In 1939, the first issue of Marvel Comics introduced the original Human Torch, an android named
Jim Hammond who would burst into flames when exposed to oxygen. Fourteen years
before that, President Calvin Coolidge proclaimed the first National Fire
Prevention Week to commemorate the Chicago fire of 1871 which killed over 300
people 54 years earlier. In that entire span of 68 years, from 1871 to 1939,
over 17,000 people died in fires in the United States. Because of fire
awareness campaigns over the years, the number of home and work place deaths have
greatly decreased, and the risk of fire in your lab goes down when fire safety
awareness increases as well.
In the laboratory, fire safety begins with a look at the
physical environment. It is important to make sure the department is set up to
prevent a fire from starting and to keep one from spreading if a fire ignites.
The electrical wiring in the lab plays a large part in fire safety. Frayed
cords are the number one cause of laboratory fires, and daisy-chained extension
cords or multi-plug adaptors are fire hazards as well. Damaged outlets can also
present danger. Because equipment may move often in the environment, it is a
good idea to check for safety in the lab electrical set up regularly. In audits
I have performed this year alone, I have discovered three damaged electrical
cords just waiting to cause a fire. Things change rapidly in the lab physical
environment, so looking for these potential safety issues is vital.
The next aspect of the lab physical layout that needs
attention is flammable chemical storage. There are complicated regulations
about that, and multiple classes of flammable liquids, but you can simplify
storage rules to make it easy to understand. In general, there should be no
more than one gallon of a flammable liquid out in the lab per every 100 square
feet. If there are automatic sprinklers in the department, that amount can go
up to two gallons. If safety cans are used, the amount can be doubled again.
Any excess volume of flammable liquids should be stored inside of a flammable safety
cabinet with self-closing doors. Remember, the point of these storage limits is
so that if a fire occurs, there is not a large amount of flammable material in
one location. That slows the spread of the fire and allows automatic fire
extinguishing systems to be able to perform their job effectively.
Fire-fighting equipment should be available as well, and
staff are required to have training to use that equipment if it is available in
the department. The best training includes a regular hands-on return
demonstration and periodic fire drills. Making sure staff can use fire
extinguishers and know how to respond to a fire situation may be the one of the
most important safety training policies you can implement. Fire blankets are
typically not required per local fire code, but if they are in place, be sure
staff is aware of how to use them should the need arise.
The last actions in a departmental fire situation include
evacuating and preventing the spread of the fire. To that end, it is important
to keep aisles clear and wide for safe travel, and all exit routes and
stairwells should be checked to make sure no obstructions exist. Staff should
be aware of their primary and secondary evacuation routes, and all exits should
be adequately marked. Make sure employees know to close fire and smoke doors
during a fire situation.
Even in modern times there are structure fires in the work place, and unfortunately, laboratories are not excluded from that list. The Human Torch could catch fire and not get burned, but we all know that is science fiction, and burns from a fire are no joke. The best practice is to be prepared for a fire-provide training, conduct physical environment rounds, and run drills often. That will protect your staff and make you a true safety super hero.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
When a patient gets their “testosterone test” at the doctor to assess their
libido, do they really know what they’re getting? Does your lab test for
testosterone, and are you confused about which of these confusingly-named tests
are in-house versus send-out? Do you need a refresher on the types of
testosterone tests out there and the clinical significance of each?
A Primer on Testosterone
Testosterone, being a fairly hydrophobic member of the steroid-ring family,
is the major androgen in males. Apart from its well-known function in promoting
the development of primary male reproductive organs and secondary male sex
characteristics, it also has important anabolic effects in maintaining muscle
mass, bone maturation, regulation of the hypothalamic-pituitary-adrenal axis
under stress, and even in promoting platelet aggregation through enhancing
platelet thromboxane A2 expression.1 In females, testosterone increases sexual arousal, and is in fact used
clinically as treatment for female sexual arousal disorders. So, clearly an
important member of the steroid family.
Being hydrophobic, much of the testosterone in the human body is not freely
available, but rather bound. Total testosterone signifies the total pool
of testosterone available in the human body, and is largely encompassed by the
majority of bound testosterone with a small (usually 1.5-2.0%)
proportion of free testosterone, which is biologically active. The bound
testosterone can further be subdivided into testosterone bound to sex-hormone
binding globulin (SHBG), a small glycoprotein that strongly binds various
androgens and estrogens, and testosterone bound toalbumin, which is a
relatively weak interaction.
Recently, the concept of bioavailabletestosterone has been
defined,2 based on the understanding that testosterone bound to SHBG (around 2/3rd
of the bound proportion) is relatively inaccessible, while testosterone bound
to albumin is weakly interacting, and thus potentially bioactive. Therefore,
the definition of bioavailable testosteroneincludes both free and
albumin-bound testosterone, which comprise the non-SHBG bound proportion.
How is testosterone measured?
Conventionally, total testosterone is measured through either immunoassays
(both radioimmunoassays, or more commonly, chemiluminescent immunoassays) or
mass spectrometry coupled with gas chromatography (GC/MS) or liquid
chromatography (LC-MS/MS). Isotope dilution mass spectrometry (IDMS) is the
reference method for testosterone measurement,3 but due to cost and convenience, most labs utilize immunoassays. Sex
hormone binding globulin (SHBG) is commonly measured through chemiluminescent
immunoassays, and also available for many platforms.4
There are two main approaches to the measurement of free testosterone,
which is significantly more challenging. The gold standard for free
testosterone measurement is equilibrium dialysis (see inset), a time consuming,
expensive, and laborious assay that uses semi-permeable membranes to measure
antibody-bound fractions of testosterone. Moreover, results can vary with pH,
temperature, and methods of dilution.5 Due to these complications, calculated free testosterone is an attractive
alternative used by many laboratories.
What is equilibrium
dialysis?
Equilibrium dialysis and ultrafiltration are reference methods used to
determine true free testosterone calculation. Briefly, a relatively large
quantity of serum (500 to 1000 uL) is placed in one chamber of an equilibrium
dialysis apparatus, which is comprised of two fluid chambers separated by a
semi-permeable membrane. Free-labeled testosterone passes through the
membrane, while testosterone bound to SHBG does not. The radioactivity in the
free chamber is quantified as a proportion of the total testosterone level,
as measured by another assay, such as LC/MS-MS.
What is calculated free testosterone, and how is it calculated?
Recognizing the difficulty of performing equilibrium dialysis on large volumes of testosterone specimens, several researchers have looked into devising good approximations of free testosterone through mathematical expressions modeling the distribution of testosterone among its various compartments. One of the most popular approximations, the Vermeulen equation developed by Dr. Alex Vermeulen,6 models the distribution of testosterone among the SHBG-bound, albumin-bound, and free component through association constants of testosterone among these compartments, and can be modeled by the equation in Figure 1, which depends on the total testosterone, SHBG concentration, and concentration of albumin (although this will be discussed below). The overall concordance of this method with apparent free testosterone obtained through equilibrium dialysis (AFTC), the reference method, is very good, with a correlation coefficient of 0.987 and mean values well within the SEM between the two methods.6
Figure 1. The Vermeulen equation for calculated free testosterone.
In studies of the variation of calculated free testosterone values to the
albumin concentration, Vermeulen et al. demonstrated that between “normal”
albumin concentrations ranging from 5.8–7.2 × 10−4 mol/L (40
to 50 g/L), the mean calculated free testosterone varied from 340 ± 40.9 pmol/L
assuming an albumin concentration of 40 g/L, to 303 ± 35.4 pmol/L assuming a
concentration of 50 g/L albumin. Moreover, the concordance of calculated FT
results to AFTC concentrations remained very good (correlation coefficient of
0.992) when an intermediate fixed albumin concentration (43 g/L) was used in
this calculation, compared to actual albumin levels. Overall, these
calculations suggest that for healthy individuals without marked abnormalities
in plasma protein composition, such as in nephrotic syndrome or cirrhosis of
the liver, or pregnant patients, a fixed albumin concentration could be used
without significantly affecting calculated FT results. Of course, in
individuals with marked changes in plasma proteins, the actual albumin
concentration should be accounted for.
Willem de Ronde et al5 compared five different algorithms for calculating free or
bioavailable, which includes the Vermeulen and Sodergard method (which use
similar parameters), as well as methods by Emadi-Konjin et al, Morris et
al, and Ly et al. In general, there was high concordance between the Vermeulen
and Sodergard methods (r=0.98) for measuring free testosterone, and lower, but
still reasonable (r=0.88) concordance between Vermeulen and other methods.
Fundamentally, the Vermeulen and Sodergard equations were derived from
experimentally derived association constants from the law of mass action, as
opposed to the other algorithms, which rely on experimentally derived free and
bioavailable testosterone measurements that was modeled by regression
equations, and thus depends on the accuracy of these measurements. Though the
experimental basis underlying the Vermeulen and Sodergard equations is
stronger, it is known that supraphysiologic concentrations of other steroid
hormones (estradiol or dihydrotestosterone), in competition for binding
sites to SHBG, can significantly underestimate free testosterone by any
of these methods. Of course, inaccuracies in the measurement of total
testosterone or SHBG can significantly affect results, as well as significant
perturbations in total serum protein concentrations (as mentioned above).
Since the publication of the above work, additional
calculations for free testosterone accounting for other modes of interaction of
SHBG such as allostery and dimerization have been published that may further
improve concordance with AFTC;7,8 however, further study is
needed to determine if these methods actually result in superior calculated FT
measurement for clinical decision making, as well as changes in sensitivity to
interference.
Why do accurate free testosterone measurements matter?
Testosterone bound to serum albumin is essentially inactive; therefore, the
only testosterone that is biologically relevant is free (and to a lesser
extent, bound to SHBG). Current consensus guidelines still support the use of
total testosterone for defining hypogonadism in men,9,10 although emerging studies and newer task-force consensus groups11,12 highlight an emerging role for both calculated and free testosterone
measurements in addition to total testosterone. The role of direct free
testosterone measurement is still hotly debated; a recent analysis of CAP
proficiency data indicates considerable heterogeneity among laboratories using
the reference methods described above, and suggests considerable cost savings
without significant loss of reliability can be achieved by using calculated or
FT bioavailable T over direct FT measurement.13 Further standardization of these assays is needed to better understand the
tradeoffs here.
References
Ajayi A a. L, Halushka PV. Castration reduces platelet thromboxane A2
receptor density and aggregability. QJM. 2005;98(5):349-356.
doi:10.1093/qjmed/hci054
Shea JL, Wong P-Y,
Chen Y. Free testosterone: clinical utility and important analytical aspects of
measurement. Adv Clin Chem. 2014;63:59-84.
Botelho JC,
Shacklady C, Cooper HC, et al. Isotope-Dilution Liquid Chromatography–Tandem
Mass Spectrometry Candidate Reference Method for Total Testosterone in Human
Serum. Clinical Chemistry. 2013;59(2):372-380.
doi:10.1373/clinchem.2012.190934
Dittadi R, Fabricio
ASC, Michilin S, Gion M. Evaluation of a sex hormone-binding globulin automated
chemiluminescent assay. Scand J Clin Lab Invest. 2013;73(6):480-484.
doi:10.3109/00365513.2013.805807
Ronde W de, Schouw
YT van der, Pols HAP, et al. Calculation of Bioavailable and Free Testosterone
in Men: A Comparison of 5 Published Algorithms. Clinical Chemistry.
2006;52(9):1777-1784. doi:10.1373/clinchem.2005.063354
Vermeulen A,
Verdonck L, Kaufman JM. A Critical Evaluation of Simple Methods for the
Estimation of Free Testosterone in Serum. None. 1999;84(10):3666-3672.
doi:10.1210/jcem.84.10.6079
Heinrich-Balard L,
Zeinyeh W, Déchaud H, et al. Inverse relationship between hSHBG affinity for
testosterone and hSHBG concentration revealed by surface plasmon resonance. Molecular
and Cellular Endocrinology. 2015;399:201-207. doi:10.1016/j.mce.2014.10.002
Zakharov MN, Bhasin
S, Travison TG, et al. A multi-step, dynamic allosteric model of testosterone’s
binding to sex hormone binding globulin. Mol Cell Endocrinol.
2015;399:190-200. doi:10.1016/j.mce.2014.09.001
Margo KL, Winn R.
Testosterone Treatments: Why, When, and How? AFP. 2006;73(9):1591-1598.
American
Association of Clinical Endocrinologists Medical Guidelines for Clinical
Practice for the Evaluation and Treatment of Hypogonadism in Adult Male Patients—2002
Update. Endocrine Practice. 2002;8(6):439-456. doi:10.4158/EP.8.6.439
Bhasin S,
Cunningham GR, Hayes FJ, et al. Testosterone therapy in men with androgen
deficiency syndromes: an Endocrine Society clinical practice guideline. J
Clin Endocrinol Metab. 2010;95(6):2536-2559. doi:10.1210/jc.2009-2354
Liu Z, Liu J, Shi
X, et al. Comparing calculated free testosterone with total testosterone for
screening and diagnosing late-onset hypogonadism in aged males: A
cross-sectional study. J Clin Lab Anal. 2017;31(5).
doi:10.1002/jcla.22073
Morales A, Collier
CP, Clark AF. A critical appraisal of accuracy and cost of laboratory
methodologies for the diagnosis of hypogonadism: the role of free testosterone assays. Can
J Urol. 2012;19(3):6314-6318.
-Dr. Jim Hsu is a 2nd year pathology resident currently in training at Houston Methodist Hospital. After completing a M.D./Ph.D at the University of Texas Medical Branch in Galveston, he realized his passions remained in the lab, but wanted to bring that passion into patient care, and soon realized that pathology was the key to achieving both. His love for all things data drew him to pathology informatics, and with the suggestion of his mentor Dr. Wesley Long, to API. In particular, he is interested in the transformative power of data analysis in improving best practices, reducing error, and combating bias. Outside of the lab, he is interested in financial markets, algorithms, neuroscience, reading, and traveling (for the food, of course).
I first started in my
current lab back in 2008. At that time, we did not have a separate section for
testing solid tumors in our lab. The small amount of testing we did have were
for three different types of sarcomas, and we still used a thermal cycler that
didn’t have a heated lid, so we had to put mineral oil over the top of the
reactions…
Fast forward eleven
years and we now have a “bench” dedicated to solid tumor testing with next
generation sequencing as a major part of this testing. We have been running our
current solid tumor assay, a hotspot panel of fifty genes, for almost five years
now and it has served us well. However, many of our oncologists have been
starting to ask for more. We have begun the search for a larger panel to
fulfill the needs of our oncologists and our patient population. As a smaller
lab, we are somewhat limited in resources and are not quite ready to go
completely custom, so we are left with kitted options from major vendors. As we
research and evaluate these options, though, certain questions come to light. These
panels have more than 150 genes and upwards of 500 genes in order to cover the
most relevant genes in a number of different cancers. The areas tested in these
genes are important for therapy and/or prognosis, but with the sheer number of
bases we are looking at, we are bound to find many variants that do not have a
known significance.
So, question one, how
do the pathologists deal with trying to interpret the large number of variants
of unknown significance (VUS’s)? Currently, with our very limited 50 gene
panel, we may get one or two VUS’s, so it doesn’t take much time to assign
significance and sign out the report. Our myeloid panel, which is a larger
panel of 40 genes, some with full gene coverage, though, can sometimes result
in reports with eight to ten VUS’s. These reports take a lot of time to
research the potential impact each of these variants will have in the disease. I
have seen reports from some of these large gene panels that have upwards of 25
or more VUS’s detected in a single specimen. How are these handled in the pathologists’
workflow? Can time be taken to investigate each of these, or are they just
placed in a list in the report?
Question two, how do
the oncologists feel when they receive a report with few, if any, variants with
known significance, and many variants with unknown significance? Does this help
at all, or make it more difficult and frustrating? I’d be interested if anyone
has feedback in this area. In our internal tumor boards, when we review testing
done at other locations, a great deal of time is spent trying to filter through
the results to see how they can help point to the best possible treatment for
the patient. If the variants do not point to therapy or clinical trials, those
variants are not currently helpful.
Lastly, if and when we bring up a larger panel, do we keep running our smaller 50 gene panel? We believe the answer to this one is easy – yes. The amount of DNA needed for some of these larger panels is more than what we can get sometimes from the smaller biopsies. Also, insurance may not always cover the larger panels. The information we get from the 50 gene panel is still very useful and can point the oncologists to therapy options, as well as clinical trials, so we believe the smaller panel will still have a place in our lab.
-Sharleen Rapp, BS, MB (ASCP)CM is a Molecular Diagnostics Coordinator in the Molecular Diagnostics Laboratory at Nebraska Medicine.
An 80 year old man presented with rapid onset of cervical adenopathy over a period of few months. The largest lymph node measuring 6 cm was biopsied and sent for histopathological evaluation.
Biopsy Findings
Sections
from the lymph node showed effacement of the lymph node architecture by a
fairly monotonous population of medium to large sized lymphoid cells arranged
in vague nodular pattern. Focally, a starry sky pattern was observed. The cells
were 1.5-2 times the size of an RBC, with high N:C ratio, irregular angulated
nuclei and small nucleoli. A high mitotic rate of 2-3 mitoses/hpf was seen.
Immunohistochemistry
Immunohistochemical
stains showed that the lymphoma cells were positive for CD20, CD5, SOX-11, and
negative for Cyclin D1, CD10, CD23, CD30, BCL-1, and BCL-6. Ki67 index was
about 70%.
Diagnosis
A diagnosis
of Mantle cell lymphoma, pleomorphic variant was made.
Discussion
Mantle cell
lymphoma is a peripheral B cell lymphoma, occurring in middle aged or older
adults, with a male: female ratio of 7:1. Although Cyclin D1 expression is
considered a hallmark of mantle cell lymphoma, yet about 7% cases are known to
be Cyclin D1 negative. In these cases, morphological features and SOX-11
positivity helps in establishing a definitive diagnosis.
Differential
Diagnosis
In the
assessment of morphological features of lymphoma, the cell size is an important
starting point. In this case, the lymphoma cells ranged from medium to large
sized. The following differential diagnoses were considered:
Burkitt lymphoma
This case showed a “starry sky” pattern focally. A medium sized
population of cells, high mitotic rate and a high Ki67 index (70%) favoured a
Burkitt lymphoma. However, although commonly seen in Burkitt lymphoma, a
“starry sky” pattern is not specific for this type of lymphoma. Also, the lack
of typical “squaring off” of nuclei, basophilic cytoplasmic rim were against
the diagnosis of Burkitt lymphoma. The nuclei in this case showed 0-1 small
nucleoli, unlike the typical basophilic 2-3 prominent nucleoli of Burkitt
lymphoma. Moreover, Ki67 index, even though high was not enough for Burkitt
lymphoma where it approaches 100%. The cells were negative for CD10 and Bcl-6, which
are almost always found in a Burkitt lymphoma. Hence, a diagnosis of Burkitt
lymphoma was ruled out.
Diffuse Large B cell Lymphoma
The presence of interspersed large cells with nucleoli, irregular
nuclei, high mitotic rate, and a high Ki67 index with a history of very rapid
enlargement of lymph node suggested a diagnosis of Diffuse Large B cell
lymphoma. However, the scant cytoplasm, lack of bizarre cells, and absence of
CD10, BCl-2, BCl-6 were against a diagnosis of DLBCL.
Lymphoblastic lymphoma
A diagnosis of lymphoblastic lymphoma was favoured by the irregularly
angulated nuclei, and presence of nucleoli. However, the cells of lymphoblastic
lymphoma have a more delicate nuclear chromatin, higher mitotic rate as against
the relatively condensed chromatin and the low to high variable mitotic rate of
Mantle cell lymphoma. Also, lymphoblastic lymphomas are more commonly of the T
cell subtype and occur commonly in younger individuals. In this case, B cell
markers were positive (CD 20), and the patient was 80 year old, disfavouring a
lymphoblastic lymphoma. The blastoid variant of mantle cell lymphoma is
practically indistinguishable from lymphoblastic lymphoma, except that it is
Tdt negative.
Cyclin
D1 negativity in Mantle cell lymphoma
In the
cases of Cyclin D1 negative mantle cell lymphomas, morphology plays a critical
role in coming to a diagnosis of mantle cell lymphomas. In this case, points
that favoured the diagnosis of mantle cell lymphoma were clinical features such
as older age (80 years), and male gender, and morphological features such as a
vaguely nodular pattern of growth, irregular nuclei, and 0-1 small nucleoli.
Due to the presence of variably sized cells with distinct nucleoli, a
pleomorphic variant was considered. Even though Cyclin D1 was found to be
negative, the cells were positive for SOX-11.
SOX-11 is a
transcription factor that is not normally expressed in B cells, but is
sensitive and fairly specific for mantle cell lymphomas. It is important to
note that SOX-11 is also positive in 25% Burkitt lymphoma, 100% lymphoblastic
lymphoma, and 66% T-prolymphocytic leukemia. Herein lies the importance of
recognising morphological features, as all of these lymphomas that may express
SOX-11 were ruled on the basis of morphology. A more specific antibody, MRQ-58
may be used for greater specificity. The presence of SOX-11 is considered a
specific biomarker for Cyclin-D1 negative mantle cell lymphomas. In these
cases, there is upregulation of Cyclin D2 or D3 that may substitute for Cyclin
D1 upregulation. But, immunohistochemical detection of Cyclin D2 or D3 is not
helpful for establishing a diagnosis, as other lymphomas are commonly positive
for these markers. Hence, it is important to perform SOX-11
immunohistochemistry to diagnose the Cyclin D1 negative variant of mantle cell
lymphoma.
SOX-11 can
be used not just for the diagnosis, but also for determining prognosis of
mantle cell lymphoma. Indolent MCL usually lack SOX-11 expression. The pattern
of SOX-11 staining has also been used a marker of prognosis. Cytoplasmic
expression of MCl, seen in only a few cases was associated with a shorter
survival as compared to the more common nuclear staining of SOX-11.
Conclusion
In this
age, lymphoma diagnosis relies heavily on the use of immunohistochemical
markers. However, this case highlights the importance of morphological features
in diagnosing lymphomas with unusual immunohistochemical marker profile.
Although, this case was negative for Cyclin D1, considered a hallmark of Mantle
cell lymphoma, yet, the combination of morphological features with SOX-11
staining helped in clinching the diagnosis. To avoid a misdiagnosis, it would
be prudent to perform SOX-11 staining in all lymphoma cases morphologically
resembling MCL, but lacking Cyclin-D1.
-Swati Bhardwaj, MD has a special interest in surgical pathology and hematopathology. Follow her on Twitter at @Bhardwaj_swat.
–Kamran M. Mirza, MD, PhD, MLS(ASCP)CM is an Assistant Professor of Pathology and Laboratory Medicine, Medical Education and Applied Health Sciences at Loyola University Chicago Stritch School of Medicine and Parkinson School for Health Sciences and Public Health. A past top 5 honoree in ASCP’s Forty Under 40, Dr. Mirza was named to The Pathologist’s Power List of 2018 and placed #5 in the #PathPower List 2019. Follow him on twitter @kmirza.
The patient is a 70 year old male who was diagnosed with Kappa free light chain multiple myeloma. He was initially seen after he had a fall in the woods and underwent imaging which showed multiple lytic lesions and blood work showing monoclonal proteins and thrombocytopenia. He was found to have a lesion on his right scapula for which he received radiation. Bone marrow biopsy was performed which showed 60% plasma cells. To date he has completed radiation therapy, 5 cycles of chemotherapy, and is in the process of collecting stem cells for autologous stem cell transplant. Routine fungal culture of the stem cell collection grew a single tan white dry appearing colony on potato flake agar. A Gram stain of the organism revealed gram positive cocci mixed with filamentous structures.
Laboratory Identification
Image 1. Single tan white dry colony on potato flake agar. Image 2. Modified acid fast stain (left) and Gram stain (right). Image 3. Filamentous branching on Gram stain.
Based on the colony morphology and Gram stain results the
organism was suspected to be in the Streptomyces
genus. Identification with MALDI-TOF was attempted and did not yield a result
as this bacteria is not in the data base.
Discussion
Streptomyces is a genus of gram positive aerobic saprophytic bacteria that grows in various environments, and has a filamentous form similar to fungi (1). The morphologic differentiation of Streptomyces involves identification of complex multicellular architecture with germinating spores that form hyphae, and multinuclear aerial mycelium, which forms septa at regular intervals, creating a chain of uninucleated spores (2,3). They are able to metabolize many different compounds including sugars, alcohols, amino acids, and aromatic compounds by producing extracellular hydrolytic enzymes (helping with degradation of organic matter). Their metabolic diversity is due to their extremely large genome which has hundreds of transcription factors that control gene expression, allowing them to respond to specific needs (3).
Streptomyces is also considered to be one of the most
medically important bacteria because of its ability to produce bioactive
secondary metabolites. These metabolites are used in the creation of
antifungals, antivirals, antitumoral, anti-hypertensives, and many antibiotics
and immunosuppressives. They are responsible for 2/3 of all the worlds
naturally occurring antibiotics (1).
Streptomyces is usually
considered a laboratory contaminant though they can cause infections in
immunocompromised patients and are chiefly responsible for granulomatous
lesions in skin also known as actinomycotic mycetomas (1,2). Invasive pulmonary
disease has been seen in HIV patients, splenectomized patients with sarcoid,
and rarely in immunocompetent hosts (1). More rare presentations include brain
abscesses can be seen in patients with cerebral trauma, peritoneal infections
have been shown to occur in patients undergoing multiple pericenteses, and
bacteremia in patients with indwelling catheters (1). Infection with Streptomyces is not common so
susceptibility data is limited. Available data shows that organisms were
consistently susceptible to amikacin; frequently susceptible to imipenem,
clarithromycin or erythromycin, minocycline, and trimethoprim-sulfamethoxazole;
and infrequently susceptible to ciprofloxacin and ampicillin (4).
Our patient had not received the stem cell unit that this
grew from, so another aliquot was requested. The second aliquot did not grow
any organisms, so the Streptomyces
was considered a contaminant.
References
Procop, Gary W., et al. Konemans Color Atlas
and Textbook of Diagnostic Microbiology. 7th ed., Wolters Kluwer Health,
2017.
Chater KF. Recent advances in understanding Streptomyces.
F1000Res. 2016;5:2795. Published 2016 Nov 30.
doi:10.12688/f1000research.9534.1
Mona Kapadia, Kenneth V.I. Rolston, Xiang Y.
Han, Invasive Streptomyces Infections: Six Cases
and Literature Review, American Journal of Clinical
Pathology, Volume 127, Issue 4, April 2007, Pages 619–624, https://doi.org/10.1309/QJEBXP0BCGR54L15
-Casey Rankins, DO, is
a 3rd year Anatomic and Clinical Pathology resident at the
University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
Julie SG. Papango, MLS(ASCPi)CM is a medical
technologist currently working in Albany Medical Center in Albany, NY. She was
born and raised in the Philippines, where she trained as a medical technologist.
I had the pleasure of talking with Julie recently as I had read about her
extensive work in global health through Doctors Without Borders which was
highlighted by ASCP when they designated her as a Top 5 honoree of the
prestigious 40
under Forty recognition program in 2019.
I was impressed by the extent of her work before talking
with her, but after digging in and hearing the details, I was entirely blown
away and fell nearly speechless. Julie is truly the bravest person I have ever
met. She has spent years of her life serving in some of the world’s most
difficult places and has done so seeking no reward. One can only imagine the
kind of daily challenges that would arise working in these conditions. Not only
that, but Julie has done all of this while transitioning as a person of
transgender experience. Knowing that in some countries this has been met by
death, Julie chose to serve those in desperate need anyway. Take a moment to
really digest that. Her bravery and dedication to humanity goes beyond anything
most of us will ever hope to parallel.
I hope you enjoy reading about her contributions to the
world and are left inspired to make your own contributions too!
Q: What made you interested in global health and how did
you have the idea to work with Doctors Without Borders?
A: After graduating as a medical technologist in
2003, I had a very vague idea about working in global health inspired by what I
had seen portrayed in movies. My ideas were almost romantic as I pictured
myself working with people in need. I heard of Doctors Without Borders around
2005 and thought this might be a good avenue to work through. The idea became
more solidified in mid-2007 when I heard a former colleague of mine speak about
his experiences working with them around the world. I was so inspired by his
impact and realized that I could make my dream a reality. I immediately applied
and went through their lengthy interview process and was accepted in December
2007. Although I was matched to a project early the next year, I was not able
to go as I stayed back to take care of my mother who had become very ill at the
same time. Once she became stable, I re-volunteered and went through the
process again and finally started out in my first project in 2009.
Q: Can you tell me about your time working with Doctors
Without Borders?
A: The first project I was matched to was in the Kampong
Cham province in Cambodia. I spent one year and two months there to help the
Ministry of Health improve their tuberculosis detection program and set up a
lab for diagnosis with bacterial liquid culture. This was challenging because
there were no public laboratories performing these tests at the time and we
started from scratch. I worked to train the local workforce to function as medical
technologists and to take over and expand the project. At the time, it was
challenging for Doctors Without Borders to fulfill their mission to improve the
laboratory services because there are not a lot of medical laboratory
technicians working as volunteers. Many laboratory members just don’t realize
there is a real need and opportunity to work in this capacity. I was originally
supposed to stay only for six months but extended my stay because they weren’t
able to find a replacement for me for another eight months.
After this, I returned home for a short time when I was then
contacted to work in a town called Arua in Uganda in 2010. Admittedly, I was
scared to go to Uganda because there had been open hostility towards the LGBT
community there, and an activist of homosexual orientation had been killed in
his own home there recently. I am a person of transgender experience so this
was frightening for me. But I decided to push forward because there was an
increasing incidence of HIV/AIDS and the laboratories that were in existence
needed serious quality improvement to properly perform testing. For six months,
I served as a laboratory supervisor and worked to bring the testing standards
up to par.
My next time working with Doctors Without Borders was in
October of 2012 when I spent six months working in an extremely remote setting
of Papua New Guinea. I spent my time there on the island of Bougainville which
hosted only 6 non-native persons in the entire town of Buin where I worked. Transportation
across the island was a full twelve-hour trip, which meant crossing numerous
rivers and very rough roads. The project focused on maternal and child health,
and I was there to help improve the laboratory which was manned by just one
technician, who had received the entirety of his training on-the-job without a
formal degree. When I arrived, the lab looked like nothing more than a stock
room. I spent two weeks alone just cleaning! Eventually, we were able to set up
a basic functioning laboratory offering rapid testing for HIV, HCV, syphilis, as
well as microscopy, blood counts, and basic transfusion services.
After this, in August of 2013, I was recruited to work in
South Sudan for an emergency project. Sudan had split into two countries in
2011 and there was conflict in the Nuba mountain border area over oil land
ownership. This created a refugee crisis which resulted in 60,000 refugees rapidly
fleeing the area and were forced to live in camps. There were major issues with
child mortality due to malnutrition, cholera, meningitis, and malaria. Doctors
Without Borders was in the camp and set up a tent that served as part hospital,
part living quarters for us working there. The living quarter capacity was
meant for just 6 people as there was already a team there, but out of necessity
was shared among 30. This situation was challenging, as food and water were
very limited – for a camp population of this size, there were only three water
points in the entire makeshift facility. Working in this setting is known among
the volunteers as the “true litmus test” due to its extreme challenges. My role
there was to set up the tent in which we would run the laboratory, help train
local staff, and to set up the point of care and basic blood testing for
transfusion services. With a break in between, I spent a total of almost two
months in the camp working on this project before returning home for a month or
two. After this, I returned to work again in South Sudan because there was a need
to verify the accuracy and quality of the testing that was being performed in
the refugee camp. There were many issues with transporting the specimens to
referral labs, and we wanted to analyze if these samples were being handled
appropriately to yield reliable results. This is one of the frustrating things
about working in these situations, nothing is done perfectly, and you have to
find a way to make it work. I was scheduled to work there for four months but
after month three, all non-essential Doctors Without Borders staff had to be
evacuated out due to a civil war that broke out and made the region too
dangerous.
I was then supposed to go to Ethiopia to spend a month
working on a primary care health project. I was delayed because of a visa issue
pertaining to the fact that I was transgender. The difference between how I
appeared on the outside as female and what my passport showed as male was an
issue. Eventually, after returning to the embassy every day for a week, I was
denied a visa. I was given an invalid reason and I knew that this was just a
power-play and was really due to the fact that I was of transgender experience.
Eventually, after more paperwork and delay, I made it through the process and
worked in Ethiopia for a month to perform a quality analysis on the basic
laboratory testing and ensure an adequate chain of supplies that had been
initiated by Doctors Without Borders before passing it on to the Ministry of
Health. Being there for only a month was frustrating because there were still
more gaps to fill, and there was only so much I could do. This is just the
reality of the situation and you have to accept that it is not always perfect.
After settling in back home in the Philippines for a short
time, I felt that I wanted to return to Cambodia to continue the work that I
had started there. So, in March of 2013, I went back to work in the laboratory
that I had helped start. This time the laboratory had expanded to other sites
where more advanced tuberculosis testing was being done and the government was
increasing the support for the labs. I worked in quality improvement and helped
to create a network for transporting specimens to larger referral laboratories.
At the end of my stay in November 2015, we were able to finish the project,
donate all of the equipment that had been provided by Doctors Without Borders,
and hand the reigns over to the Ministry of Health. I decided at this time that
I would look to stay in the country and worked as a private citizen in a
developmental aid project, which was aimed to improve the country’s diagnostic
microbiology services. There I found the organization called Diagnostic
Microbiology Development Program. This was an interesting shift from the humanitarian
aid work that I had done with Doctors Without Borders since it focused more on
sustainability rather than immediate intervention in a crisis.
Q: What brought you to the US?
A: Over the years of volunteering abroad, I have had
countless challenges when I am crossing a border and the fact that my external
appearance of a woman does not match the gender marker that is designated on my
passport. I decided that it had come time to go through the process of
rectifying this situation and so I applied for a visa to work in the US with
the eventual goal to change my gender marker on my passport. I moved to the US
in 2016 and have been working as medical technologist in Albany since.
Q: I know that working in global health can sometimes be
equally as challenging as it is rewarding, and you have certainly faced your
fair share of challenges. What would you say to those wondering if they have
what it takes to contribute?
A: I encourage people to go out of their comfort
zones and look at what you can give, and just give it. It can be scary, but we
have a responsibility to the global world to share what we are privileged to
have. For me, being a person of transgender experience, labels are assigned to
me that this is not the “right type” of work for me, that I might be more
suited for the fashion and beauty industry for instance. This is like any
stereotype that puts people in boxes based off race, gender, religion, or
sexual orientation. This box should not be the reality, and at the end of the day,
we must realize that we are not boxes and we are all just human beyond labels.
I encourage everyone to break the glass ceiling, get out of their comfort zones
and look for ways to share what you have with the world.
-Dana Razzano, MD is a former Chief Resident in her fourth year in anatomic and clinical pathology at New York Medical College at Westchester Medical Center and will be starting her fellowship in Cytopathology at Yale University in 2020. She is passionate about global health and bringing pathology and laboratory medicine services to low and middle income countries. She was a top 5 honoree in ASCP’s Forty Under 40 in 2018 and was named to The Pathologist’s Power List of 2018 and 2019. Follow Dr. Razzano on twitter @Dr_DR_Cells.
I’m writing to you now back in Manhattan after visiting
sunny Phoenix, AZ for this year’s ASCP Annual Meeting. Last month
I talked about downtime, pathology emergencies, and introduced you all to our
insightful and dynamic colleague, Jalissa Hall. It was great working with her
and one of the last things we talked about was getting to go to professional
society meetings. We also talked about the upcoming meeting next year in
Austin, TX! And that’s exactly what I’d like to talk about with you this time:
why going to meetings like ASCP is not only educational, but an excellent way
to network with your laboratorian peers from around the country.
Image 1a. My wife and I made it to the Phoenix Hyatt Regency on registration day! ASCP swag on, obviously.Image 1b. Behind the Scenes – Hosting the ASCP 2019 Facebook Live broadcast with two fantastic colleagues, Dr. K. Mirza and Dr. A. Booth! Did you catch us? But more about social media later…
I couldn’t go to every single session—there’s just too
many—but I did learn so much valuable, practical information at the educational
sessions. Here are just a mere few insights from the long list of fantastic
speakers I had the chance to visit!
I participated in an interactive session on the
ASCP/CAP/ASH guidelines for lymphoma workup…
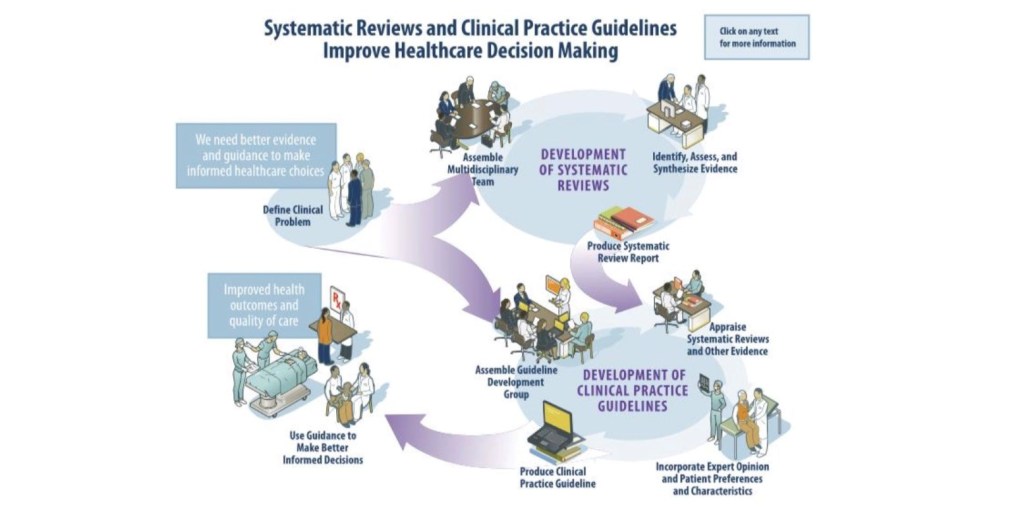
Figure 1. All the multidisciplinary expertise must go through rigorous adjustment and evaluation all the way throughout the process of seeking out and publishing proper guidelines. (Source: ASCP 2019 session 5007-19; Kroft, S., Sever, C., and Cheung, M.)
Drs. Kroft, Sever, and Cheung discussed updates from the WHO
2016 guidelines as well as relating any changes in concurrent literature to
appropriate diagnostic accuracy with evidence-based guidelines. If it sounds
familiar, it’s because I talked about these guidelines a
few months ago! In my month clerkship at The Mayo Clinic in Rochester, MN I
presented a therapy-related AML case in the setting of Li-Fraumeni disorder. In
my discussion I stressed the utility and importance of having organized and
algorithmic guidelines to diagnose patients accurately, effectively, and
timely. This time, instead of just talking about the guidelines, I got to
listen to some of the folks who actually put them together—and,
according to them, it’s no easy task!
I learned about culturally appropriate leadership
training…
Figure 2. The panelists each had something insightful and moving to contribute to this wonderful discussion on female empowerment in our profession, and ultimately how it relates to improving patient care! (Source: ASCP 2019 session 8012-19; Mulder, L., Upton, M., Vuhahula, E., Abedl AlThagafi, M., Papas, F., and Sanford, K.)
This year’s ASCP president, Dr. Melissa Upton moderated this
fantastic panel and opened with an old proverb: “If you want to go fast, go
alone. If you want to go far, go together.” This was definitely a theme for
each of the mini-sessions’ discussions. ASCP’s own Lotte Mulder discussed her
research on culturally applicable leadership training using her Leadership
Institute Initiative. She talked about countries that are culturally different
and developmentally different up and down the spectrum can all benefit from
leadership development and opportunity. Next came Dr. Edda Vuhahula, an
accomplished physician, educator, and advocate in Tanzania. She related her
experiences of women in leadership roles, and challenges on the horizon as more
women rise to these positions every day. Dr. Malak Abed AlThagafi talked about
her “hats:” as an entrepreneur, a medical director, and a researcher in her
whirlwind story of empowerment and accomplishment. Finally, medical laboratory
scientist and former Philippine Army colonel, Filipinas Papas gave her personal
perspectives on sexism, education, bias, and opportunity.
Celebrated my colleagues and my contributions to the 6thChoosing Wisely list of recommendations…
Figure 3. My totally biased favorite slide from Dr. Lee H. Hilbourne, chair of the ASCP Effective Test Utilization Steering Committee. It’s an honor to be included in this year’s list, alongside so many accomplished contributors.
The Choosing Wisely initiative, partnering with the
American Board of Internal Medicine and many other specialty organizations, is
one of my favorite programs at ASCP. To date, our lab medicine organization has
the highest number of effective test utilization recommendations. ASCP seeks
active contributions to our expanding lists of recommendations to eliminate
wasteful, unnecessary testing and to improve patient outcomes. This talk was
also a great opportunity to honor the ASCP 2019 Choosing Wisely
Champions: Dr. Gary W. Procop from the Cleveland Clinic, Dr. Lucy Nam from the
Inova Lab best practice team, and Dr. Alyssa Ziman from UCLA Health. Want to read
the most updated list of recommendations ASCP made to the Choosing Wisely initiative?
I watched some cutting-edge exchanges about cellular
therapy…
Image 2. Here I am with laboratorian S. Malakian and Dr. Gastineau with The Mayo Clinic after they discussed the future of complex cell therapies.
One really effective take-home message from this seminar was
that, if we’re going to rely on cellular therapy in the future—especially as it
relates to “individualized medicine”—then who do you think should be in charge?
Who’s got the most experience and knowledge when it comes to cell storage,
transfusion protocol, patient outcomes, and high reliability? Short answer:
it’s us. Long answer: go back and check out a piece
I wrote about high-stakes responsibility in and out of the lab!
Popped into fascinating hematologic cases at our
neighboring SHEAHP2019 meeting…
Listen, I like hematopathology, I’ll be the first to tell
you that. There were so many people giving presentations in this near
standing-room-only meeting, that I recognized from papers, abstracts, and
journals that I’ve read in the past year alone! There were so many interesting
sessions at this meeting, I wish I could have seen more…
Image 3. Here’s Dr. J. Dalland from Mayo Clinic Pathology discussing a lymphoproliferative disorder with associated eosinophilia. These talks go deep into morphology and photypic patterns, so that Hemepath colleagues have a chance to assess their workup and protocols. It’s also great learning for avoiding pitfalls—this case shows architectural changes in lymph nodes which could cause someone to misdiagnose!
Learned how to create an impactful dialogue with patients
directly…
What do you do as a pathologist when a patient wants to
speak to you? Yes, you. Not a typo! This was the last talk I went to and it was
a great way to close out this awesome conference.
Image 4. Me with (left to right) Dr. K. Sanford from VCU, Patient Champion Anthony Reed, Dr. M. Sitorius from the University of Nebraska, and M. Mitchell. All of these individuals had amazing things to say about bridging the gap between the bench and the bedside!
In their own ways these patient advocates demonstrated that
if you want to represent our lab profession as one of accuracy, answers, and
hope, we’ve got the skills and resources to do it! Dr. Sanford sees so many
patients in her transfusion services and discusses their care plans regularly.
Mr. Reed is an ASCP patient champion who, after being diagnosed with ESRD,
became a learned lab ally. Dr. Sitorius is a family medicine physician at a
pathology conference, talking about empathy and connection! Ms. Mitchell has
done fantastic work with her pathology colleagues after beating cancer and
fighting for patient education every day! These folks have taken our field of
laboratory medicine to its outer edges, touching patients’ lives directly—and I
left energized to take it further in the future.
And of course, I learned so much about the utilization of
social media as a practical tool for education, advocacy, and outreach…
I can’t list every single session, lecture, keynote,
presentation, or panel in this article. This was just a glimpse of what
meetings like this have to offer. You will learn, obviously, but you’ll also
gain access to new perspectives and meet people who reinvigorate your passion
for your profession in ways you didn’t even consider. One of the most
fulfilling experiences of this meeting was being on the ASCP Social Media Team!
Posting to Instagram, Facebook, and Twitter with the hashtags #ASCP2019,
#ASCPSoMeTeam, or the scavenger hunt #ASCPiSpy was a great way to bolster our
enthusiastic network. This was my third ASCP Annual Meeting, and I met so many
wonderful people I can’t wait for the next one! Here’s a few of my favorite
snaps from the meeting:
Image 5. Here’s part of our amazing #SocialMediaTeam: (left to right) A. Odegard from Baptist Health, myself, Dr. S. Mukhopadhyay from the Cleveland Clinic, Dr. A. Booth from the University of Texas, and Dr. K. Mirza from Loyola Chicago!Image 6. At my first ASCP meeting in California, Jeff Jacobs, ASCP’s Chief Science Officer, gave me some of the best advice for my own personal and professional growth, “Stay Humble” he told me. Nearly 5 years later, he added “Don’t Give Up” on goals, yourself, or anything in life. You can’t pick that up in a path review book. I feel lucky to know people like him.Image 7. #SoMe FTW (Social Media for the win!) At this great talk, Dr. C. Arnold, Dr. L. Shirley, and Dr. D. Gray III, all from the Ohio State University discussed how to use social media to build a reputation and expand your impact as a pathologist, educator, and advocate!Image 8: Conferences are a great time to run into old friends and colleagues whom you may have spent a month rotating with! If you read about my time at Danbury Hospital in Connecticut, Drs. O. Olayinka and G. Kuar were part of it and I’m glad to call them friends!Image 9: Presented by the ASCP Resident and Pathologist Councils, this was a great networking session to discuss fellowships, employment, and how to plan for the first 100 days of working in laboratory medicine from PGY-1 and on! I certainly learned a lot!Image 10: (left to right) Dr. K. Chaztopoulos from the Mayo Clinic, myself, and K.C. Booth, RN in front of his finalist poster in the scientific category! Another valuable professional connection and friend made through my experiences in laboratory medicine.Image 11. When one of your mentors (Dr. K. Mirza) is signing copies of The Pathologist magazine that featured him on the cover, you get in line for one …obviously.Image 12. Dr. M. Upton is an inspirational speaker and insightful individual both on stage and in person. She had words of encouragement for my upcoming residency interview season and made sure I felt I could rely on ASCP for whatever I needed professionally. Thank you, Dr. Upton!Image 13. Some more colleagues from Mayo Clinic Pathology (left to right): Dr. A. Ravindran, Dr. D. Larson, Dr. J. Dalland, and myself. These folks were very busy with all the great hematology sessions at the SHEAHP2019 meeting.Image 14: No ASCP Annual Meeting would be complete without the leadership, passion, and vision of our CEO Dr. Blair Holladay. He, his leadership team, and this organization have been integral in my path to pathology and I can’t wait to see what’s in store for the future!
Social media has become so valuable in our field. Not just
for networking, but sharing cases, impressions, publications, and more! It’s so
easy to rally behind a hashtag and support a cause in so many instances—why not
in our profession? Get involved, be an active voice for your own practice as
well as your colleagues.
If you want to learn more about the sessions you may have
missed, download the ASCP2019 app from the Apple App Store or Google App Store!
Thanks for reading! See you on social media, because when we
communicate and collaborate, we are #StrongerTogether! I’m on twitter at
@CKanakis, until next time!
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola
University Chicago with a BS in Molecular Biology and Bioethics and then
Rush University with an MS in Medical Laboratory Science. He is
currently a medical student actively involved in public health and
laboratory medicine, conducting clinicals at Bronx-Care Hospital Center
in New York City.
A 40 year old African American female with a history of sickle cell
disease presented to an outpatient clinic with fever, chills, and leg and back
pain consistent with a sickle cell crisis. Her past medical history was also
significant for asthma and seizures. She rated her pain as 10 out of 10, her vitals
showed a temperature of 101.0°F, and she was also tachycardic and hypotensive.
Her white blood cell count was 23.0 TH/cm2, hemoglobin 8.4 g/dL,
hematocrit 26.0%, and platelets 619,000 TH/cm2. In clinic, she
received pain medications and a fluid bolus, two sets of blood cultures were
collected, and she was transferred to the emergency department for further work
up.
Laboratory Identification
Image 1. Gram stain from a positive blood culture bottle showing small, gram positive budding yeast (1000x oil immersion). Image 2. A mucoid, salmon-colored yeast grew on Sabouraud dextrose and chocolate agars.
Blood culture bottles were positive after approximately two days on the automated instrument. The Gram stain showed small, gram positive budding yeast (Image 1). The BioFire FilmArray for blood culture identification was negative for Candida albicans, C. glabrata, C. krusei, C. parapsilosis, and C. tropicalis. At this time, she was started on micafungin for antifungal therapy. A mucoid, salmon colored yeast grew on both Sabouraud dextrose and chocolate agars (Image 2) and was identified by Vitek 2 as Rhodotorula spp.
Discussion
Rhodotorula spp. are
basidiomycetous yeasts that make up the normal microbiota on moist skin and can
be found in bathtubs and on shower curtains. Rhodotorula spp. are usually considered contaminants, but can
rarely cause fungemia in patients with central lines, endocarditis,
peritonitis, and meningitis, especially in those that are immunocompromised. R. mucilaginosa, R. glutinis, and R. minuta
are the species commonly associated with human disease.
In the laboratory, Rhodotorula
spp. grow as a mucoid, salmon colored yeast within 1-3 days of incubation. On
Gram stain or lactophenol cotton blue prep, the yeast is small and round to
oval with multilateral budding. Pseudohyphae are not usually present. Rhodotorula spp. produce urease and fail
to ferment carbohydrates. R. mucilaginosa
is negative for nitrate assimilation. Identification can also be confirmed by
commercial kits, automated systems, and MALDI-TOF mass spectrometry. Rhodotorula spp. are intrinsically
resistant to echinocandins and fluconazole.
In the case of our patient, she was switched to intravenous
amphotericin B after the identification of Rhodotorula
spp. was made. Reference laboratory testing identified the isolate as R. mucilaginosa with high minimum
inhibitory concentrations (MIC) to fluconazole and echinocandins. Amphotericin
had an MIC of 0.5 µg/ml. She successfully completed a 14 day course with close
monitoring of creatinine, electrolytes, and platelet count. Repeat blood
cultures were negative and no other focuses of infection were found on CT
scans, transthoracic echocardiogram, and ophthalmology exam.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the
University of Mississippi Medical Center in Jackson, MS. She is
certified by the American Board of Pathology in Anatomic and Clinical
Pathology as well as Medical Microbiology. She is the Director of
Clinical Pathology as well as the Microbiology and Serology
Laboratories. Her interests include infectious disease histology,
process and quality improvement, and resident education.