs, and these checklists may not cover them, or they may be too much for your current issues. If that is the case, create a checklist that focuses on an issue or issues you’d like changed. For example, if PPE compliance is on the rise, create a list that can be used daily or weekly. Walk around and look for proper footwear, lab coat use, and face protection for example. Home made checklists can be scored and used as a quality monitor in order to show improvement in lab safety over time. Make sure people are trained to use the checklists properly, and that people are consistent in how they answer individual items. It’s always a good idea to alter who uses the safety checklists as well. Make sure everyone can use them, and that will create a broader understanding of the safety needs of the department. That can go a long way toward improving the overall safety culture. A review of checklists is always key. If there is a problem with a response for a particular item, it should never be ignored. In fact, it should be addressed quickly.
Many labs today do not fall into the category of a High Reliability Organization. Complex and dangerous tasks do occur in the field, but safety incidents are not uncommon. It may be because lab employees are not educated enough about the consequences. There are definite hazards when working in the lab setting, but often they are not in the forefront of the lab techs’ minds, safety is not made a priority. It needs to be discussed more. Or maybe the reason is that many of the hazards in the lab do not always have more immediate consequences. Organisms involved with exposures have incubation periods, and disease states (like cancer) can take years to develop after a safety incident.
In the airline and nuclear industries, if a safety error is made, the consequence is usually immediate, and deadly for many. Is that it? Is that why people don’t have the same reaction to safety issues in the lab? What can we do as safety professionals to change that? I believe we can change it- and it will take checklists, training and safety awareness.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
As we all find ourselves 9 months into 2020, which is arguably the worst year in living memory for many people, we face daily ongoing challenges of completing our work, finding work, adapting our work, feeding our children, schooling our children, preserving our health, caring for loved ones, and trying to not let the daily stress piped in from every communication channel send us over the edge. There are many people who have had a stellar year and have become richer beyond anyone’s imagining as the multitude of crises have fed their business models. There are many people we have lost prematurely due to an uncontrolled viral plague who would have contributed so much had they lived. Amidst all of this, there are individuals dealing with everyday problems in the chaotic setting of 2020—cancer, mental illness, disability, disparities, financial burdens, etc. Personally, I have a dear friend who was on the brink of a complete mental breakdown in 2019 for who I now feel I am on suicide watch 24/7. Life is normally hard, but it has certainly been abnormally hard for the past 9 months. I do not wish to point fingers, place blame, use hindsight, or make astute observations that are of no value—what my sports colleagues call the Monday quarterback effect. What I do want to do is open up to anyone reading this with a few of the things I have done in the last 9 months that have provided comfort and reminded me that, “This too shall pass.”
Take a stroll down memory lane – When I was younger, I used to take a lot of photographs with an actual camera and film. I would probably pass out if I knew exactly how much money I have spent in my life on buying and developing film. My dad was also an amazing photographer and probably knew more about taking traditional photographs than I know about infectious disease. During a certain period (end of high school through the beginning of residency – about 10 years), I was always taking photos and had at least three cameras all the time: a polaroid, an SLR, and point-and-shoot. I was not a very good photographer overall and most people quickly got annoyed with my constant snapping. But I am a collector so every photo I took was placed in an album. In organizing my garage on a Saturday recently when I was looking for anything to do because there was nothing really to do socially outside of my home, I made the decision to reorganize all of my photos into boxes by year and/or event and get rid of the photo albums. I do not recommend that unless you have a lot of time on your hands. But what I do recommend, and I greatly enjoyed, was going through EVERY photograph in my collection. There is a small box from when I was young that were taken by others as well as high school. There is a small box from college. There are literally 12 boxes from medical school and 6 boxes of my family. What did that mean in reality? I was incredibly happy in medical school. I remember being unhappy in high school and college. I have only a handful of friends each from high school, college, and medical school that I am in contact with regularly so no bias in that regard. But I wanted to remember medical school to a much greater degree than I had college or high school. My family is similar as I love my family. Seeing pictures of my grand parents who have all passed and my little cousins before they became grandparents made me feel happy and nostalgic. You have got photos somewhere (and I don’t mean the loads of ridiculous selfies on your Facebook account). Go dig them out and flip through them. If you find some true gems, post them on your social media. Share your memories and you will naturally smile.
Learn something new – We are inundated with information constantly but most of it is not knowledge. Most of it is simply status—the current state of people around us, all of whom will be dead and dust one day. One of my favorite lines from “The Terminator” is, “Look at it this way… In a hundred years, who’s gonna care?” All the tweets, all the posts, all the photos are fleeting moments of fluff (and probably rot your brain—scientific studies to be complete). But knowledge is forever and is precious. Do you know how to refinish an old piece of furniture? Do you know how to grow any type of plant from a cutting? When is the next time we will see Saturn chasing Jupiter across the sky? What happens to stuff you put in a recycling bin? Where does the electricity you use in your home come from? Can you name all 80 unique cultures in Ethiopia? The internet is full of a lot of garbage, but it is also full of incredible sources of knowledge. Sometimes (most of the time) we are so tired of looking at a computer or a smartphone or a tablet if we are working remotely that the last thing we want to do is engage with it further. Libraries are open so you can always resort to dusty old books which are also full of knowledge. Online classes are available for many things. Although cliché, TED talks can be cool. If you are feeling overwhelmed by all of the negativity, opinions, and bandwidth that’s given to things no one will care about in 100 years, turn your attention towards something pure and lose yourself in the nonpolitical world of knowledge. An expert is someone who knows everything that is true about a subject as well as everything that is false. Pick a topic, preferably something that does not come up in your work and set a goal to become an expert in that topic. There will always be people who know more than you do on any topic—but not every topic—but the point is to gain knowledge, grow your brain, and appreciate the permanence of truth.
Mindfulness, it’s really NOT a fad – I wouldn’t dare try to completely address the topic of mindfulness in a short blog, but I will challenge you to investigate it for yourself. Where my last suggestion is one to fill your brain with new ideas, information, processes, and thoughts so you master something external to yourself, mindfulness is the exact opposite. Learning to “turn your brain off” is an amazing skill that does take practice but has enormous benefits. And it is not really turning your brain off but rather turning down the volume on all the negative thoughts you have and may not even know it. Negative thoughts—internal or external—do not control you! They are your thoughts and the most powerful thing you can do is control them. There are many books on this subject, but my favorite is, “Mindfulness: An Eight-week Plan for Finding Peace in a Frantic World”. I will not lie to you. I read this book 5 years ago and have been practicing the techniques since then which did give me a leg up on the horror hurricane that is 2020. But it is never too late to reach inside yourself and find inner strength to deal with outer challenges. It is a bargain at less than $15 and will give you some amazing tools to use if you give it a chance. On a side note, if you are dealing with mental illness or you have a loved one who is dealing with mental illness, the most important first step is recognition, acceptance, and treatment. No one can be expected to defeat the external demons of the world when your internal demons have the chemical advantage. Recognize the signs and recognize the external amplifiers so you can be the hero for those who need you most during this time.
You’ve got to have friends – I remember in the not too distant past listening to “old people” say, “These darn kids need to stop playing video games and texting friends in the same room and get outside and play.” True? Yes. But now our reality has shifted to digital communications as the safest way to go to work, go to school, and see our friends. Zoom parties and the like have become extremely popular and I wrote about etiquette for these tools previously. But they are not the only way to communicate. Did you know that your smartphone is a phone? You can call and talk to people! All that paper junk mail that shows up in your snail mailbox is bidirectional. You can send people letters! This is all obvious and the vast majority if not all of you reading this have used some form of communication to talk to non-work people at least once in the last 24 hours. But do not take this for granted. There were people before our virally induced confinement that did not have large social networks or even limited ones. The isolation of our current situation is amplifying their loneliness. What am I asking you to do? You have a phone. You have social media. Dig through your contacts, find someone you have not talked to in a while, and reach out. Check on them. Check on your distant family members. Ask about them, how they are doing, and what is new in their life. Hearing their voice and laughing with them will make you smile on the inside and the outside.
Move – Your body. Daily.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.