One of the challenges of providing healthcare to patients of any type is “staying current” or “keeping up with the literature.” This can be especially challenging in the diagnostics laboratory where novel or unique approaches to a given test or test method or disease may show early promise but have no clinical utility, be too expensive, or not actually significantly change work-flow and/or patient value to justify implementation. On the other hand, sometimes a technology or test which is in development or approval can be so anticipated that clinicians and laboratorians are frustrated that it is not yet available.
In global health, there is a different problem that is encountered every day. There are technologies and tests that are approved, have documented clinical utility, and add great value to patients but they are simply not available because of supply chain, cost, administration, or geography. In such situations, the practitioners in these settings face extreme frustration—especially with stock-outs—and can become jaded and non-dependent on laboratory testing as part of care. This latter issue is a major challenge in cancer care where cancer diagnoses are required before treatment can begin; yet, in a large number of countries, access to cancer diagnostics routinely is not available. It is to that end that ASCP along with a whole host of NGO, industry, academic, and government partners are making great efforts to improve cancer care in each part of the continuum.
In this environment, however, disruptive innovations are, in fact, much easier to recognize as forthcoming. In the early 2000’s when I was working and traveling in Malawi, our project had a landline in the hospital to call the landline at the doctor’s house for issues overnight with patients. This required 24-hour nurses to be physically in the ward, tied to the phone and the patients. Landlines were expensive to install, had a very long waiting list to be installed, and, for the most part, the majority of the population in the country had never had a phone line in their dwelling. By the mid-2000’s, our project had one or more cellphones (as did the nurses) and communications through texting were nearly constant (especially since it was less expensive than making a phone call). By 2010, cell phones were ubiquitous in Malawi (and almost everywhere else in Africa) and there was no demand for landlines. Although this is a commonly used example, consider the adoption of cellular telephones and now smartphones in the US compared with Africa. There was push back, denial, avoidance, and even refusal to use them because there was an existing, well established system of landline communication. If you want to install cable television and internet in your home as late as 2016, you were often required to bundle with a landline. The point is that the adoption pattern was significantly different because there was a pre-existing competitor with the new technology although—clearly—the new technology was superior.
Now consider a woman of 35 years who has a breast mass on mammogram in downtown Boston today. She will likely have an imaging study with immediate ultrasound and fine needle aspiration and/or core biopsy subsequent. A pathological diagnosis will be issued within 3 to 4 business days (or sooner) which includes a histological diagnosis along with hormone receptor status and Her2 staining. She will see a clinician likely within a week for a positive cancer diagnosis and a treatment plan will be decided upon and executed. If we consider a similar woman in downtown Nairobi, Kampala, or Lagos, they may, in fact, have a similar experience because of the recent efforts globally to improve cancer awareness, diagnosis, and treatment. There may be some delays (reports may take several weeks), potential stock-outs, etc. but, in these major cities, the services might exist. They are likely, however, provided in private clinics, will cost a premium, and may or may not have any guarantees about quality.
The reality, however, is that the vast majority of women in the US or Europe who present with breast cancer do so at a very early stage because of active screening programs which include mammography. The vast majority of women in low- and middle-income countries (LMICs) present with later staged disease because of lack of screening. The latter group of women, however, often live in rural conditions and/or poverty conditions such that seeking care for a breast mass (of any size) will require them to spend time and money to travel to one of the major cities and attempt to access services. With this situation, many of these cancers are detected by the health system at a late stage where curative therapy windows have been missed.
Onto these observations let’s now overlay access to a test for a breast mass that can be performed on a fine needle aspiration biopsy and resulted in ~4 hours which will provide a diagnosis of cancer (or benign) along with prognostic features directing treatment. If we consider the woman in Boston, we may see such a test providing an incremental improvement in care because billing systems, litigation fears, compliance requirements, or accreditation standards still include routine histology and immunohistochemistry to be performed on a tissue biopsy. To some degree, the test may be rejected because it is adding a cost over the standard costs without adding value (other than speed) to the results. However, for the woman in the rural village who likely has access to a community health worker, access to such a test could mean that she starts oral therapy the same day she has the health visit without ever having to leave her village. We have now removed the journey to a clinic that can performed a biopsy, the costs associated with that travel, the time lost while traveling and waiting for a result, and removed the risk that this is not breast cancer—which would mean all the time and money were wasted. For this woman, enormous value is created for her with a test that is performed same day with immediate results.
This concept of point-of-care (POC) cancer diagnostics would arguable meet resistance in the US or European system because of competition with existing systems and other issues as mentioned previously. In an LMIC setting, as there may be no competition, such an innovation would sweep the system and become standard of care—almost regardless of cost. This last bit is very important because traditional systems for performing histology and IHC are complex, costly, and require multiple highly trained individuals to get a quality result. If that process costs $75 to $100 US dollars (to the health system) to provide and, for the individual patient, $10s to $100s of dollar for the travel, lodging, and lost wages, the cost of such a test could, in a stable, high-income country (HIC) market, fetch a hefty price. However, if such a test is priced at $25 to $50 USD (half the cost of the current system excluding the travel), the immediate replacement of the old system with this new system for the given indication must and will occur. This uptake is amplified in an LMIC when the POC test moves to the patient in a geographically distributed process. Breast cancer is an obvious target for such an approach because the tumors are easily accessible, the disease is quite common globally, and the primary therapies are very inexpensive. Could such a test have an impact in an LMICs for bone marrow-based, lung, bladder, colon, prostate, liver, kidney, or soft tissue tumors? The answer to that question lies in the availability of therapy, incidence of disease, and access to radiological equipment rather than availability of the actual POC device. That is, once you have a POC test for one cancer, creating a subsequent POC test for another cancer is a surmountable technical hurdle. But will such a test be able to have an impact because of the alignment of the other factors? It is likely that as you are reading this sentence, you have thought of a few yourself but there are certain cancers where you are likely thinking, “not possible”.
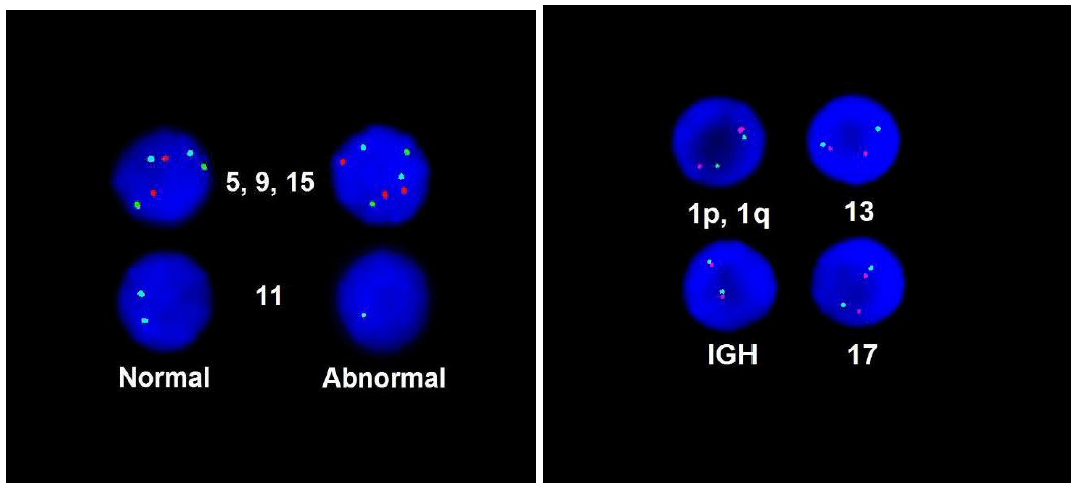
For breast cancer, two such POC approaches are coming down the pipeline. The first is the Cepheid GeneXpert Breast STRAT4 assay which measures quantitative RNA (qRNA) for ESR1, PGR, ERBB2, and MKi67. These four assays are surrogates for standard immunohistochemical staining for ER, PR, Her2, and Ki-67, respectively. In a series of published and in press feasibility and validation studies, the qRNA assay is essentially equivalent to IHC. There are nearly a dozen studies of this new testing cartridge using formalin-fixed, paraffin embedded (FFPE) tissue throughout Africa where the test is being compared to standard IHC. However, in at least one site, the test is being performed directly on FNA material. The second test is from the laboratory of Dr. Sara Sukumar at Johns Hopkins which uses a set of DNA methylation markers that can separate benign from malignant disease on FNA using only 10 markers. By combining these two approaches (benign vs. malignant followed by STRAT4 for positive tumors), a diagnosis of malignant breast disease with prognostic factors for treatment could be obtained in less than 4 hours.
Let’s jump forward to the point in time when both of these POCs are available (or, in fact, any POC for cancer is available). How would they change the approach to breast or other cancer in an LMIC? Because both tests require only an FNA of a mass and because tumors of the breast and other organs today are often late staged, community health workers could be trained to evaluate patients with masses, perform the sampling, and run the test in a remote village. Regardless of stage, starting a breast cancer patient on estrogen receptor antagonists can provide palliative relief or pre-surgical treatment. As a population down stages—which occurs as community health workers begin routine screening—the testing can triage benign and malignant disease at a fraction of the cost for both the system and the patient. Based on population epidemiology, nearly exact costs for these services can be predicted for a population and stock outs can be avoided. Corollary note: Only for those cancers for which you HAVE a POC.
How would these tests change the approach to breast cancer in an HIC? There would likely be resistance at many levels but, eventually, the relatively low cost and the increased patient value would allow the tests to replace or displace standard diagnostics. Without complete replacement, there could, at a minimum, be multimodality redundancy which increases quality. However, the tests would find purchase within the system because in some settings their cost and added value would make any other choice impossible.
For both settings, we can now add other market entrants, other tests for other cancers, and a generalize increased in cancer awareness in the community, all of which would increase demand, improve morbidity and mortality, but decrease costs. Such a situation would be highly valued by the patients and, therefore, is the most important eventuality as this disruption ensues. Recognizing forthcoming change is sometimes hard and sometimes easy; however, accepting and embracing forthcoming change in healthcare can lead to best outcomes for our patients—the central mission of ASCP.
Dr. Milner has no financial disclosures regarding this blog post and has received no fiscal or in-kind support from any entity, named or otherwise, that involves this blog post.
References
- Wu NC, Wong W, Ho KE, Chu VC, Rizo A, Davenport S, Kelly D, Makar R, Jassem J, Duchnowska R, Biernat W, Radecka B, Fujita T, Klein JL, Stonecypher M, Ohta S, Juhl H, Weidler JM, Bates M, Press MF. Comparison of central laboratory assessments of ER, PR, HER2, and Ki67 by IHC/FISH and the corresponding mRNAs (ESR1, PGR, ERBB2, and MKi67) by RT-qPCR on an automated, broadly deployed diagnostic platform. Breast Cancer Res Treat. 2018 Nov;172(2):327-338.
- Wasserman BE, Carvajal-Hausdorf DE, Ho K, Wong W, Wu N, Chu VC, Lai EW, Weidler JM, Bates M, Neumeister V, Rimm DL. High concordance of a closed-system, RT-qPCR breast cancer assay for HER2 mRNA, compared to clinically determined immunohistochemistry, fluorescence in situ hybridization, and quantitative immunofluorescence. Lab Invest. 2017 Dec;97(12):1521-1526.
- Downs BM, Mercado-Rodriguez C, Cimino-Mathews A, Chen C, Yuan JP, Van Den Berg E, Cope LM, Schmitt F, Tse GM, Ali SZ, Meir-Levi D, Sood R, Li J, Richardson AL, Mosunjac MB, Rizzo M, Tulac S, Kocmond KJ, de Guzman T, Lai EW, Rhees B, Bates M, Wolff AC, Gabrielson E, Harvey SC, Umbricht CB, Visvanathan K, Fackler MJ, Sukumar S. DNA Methylation Markers for Breast Cancer Detection in the Developing World. Clin Cancer Res. 2019 Nov 1;25(21):6357-6367.

-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.