A 65 year
old man with diabetes mellitus type 2 presented to the emergency department
(ED) for left hip pain. He has a remote history of avascular necrosis of
bilateral hips of unknown etiology for which he received a bilateral total hip
arthroplasty and subsequent multiple revisions due to hardware failure several
years ago. He initially presented to an urgent care clinic a few months prior
for “noise with movement” of the left hip and mild lower back pain. Plain radiographs
of the left hip in comparison to his prior imaging were unremarkable and he was
subsequently discharged. Repeat imaging at a follow-up visit at the orthopedic
clinic showed mild superior migration of the femoral head bilaterally secondary
to periprosthetic osteolysis of
the joint headliner. He was scheduled for surgery however presented to the ED prior
to his scheduled appointment with severe crushing left hip pain and restricted
joint mobilization. He denied fevers, chills, night sweats, or any other recent infections. The left
hip was aspirated yielding
10cc of dark
black fluid and a stat gram stain was ordered.
Laboratory identification
The stat gram stain showed many
polymononuclear cells with moderate gram positive bacilli in a background of
dark inorganic material (Image 1). Following 48 hours of incubation, there was anaerobic
growth on the kanamycin and vancomycin (KV) and schaedler agar
plates. A Gram stain of the broth showed gram positive bacilli arranged
singly and in chains with some decolorization (Image 2). The KV and schaedler plates showed moderate growth of a single
organism consisting of small glossy tan colored colonies (Images 3-4). No
aerobic growth was observed on the blood, MacConkey, Columbia Naladixic Acid (CNA),
or chocolate agar plates. Mass
spectrometry (MALDI-TOF) identified the
pathogenic organism as Clostridium innocuum.
Image 1. Synovial fluid Gram stain of the left hip showed moderate gram positive bacilli and many polymononuclear cells in a background dark inorganic debris (100x oil immersion).Image 2. Gram stain from a positive broth culture showed gram positive bacilli arranged singly and in chains with some decolorization (100x oil immersion).Image 3. Anaerobic growth on the schaedler agar showed growth of a single organism consisting of small round glossy tan colored colonies. Image 4. Anaerobic growth on the kanamycin and vancomycin (KV) agar showed growth of a single organism consisting of small glossy tan colored colonies.
Discussion
Bacterial joint infections are more common in prosthetic joints as
compared to native joints with a prevalence of 1-2% following hip arthroplasty
(1). Most cases of bacterial septic
arthritis are due to staphylococci (40 percent),
streptococci (28 percent) or gram negative bacilli (19 percent) organisms (2). Joint
infections secondary to anaerobes are less likely and account for 2-3%
of all cases (3). A review of the literature shows less than 50 documented
cases of septic arthritis due to Clostridium species. Amongst these
cases Clostridium perfringens is the most commonly isolated pathogen (4).
To date there are no documented cases of joint infections secondary to Clostridium
innocuum species.
Clostridium innocuum is a non-motile, anaerobic, gram positive organism
that reproduces by sporulation. These organisms are normally found as a part of
the usual human gut flora and are rarely human pathogens. The name “innocuum”
is derived from the term “innocuous” to convey the innocence of these organisms
as they do not produce clostridial exotoxins. A review of the literature shows
fewer than 20 reported cases of Clostridiuminnocuum infections
with most reported cases being described in immunocompromised patients such as
those with diabetes mellitus, chronic
hepatitis, acquired immune deficiency syndrome (AIDS), leukemia, and
organ transplantation (5-6). Clinically patients can present with a spectrum of
symptoms which include fever
of unknown origin, diarrhea/constipation, and non-specific respiratory symptoms.
In almost all cases bacteremia ensued. Most
cases were associated with a traumatic penetrating injury with few reported
cases due to hematogenous spread (5-6).
Laboratory identification of Clostridiuminnocuum can be challenging due to its variable gram staining morphology and
atypical colony morphology on differing culture media. Most traditional
phenotypic methods can only reliably identify these organisms to the genus
level as a Clostridium species. However, using mass spectrometry
(MALDI-TOF) these organisms can be identified to the species level. Rapid
identification of Clostridium innocuum from the subset of Clostridium
species is clinically important as these organisms are the only known Clostridium
species with intrinsic resistance to vancomycin (7). Although they do not
possess clostridial exotoxins, these organisms are thought to have a
lipopolysaccharide-like virulence factor and have a mortality rate comparable
to toxigenic Clostridium species (7). Due to resistance to vancomycin, metronidazole, piperacillin and ampicillin-sulbactam are the
alternative recommended first-line treatment options.
For this
patient, following the results of the gram smear the patient was started on IV vancomycin
but due to an adverse allergic reaction was switched to intravenous pencillin G
and oral ciprofloxacin. He was subsequently taken to the operating room for
incision and drainage and left hip revision arthroplasty with cup exchange. Blood
cultures were collected post-operatively and showed no growth, possibly due earlier
antibiotic administration. Susceptibility studies from Mayo Laboratories showed
pan susceptibility to penicillin, piperacillin-tazobactam, ertapenem,
clindamycin, and metronidazole. The patient was subsequently switched to
intravenous penicillin and continued to show clinical improvement during his
remaining hospital course.
References
Horowitz DL,
Katzap E, Horowitz S, Barilla-labarca ML. Approach to septic arthritis. Am Fam
Physician. 2011;84(6):653-60.
Ryan MJ,
Kavanagh R, Wall PG, Hazleman BL. Bacterial joint infections in England and
Wales: analysis of bacterial isolates over a four year period. Br J Rheumatol.
1997;36(3):370-3.
Gredlein CM,
Silverman ML, Downey MS. Polymicrobial septic arthritis due to Clostridium
species: case report and review. Clin Infect Dis. 2000;30(3):590-4.
Leal J,
Gregson DB, Ross T, Church DL, Laupland KB. Epidemiology of Clostridium species
bacteremia in Calgary, Canada, 2000-2006. J Infect. 2008;57(3):198-203.
Lee NY,
Huang YT, Hsueh PR, Ko WC. Clostridium difficile bacteremia, Taiwan. Emerging
Infect Dis. 2010;16(8):1204-10.
Chia JH,
Feng Y, Su LH, et al. Clostridium innocuum is a significant
vancomycin-resistant pathogen for extraintestinal clostridial infection. Clin
Microbiol Infect. 2017;23(8):560-566.
-Noman Javed, MD is a 3rd year anatomic and
clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
The following case is an interesting overlap of
Hematopathology and Molecular Diagnostics, and shows the utility of sequencing
to detect a cancer before biopsy could.
A 63 year old gentleman presented to a heme/onc physician
with six months of intractable anasarca, fatigue, and a recent mild
thrombocytopenia (Table 1). They were otherwise in healthy condition. The
physician initiated a lymphoma work-up that included a bone marrow biopsy. The
tests were negative for M-protein.
Table 1. Summary of symptoms and relevant abnormal labs.
The bone marrow biopsy was somewhat limited, but the core contained multiple marrow elements. After a thorough review by a Hematopathologist, no evidence of dysplasia or other irregularities could be detected (Image 1). Flow cytometry detected no aberrant blast population. Cytogenetics detected 20del [16/20] and 5del [3/20]. These findings did not clearly indicate a specific diagnosis.
Image 1. 40x view of the bone marrow specimen at the initial presentation. No evidence of dysplasia was found.
As the clinical suspicion for a malignancy was high, the
bone marrow specimen was sent for sequencing on a 1385-gene panel test. The
test included tumor-normal matched DNA sequencing (“tumor” sample: bone marrow,
normal: saliva), RNA whole transcriptome sequencing on the bone marrow, and
Copy Number Variant (CNV) analysis. Tumor-normal matched sequencing helps rule
out variants that are normal and present in the patient.
Somatic mutations were determined as those that were present
in the “tumor” sample and not in the matched normal sample. The somatic
variants found are listed below with their variant allele frequency (VAF) in
parenthesis. Recall that a VAF of 40% means that a mutation is present in the
heterozygous state in 80% of cells.
IDH2 (p.R140Q, 46%)
SRSF2 (p.P95T, 51%)
CBL (p.R499*, 47%)
KRAS (p.K117N, 12%)
Figure 1. View of IGV, which displays the NGS reads for IDH1 along with the variant allele highlighted in red. The color of the bars indicates the direction of the reads (forward in red and reverse in blue). This reflects the allele frequency of approximately 50%.
The mutations in these genes are commonly found in myeloid
cancers including myselodysplastic syndrome. Activating mutation in IDH2 (isocitrate dehydrogenase 2)
increase the production of the oncometabolite 2-HG, which alters methylation in
cells taking them to an undiffereitiated state. SRSF2 (Serine And Arginine Rich Splicing Factor 2) is a part of the
spliceosome complex, which regulates how sister chromatids separate from each
other. Failures in the proper function of the complex creates genomic
instability. CBL (Casitas B-lineage
Lymphoma) is a negative regulator of multiple signaling pathways, and loss of
function mutations (as seen here) lead to increased growth signals through
several tyrosine kinase receptors. KRAS
(Kirsten RAt Sarcoma virus) is an upstream mediator of the RAS pathway, which
acquires mutations that lead to constitutive activation and sends growth
signals to cells causing them to proliferate.
Furthermore the CNV analysis
also found the heterozygous loss of chromosome 20 as reported in cytogenetics.
CNV analysis did not detect chromosome 5 deletion, as it was below the limit of
detection (20% for CNV analysis).
Figure 2. This plot shows the normalized read frequency of genes across each of the chromosomes is shown here. The drop at chromosome 20 is shown in a pale brown color on the right side of the graph. This is consistent with the cytogenetic findings. The loss of 5q isn’t seen as it is below the limit of detection of 30%.
These mutations are all individually common in MDS, but the co-occurance of each gives very strong evidence that MDS is the diagnosis (Figure 3). There have also been studies that provide prognostic implications for several of the genetic mutations present. Some mutations like SRSF2 or CBL at high VAF (>10%) indicate a poor prognosis, but mutations in IDH2 or TP53 at any frequency have not only a high chance of progression, but also a faster time to onset of disease. Another non-genetic risk factor for developing MDS is an elevated RDW, which we saw in our patient.
Figure 3. From Becker et al 2016.
All of these high-risk factors together led us to push for a diagnosis of MDS based off of molecular findings, and the patient was started on treatment with Azacitadine. Our assessment was confirmed 3 months later when, the patient’s follow up bone marrow biopsy showed significant progression with megakaryocytic and erythroid dysplasia and hyperplasia and reticulin fibrosis MF2 (Image 2). Aberrant blasts were detected (1-2%), but not elevated. This demonstrates how molecular findings predicted and predated the patient’s rapid progression to morphologic disease.
Image 2. Dysplastic, hyperplastic megakaryocytes and erythroid lineage.
In summary, multiple molecular mutations indicative of MDS
were found in a symptomatic patient’s unremarkable bone marrow biopsy months
before a rapid progression to MDS.
References
Steensma DP, Bejar R, Jaiswal S et al. Blood 2015;126(1):9-16.
Sellar RS, Jaiswal S, and Ebert BL. Predicting progression to AML. Nature Medicine 2018; 24:904-6.
Abelson S, Collord G et al. Prediction of acute myeloid leukemia risk in healthy individuals. Nature 2018; 559:400-404.
Desai P, Mencia-Trinchant N, Savenkov O et al. Nature Medicine 2018; 24:1015-23.
Becker PM. Clonal Hematopoiesis: The Seeds of Leukemia or Innocuous Bystander? Blood.2016 13(1)
-Jeff SoRelle, MD is a Chief Resident of Pathology at the
University of Texas Southwestern Medical Center in Dallas, TX. His
clinical research interests include understanding how the lab intersects
with transgender healthcare and improving genetic variant
interpretation.
The majority of laboratory injuries and exposures are
preventable, and most of them occur because staff is not paying close attention
to the situation. They lose their situational awareness or were never paying
attention to it from the start. Unfortunately, lab safety professionals spend
much of their time investigating such incidents rather than being able to
prevent them. If laboratory staff could understand the power of the pause, labs
would have fewer dangerous incidents.
One illustration of that power can be seen in a simple
exercise. A group of people is asked to read aloud quickly a list of words that
indicate different colors- green, red, etc. The words themselves, however, are
written in different colors, and the colors do not match the words. For
example, the word “red” is written in black, the word “blue” is written in
green, etc. This first part goes well, you’re just asking them to read the
actual words. Next, however, it gets harder. The people are asked to quickly go
down the list again, but this time they are asked to say the color of the word,
not that actual word. Typically, this does not go well. For the next step, the
exercise is repeated at a much slower pace, with a slight pause between each
word. Once a pause is placed between each word, the people recite the correct
colors. The incongruent words and colors creates what is known as the “Stroop
Effect,” first theorized in 1935, but pausing is a means of overcoming this
issue in our brains.
When investigating a needle stick incident, the lab safety
officer learned the employee completed the draw, attempted to engage the needle
safety device, but stuck their finger when grabbing the needle to toss it into
the sharps container. She did not notice the safety device did not engage and
the needle was still exposed. The employee stated she was busy and in a hurry
because there were many other patients waiting. I have always said that when a
lab employee is stressed and busy, that’s when stopping for a moment to gain
situational awareness is most important. Had this employee paused for a moment
to ensure the needle safety device was fully engaged, the incident would never
have occurred.
The lab manager had to speak to a chemistry tech after a
serum splash exposure to the eyes. When looking at the work area, the manager
noticed there was an adjustable face shield in place but that staff moved it
into place only when needed. The tech admitted he was busy at the time of the
splash and that he neglected to move the shield into place before uncapping
specimens. Again, a pause to think about safety here would have helped.
In another situation, a microbiology technologist was eager
to start the day and get it done since her vacation began the next day. She
quickly went through the daily checklist and checked items off but did not
actually perform the checks. Halfway through the day, she noticed it seemed
warm and that it was unusually quiet at her biological safety cabinet work
station. She decided to look at the gauges and noticed that there was no
protective air flow in operation. She had been working with TB samples all
morning. When she reported the issue, the manager told her that all employees
in the area would need to go to Employee Health and be followed up for TB
exposures. Pausing to perform the safety checks at the beginning of the shift
would have made a big difference in that outcome for several employees.
Pausing for safety in the laboratory setting can be a
powerful tool, even during the busiest moments. In fact, that’s when it works
best. Use that pause in your arsenal, and teach maintaining situational
awareness with your staff so that future injuries and exposures can be
prevented.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years
experience as a certified medical technologist. Today he is the
Laboratory Safety Officer for Sentara Healthcare, a system of seven
hospitals and over 20 laboratories and draw sites in the Tidewater area
of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
A man in his 40’s with a past medical history of acute
lymphoblastic leukemia/lymphoma (in remission), multiple infections including
bacteremia and pulmonary aspergillosis, presented to the hospital with fever
and diarrhea. Over the course of his stay, he had worsening renal function and
developed profound hypotension and shock, which prompted initiation of two
vasopressors and high-dose steroids. Eventually he developed acute hypoxic
respiratory failure, requiring intubation. Complete blood count demonstrated an
absolute eosinophilia of 8.58 x109/L (reference range 0.04-0.62 x109/L).
Imaging revealed bilateral pulmonary infiltrates and a pleural effusion.
Respiratory culture with gram stain was ordered for his tracheal aspirate,
which revealed few polymorphonuclear cells, many gram-negative rods, yeast, and
larvae of Strongyloides stercoralis (Image
1A). Wet mounts of the tracheal aspirate revealed numerous larvae and a few
eggs of S. stercoralis (Image 1B-C);
many of the larvae were motile (Movie 1). Stool examination of ova and
parasites (O & P) were positive for larvae. Given the burden of organisms
and prior administration of steroids, he was diagnosed with severe
strongyloidiasis, consistent with hyperinfection. Concurrent blood cultures
grew Enterococcus faecalis and Stenotrophomonas maltophilia; the
respiratory culture also grew S.
maltophilia, and tracks from the migrating larvae were observed on
respiratory culture bacterial media (Image 1D).
Image 1. Tracheal aspirate Gram stain with S. stercoralis larvae, 100x objective magnification (A). Wet mount of tracheal aspirate revealing larvae (B) and eggs (C), 40x objective magnification. Blood agar plate growing S. maltophilia in an abnormal pattern, indicating motile larvae tracking through the agar (D).
Discussion
Strongyloidiasis is a spectrum of clinical disease caused by
the nematode Strongyloides stercoralis.1,2
Descriptions of acute infection have been described in other Lablogatory
entries here,3,4 and the full lifecycle is described in detail on
the CDC DPDx website.5
Severe strongyloidiasis includes the syndromes of
hyperinfection and disseminated disease. Hyperinfection
is when there is an elevated burden of the typical autoinfection cycle
involving the lungs and GI-tract. Usually there is an antecedent
immunosuppressive event, such as administration of corticosteroids. Within the
GI-tract lumen, increased numbers of rhabditiform larvae transform into the
infective filariform larvae, which traverse the GI mucosa, migrate to the lungs
via bloodstream/lymphatics where they enter alveolar air spaces, then ascend
the respiratory tract, and are coughed up by the host and swallowed to re-enter
the GI tract. In the GI tract adult females lay eggs through parthenogenesis,
which give rise to further rhabditiform larvae. In extreme cases of
hyperinfection, adults can be found in the lungs, where they may also lay eggs.
Finding eggs in respiratory specimens is unusual, and may be related to the
burden of disease.6
Disseminated disease
is when larvae can be found in any additional organs/organ systems, such as the
central nervous system, kidneys, liver, adrenals, etc. Invasive sampling is not
typically performed, and larvae can be observed at autopsy.
Laboratory diagnosis of S.
stercoralis involves identification of rhabditiform larvae in stool O
&P exam; the presence of adults or eggs in stool is rare. Rhabditiform
larvae have short buccal cavities and an ovoid genital primordium structure midway through the body (Movie 2).
O&P exams can be performed on other body fluids, such as sputum and CSF.
Serology can be useful to identify past exposure, especially prior to
initiating immunosuppressive therapeutics such as corticosteroids. A
nonspecific finding can be observed, as in this case, in the complete blood
cell count and differential. Relative and absolute eosinophilia can be found in
patients with parasitic infections; therefore, it is reasonable to rule out
parasitic infection in this subset of patients. In the case presented here, the
absolute eosinophilia was likely due to a persistent S. stercoralis infection, since these nematodes can live in the
human host for decades.
The treatment of choice for severe strongyloidiasis is oral
ivermectin, though albendazole is an alternative therapy. In some instances,
subcutaneous ivermectin administration may be used.7
Follow-up
Oral ivermectin was administered to treat the
strongyloidiasis and antibiotics were administered to treat the bacterial
infections. Over the coming days, serial tracheal aspirates continued to reveal
many larvae and eggs, so therapy was escalated to subcutaneous ivermectin. Over
the course of therapy, the patient developed a fungemia with Candida guilliermondii. Despite
aggressive antimicrobial therapy and intensive care, the patient remained
hypoxemic and hypotensive. The family decided to transition to comfort measures
and the patient passed away.
References
Maguire JH. Intestinal Nematodes (Roundworms), in Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, B. Mandell, Dolin, Editor. 2010, Elsevier: Philadelphia, PA. p. 3577-3586.
Parasitology, in Koneman’s Color Atlas and Textbook of Diagnostic Microbiology, Procop et al., Editors. 2017, Lippincott Williams & Wilkins: China. p. 1452-1454.
Keiser PB and Nutman TB. Strongyloides stercoralis in the Immunocompromised Population. Clin Microbiol Rev, 2004. 17(1): p. 208-17.
Hurlimann E and Keiser J, A single dose of ivermectin is sufficient for strongyloidiasis. Lancet Infect Dis, 2019. 19(11): p. 1150-1151.
-IJ Frame, MD, PhD, Microbiology Fellow, University of Texas Southwestern Dallas, Texas
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
“Never, ever underestimate the importance of having fun,”
said Randy Pausch, a professor of computer science at Carnegie Mellon
University. Indeed, having fun is an important component of life, and that
includes your professional life. However, having fun in the workplace can seem
like an impossible task sometimes. There is, after all, lots of work to be
accomplished, performance to be measured, and projects to complete. This can
make it challenging to find of time and ways to have fun appropriately and
constructively.
The benefits of having fun in the workplace are plentiful. Because
most fun activities require people to work in groups or teams, the shared
experience can increase collaboration, engagement, and foster communication. Having
fun fosters motivation and commitment to an organization as people associate
the positive feelings and experiences with the workplace. This also increases
morale and comradery among the participants, which increases their performance.
All these aspects, in turn, foster creativity, innovative thinking, and
problem-solving skills. The more creative employees are, the more comradery
they feel among themselves, and the better they perform the more turnover is
reduced. Having fun in the workplace is incredibly beneficial to both the
employees and the organization overall.
In today’s workplace culture, people are generally more
aware and considerate of what is appropriate behavior. This also applies to
having fun, because if activities are only fun and enjoyable if they are
appropriate for everyone involved. It is, therefore, important to establish
clear boundaries: what is considered part of this activity and what is not. It
is also important to consider different levels of physical, mental, and
emotional ability. Having fun is inclusive and collaborative, so it is critical
to design activities that everyone can partake in. The activity should also
always be optional. Making participation mandatory is not actually fun for people,
so make sure that there is an opt-in and opt-out option. Finally, every
activity should have some element of learning and education. If you are asking
people to participate in a fun activity, ensure that they are learning
something about one another or about a specific topic.
There are many different ways in which you can incorporate
fun in the workplace. Last year at ASCP, our social committee hosted an ‘Oscar
Party” in which we could vote for our colleagues in categories such as “Outside
the Box Thinker/Innovator,”, “Outstanding Philanthropist,” and “Rookie of the
Year.” Then all staff gathered in the kitchen area of our office that was
decorated with a red carpet and we all received a glass of sparkling cider. The
winners were announced and cheered on as they walked the red carpet. They gave
a short speech after receiving their little Oscar award. It was a simple way to
have some collective fun and it felt so great cheering everyone on and
recognizing certain employees for their outstanding contribution to the society.
On average, babies laugh about 400 times a day. Adults, on the other hand, only laugh about 35 times a day and significantly less often on weekdays than on weekend (Beard, 2014). Laughter is incredibly important to our overall well-being and performance. In fact, “laughter relieves stress and boredom, boosts engagement and well-being, and spurs not only creativity and collaboration but also analytic precision and productivity”(Heggie, 2018). So, let’s try to incorporate more fun and more laughter in both our personal and our professional lives. Let’s find ways to cheer each other up and create a collaborative, warm, and productive environment that fosters engagement, retention, and analytic precision. After all, laughter is the best medicine.
-Lotte Mulder, EdM, is the Senior Manager of Organizational Leadership and Patient Engagement at ASCP. She earned her Masters of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. After she graduated, Lotte started her own consulting company focused on establishing leadership practices in organizations, creating effective organizational structures, and interpersonal coaching. She has worked in Africa, Latin America, Asia, and the U.S. on increasing leadership skills in young adults through cultural immersion, service learning and refugee issues, and cross-cultural interpretation. She is currently working toward a PhD in Organizational Leadership.
During the 2019 ASCP Annual Meeting in Phoenix, I noticed a
morning workshop session entitled “The Impact of Fun.” The title intrigued me,
so decided to take a break from the science and clinical medicine workshops
that I would normally attend, and take advantage of the opportunity to listen
in.
I have been working as a pathologist and lab director for 30
years, and while I hate to admit it, I had never thought seriously about taking
time during the day for playing games with my co-workers. I was always consumed
with meetings, deadlines, and getting the clinical work completed.
At the beginning of the course, I was a little unsure what I
had gotten myself into. However by the time the workshop concluded, the reality
of what I had been missing had set in.
When I returned to work following the meeting, I began to
search for fun activities that our lab team could do over a lunch hour. I set a
date and promised food to entice the wary into attending the event in the
conference room. Once they had assembled, I divided the group into two teams by
drawing an imaginary line down the middle of the room. We then played team trivia
using a book of questions I had acquired. By the end of the hour, everyone was
laughing and having fun. The lab continued to buzz with talk and occasional
laughter all afternoon.
We have continued setting aside one noon hour each month
where we gather for different types of games. Charades, and Pictionary have
been hits. Mostly everyone brings their own lunch, but food or deserts are
provided on occasion to keep these events special. There are a few who choose
not to participate, but even they occasionally show up to watch and laugh along
with the rest. As is pointed out above, you cannot make having fun a mandatory
or it ceases to be fun.
Our lab staff really seem to enjoy these events and so does
this old pathologist. During our most recent event, one of my young colleagues
remarked how much fun these lunches have been, and that they hoped we would
continue these going forward. I intend to keep these going as long as I
continue working. It has provided me with an opportunity to get to know each of
my co-workers much better. I only wish I had learned about the importance of
having fun with your co-workers and teammates earlier in my career. I encourage
other pathologists, lab directors and section supervisors to learn from my
experience and begin finding ways to bring the fun back into the workplace if
you have not already done so.
-Dr. Wisecarver is currently Professor Emeritus in the Department of Pathology/Microbiology at the University of Nebraska Medical Center in Omaha, Nebraska. He served as Medical Director of the Clinical Laboratories for Nebraska Medicine, their clinical affiliate from 1996 until 2017. He currently serves as the Director of the Histocompatibility Laboratory for Nebraska Medicine.
A 77 year old male presented to the hospital with chest
pain, lightheadedness, burning urination for the past few weeks. He has blood
in his urine due to a previously diagnosed neoplasm. The patient moved from
India to the United States in February, with a diagnosis of bladder cancer and
a history of hypertension, congestive heart failure, coronary artery disease,
and atrial fibrillation. In the hospital, abscesses on both right and left
kidneys were found, and patient had nephrostomy tubes placed. Purulent
discharge confirmed he had a severe urinary tract infection.
Laboratory Identification
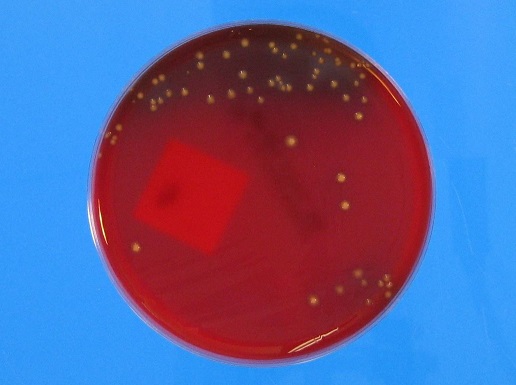
The patient’s urine culture grew >100,000 colony forming
units/milliliter (CFU/ml) of an oxidase-positive, non-lactose fermenting
Gram-negative rod. On the blood agar plate, large gray, smooth, flat, mucoid, β-hemolytic
colonies were found. Although bacteria growing on solid media should not be
actively smelled, the organism emitted a grape or tortilla smell from the
plate. The organism was identified as Pseudomonas
aeruginosa by MALDI-TOF mass spectrometry. The isolate was plated onto Mueller
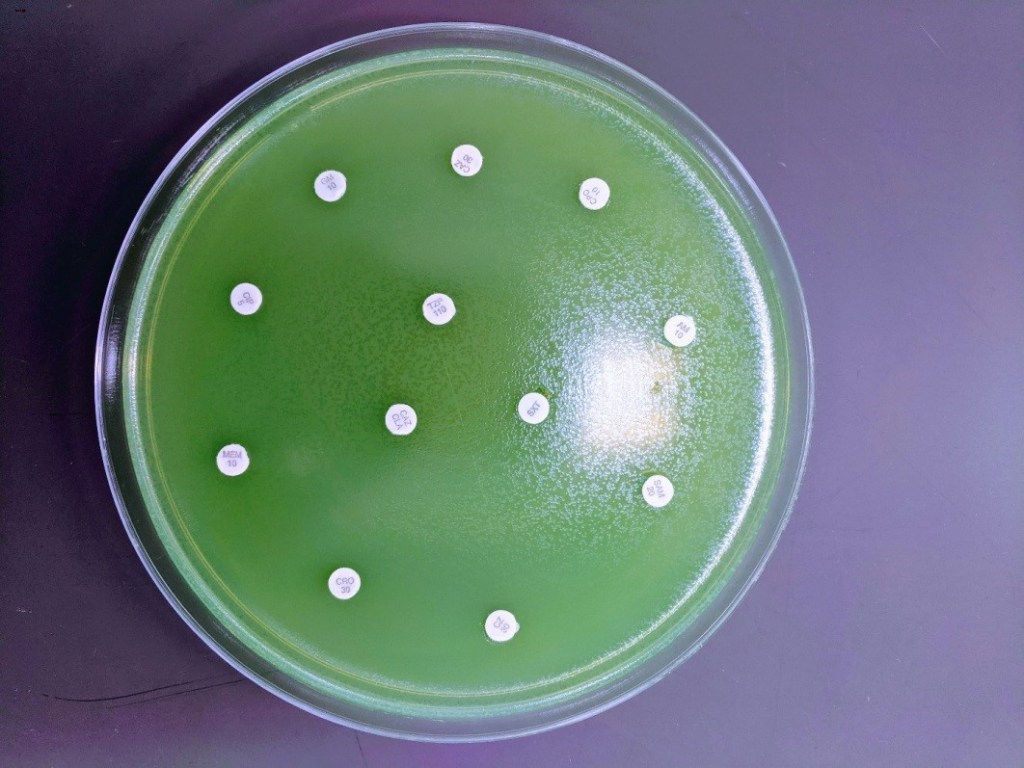
Hinton agar for Kirby-Bauer disc diffusion antibiotic susceptibility testing (Image 1). A fluorescent green lawn of bacteria
grew up to the edge of all discs, indicating high-level resistance to all
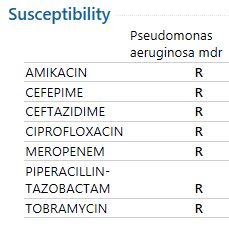
antibiotics tested (Table 1). Modified
carbapenem inactivation method (mCIM) testing was positive and Cepheid
GeneXpert CarbaR PCR testing revealed that this P. aeruginosa isolate carried the New Delhi metallo-β-lactamase-1
carbapenemase (NDM-1).
Image 1. Kirby-Bauer disc diffusion was used for antimicrobial susceptibility testing. Note no zones around any of the antibiotic discs, indicating resistance to all antimicrobials tested.
Table 1. Antimicrobial susceptibility testing interpretations. All drugs tested were resistant to this P. aeruginosa isolate.
Discussion
The issue of super bugs is on the rise, with the fear of
antibiotic resistance disseminating through more bacterial populations and
species. Carbapenems are drugs that are very powerful broad-spectrum
antibiotics, usually reserved as a last resort treatment for serious and
resistant infections.1 β-lactamases are divided into four Ambler
classes: A, B, C, and D. Class B differs from the others because it utilizes
zinc as a metal cofactor for its catalytic activity. The others use a serine
residue for their catalytic activity.2
NDM-1 is a class B β-lactamase. It was named after New Delhi, India when a Swedish resident presented with an extremely resistant infection after a trip to India in 2008. NDM-1 bacteria can now be found with high prevalence in India and China, and increasingly in other countries such as the UK and US.3,4 While the origination of the gene may not have been India, many of these infections are from people who have traveled to India or other Asian continents.5 Concerns about overprescribing and misuse of antibiotics in India are rising, where India is one of the biggest consumers of antibiotics in the world. One study even found striking evidence of this misuse, demonstrating that 2 out of 3 adults under 20 presented antibiotic resistance isolates to fluoroquinolones and/or cephalosporins.6,7,8
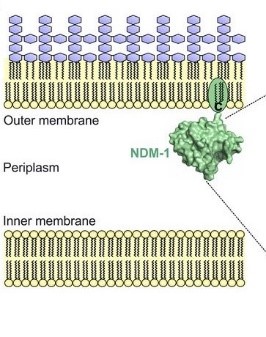
Image depicting the NDM-1 protein anchored in the outer membrane of the bacterium. (Taken from Bahr, Guillermo, et al. “Clinical Evolution of New Delhi Metallo-β-Lactamase (NDM) Optimizes Resistance under Zn(II) Deprivation.” Antimicrobial Agents and Chemotherapy, vol. 62, no. 1, 2017, doi:10.1128/aac.01849-17.)
The gene for NDM-1 is blaNDM-1 and has been found on both plasmid and chromosomal components of different bacteria. Due to its presence on plasmids, the gene can easily spread through bacterial populations and other bacterial species – as has already been documented in Enterobacteriaceae and A. baumannii.3 The β-lactamase that it codes for is a lipoprotein that is anchored in the outer membrane of the gram negative bacteria. Other metalo-β-lactamases (MBLs) are periplasmic proteins, which are more affected by changes in essential metal cofactors in their enzymatic function. Thus far, it has been found that there are 16 discovered variants of NDM. Some variants being more fit than NDM-1. It is hypothesized that these variants are being selected for in the clinical setting, with the protein being more stable and demonstrating higher affinities for zinc during time of metal-chelating (a process the immune system adapts to combat infections).9 Unfortunately, NDM-1 and its variants are resistant to almost all antibiotics. Usually the only option is colistin and tigecycline.3
The disturbing issue, and the big picture, is the capability
of MDR organisms and their genes of disseminating. As previously mentioned, NDM-1
is capable of spreading to other species and within its population. Yet, a
terrifying report has demonstrated blaNDM-1
detection in artic soil samples from 2013, 4 years after the first detection of
the gene.10 This demonstrates the ability for antibiotic resistance
to spread on a global scale, and how serious this battle truly is.
Walther-Rasmussen, Jan, and Niels Høiby.
“Class A Carbapenemases.” Journal of Antimicrobial Chemotherapy, vol. 60, no.
3, 2007, pp. 470–482., doi:10.1093/jac/dkm226.
Khan, Asad U., et al. “Structure, Genetics and
Worldwide Spread of New Delhi Metallo-β-Lactamase (NDM): a Threat to Public
Health.” BMC Microbiology, vol. 17, no. 1, 2017, doi:10.1186/s12866-017-1012-8.
Mohapatra P. R. (2013). Metallo-β-lactamase 1–why blame New
Delhi & India?. The Indian journal of medical research, 137(1),
213–215.
Gupta, M., Didwal, G., Bansal, S., Kaushal,
K., Batra, N., Gautam, V., & Ray, P. (2019). Antibiotic-resistant
Enterobacteriaceae in healthy gut flora: A report from north Indian semiurban
community. The Indian journal of medical research, 149(2), 276–280.
doi:10.4103/ijmr.IJMR_207_18
Kotwani, Anita, and Kathleen Holloway. “Access
to Antibiotics in New Delhi, India: Implications for Antibiotic Policy.”
Journal of Pharmaceutical Policy and Practice, vol. 6, no. 1, 2013,
doi:10.1186/2052-3211-6-6.
Kotwani, Anita, et al. “Antibiotic-Prescribing
Practices of Primary Care Prescribers for Acute Diarrhea in New Delhi, India.”
Value in Health, vol. 15, no. 1, 2012, doi:10.1016/j.jval.2011.11.008.
Bahr, Guillermo, et al. “Clinical Evolution of
New Delhi Metallo-β-Lactamase (NDM) Optimizes Resistance under Zn(II)
Deprivation.” Antimicrobial Agents and Chemotherapy, vol. 62, no. 1, 2017,
doi:10.1128/aac.01849-17.
Mccann, Clare M., et al. “Understanding Drivers
of Antibiotic Resistance Genes in High Arctic Soil Ecosystems.” Environment
International, vol. 125, 2019, pp. 497–504., doi:10.1016/j.envint.2019.01.034.
-Ben Dahlstrom is a recent graduate of the NorthShore University HealthSystem MLS program. He currently works as a molecular technologist for Northwestern University in their transplant lab, performing HLA typing on bone marrow and solid organ transplants. He graduated with a bachelors in Biology at the University of Illinois at Chicago (UIC) and concurrently from the UIC Honors College. He discovered his passion for the lab through his experience in healthcare. His interests include microbiology, molecular, immunology, and blood bank.
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.
A 66 year old man with past medical history of recently diagnosed Clostridioides difficile colitis presented to emergency department with diarrhea, weight loss of 52 pounds in 4 months, and occasional night sweats. CT imaging revealed dilation of small bowel with thickened mucosal folds. The duodenum was subsequently biopsied to reveal diffuse intestinal lymphangiectasia containing PAS positive and Congo red negative eosinophilic material and lamina propria foamy macrophages. Laboratory investigations revealed normocytic anemia, proteinuria, and peripheral IgM kappa monoclonal gammopathy.
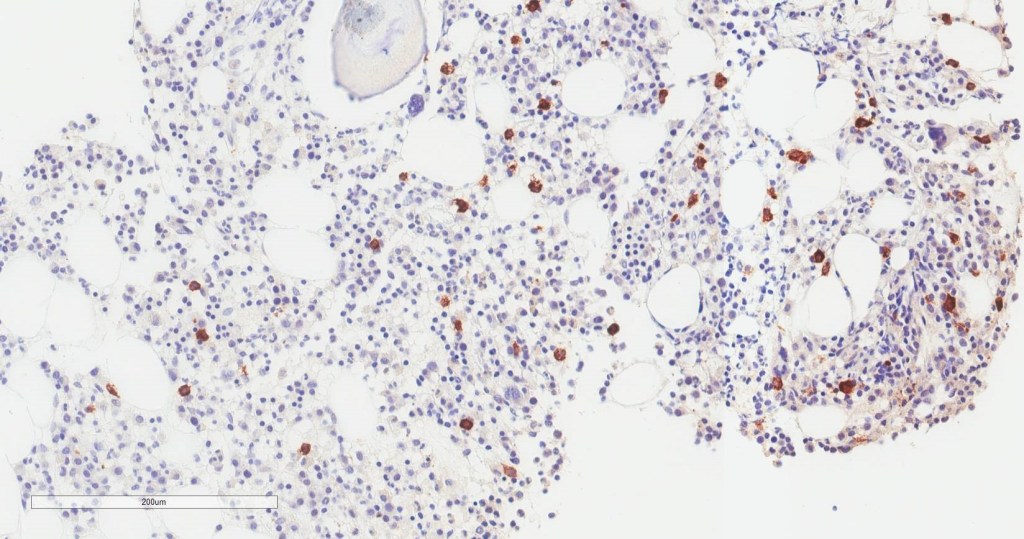
Bone
marrow aspirate shows increased plasma cells and mast cells. H&E stained
sections demonstrate a normocellular bone marrow with trilineage hematopoiesis
and involvement by 35% plasma cells. By immunohistochemistry, CD138 highlights clusters
of plasma cells that predominantly express kappa light chain restriction.
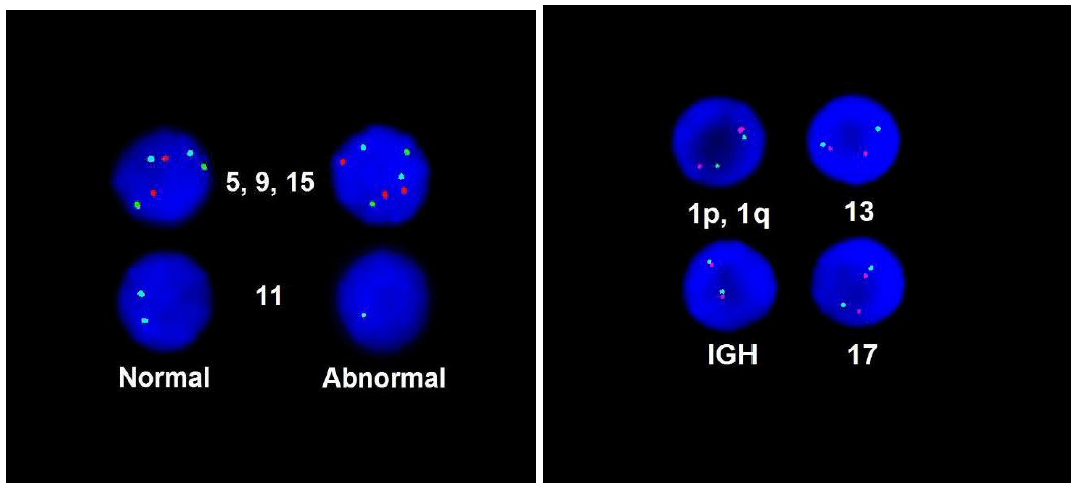
FISH
and Mutation Analysis
FISH
demonstrated loss of chromosome 11 and gain of chromosome 15, which was
consistent with plasma cell dyscrasia. MYD88 mutation analysis did not
detect the mutation.
Diagnosis
The
findings of the patient’s normocytic anemia, IgM monoclonal gammopathy, and
intestinal lymphangectasia with an associated plasma cell dyscrasia involving
the bone marrow favor a lymphoplasmacytic lymphoma/Waldenström
macroglobulinemia.
Discussion
Waldenstrom
macroglobulinemia (WM) is a malignant B-cell lymphoproliferative disorder characterized by lymphoplasmacytic infiltration of the bone
marrow and peripheral IgM monoclonal gammopathy.1 It is rare with an
overall incidence of 3 per million persons per year, accounting for 1-2% of
hematologic cancers.1 It
occurs predominantly in Caucasian males, with a median age of 63-68 years old
at diagnosis.1-3
Patient
may be asymptomatic for years and require observation or experience a broad
spectrum of signs and symptoms. These symptoms may be attributable to the tumor
infiltration of the bone marrow and lymphoid tissues, IgM circulating in the
blood, and IgM depositing into tissues. The most common clinical presentation
of WM is fatigue and nonspecific constitutional symptoms, such as fever, night
sweats, and weight loss, due to normochromic, normocytic anemia. 20-30% of
patients may exhibit lymphadenopathy and hepatosplenomegaly due to infiltration
of peripheral tissues. High concentration of IgM in the circulation may lead to
hyperviscosity, resulting in oronasal bleeding, gingival bleeding, blurred
vision due to retinal hemorrhages, and neurological symptoms, including
headache, ataxia, light-headedness, dizziness, and rarely, stroke.2-3 The gastrointestinal manifestations are rare; however, IgM monoclonal
protein may deposit into the lamina propria of the GI tract, causing diarrhea,
steatorrhea, and GI bleeding.4 Other
IgM-related manifestations include cold agglutinin hemolytic anemia,
cryoglobulin, and amyloid deposition in tissues.3
Diagnosis
of WM includes evidence of IgM monoclonal gammopathy
and at least 10% of bone marrow infiltration by lymphoplasmacytic cells.5 Monoclonal
gammopathy can be detected by the monoclonal spike, or M-spike, on serum
protein electrophoresis.3 Serum immunofixation may be performed to identify
the type of monoclonal protein and the type of light chain involved.3
In terms of immunophenotype, neoplastic cells express surface IgM, cytoplasmic Igs, CD38, CD79a, and
pan B-cell markers (CD19, CD20, and CD22). CD10 and CD23 are absent. Expression
of CD5 occurs in approximately 5-20% of cases.6 Recent
studies have reported two most common somatic mutations in WM, which are MYD88
L265P mutations (90-95% of cases) and CXCR4 (30–40% of cases).7 Absence
of these mutations, however, do not completely exclude the diagnosis of WM.
The International Staging System for WM
identifies five factors associated with adverse prognosis, including age older
than 65, hemoglobin < 11.5g/dL, platelet count < 100K/μL,
beta-2-microglobulin > 3mg/L, and monoclonal IgM concentration > 7g/L.3 Patients
younger than the age of 65 years with 0 or 1 of these factors are in the
low-risk category with a median survival of 12 years.3 In contrast, patients
with 2 or more risk factors are in the intermediate- and high-risk categories and
have a median survival of almost 4 years. 3
Management of WM depends on the patient’s
clinical manifestations.Furthermore, patients with minimal symptoms
should be managed with rituximab, whereas patients with severe symptoms related
to WM should receive more aggressive treatment, including dexamethasone,
rituximab and cyclophosphamide. Hyperviscosity syndrome is an oncologic
emergency that requires removal of excess IgM from the circulation via
plasmapheresis.8
References
Neparidze N, Dhodapkar MV. Waldenstrom’s Macroglobulinemia: Recent advances in biology and therapy. Clin Adv Hematol Onco. 2009 Oct;7(10): 677-690.
Leleu X, Roccaro AM, Moreau AS, Dupire S, Robu D, et al. Waldenstrom Macroglobulinemia. Cancer Lett. 2008 Oct;270(1):095-107.
Tran T. Waldenstrom’s macroglobulinemia: a review of laboratory findings and clinical aspects. Laboratory Medicine. 2013 May;44(2):e19-e21.
Kantamaneni V, Gurram K, Khehra R, Koneru G, Kulkarni A. Distal illeal ulcers as gastrointestinal manifestation of Waldenstrom Macroglbulinemia. 2019 Apr; 6(4):pe00058.
Grunenberg A, Buske C. Monoclonal IgM gammopathy and Waldenstrom’s macroglobulinemia. Dtsch Arztebl Int. 2017 Nov;114(44):745-751.
Bhawna S, Butola KS, Kumar Y. A diagnostic dilemma: Waldenstrom’s macroglobulinemia/plasma cell leukemia. Case Rep Pathol. 2012;2012:271407.
Varettoni M, Zibellini S, Defrancesco I, Ferretti VV, Rizzo E, et all. Pattern of somatic mutations in patients with Waldenstrom macroglobulinemia or IgM monoclonal gammopathy of undetermined significance.
Oza A, Rajkumar SV. Waldenstrom macroglobulinemia: prognosis and management. Blood Cancer Journal. 2015;5:e394.
-Jasmine Saleh, MD MPH is a pathology resident at Loyola University Medical Center with an interest in dermatopathology and hematopathology. Follow Dr. Saleh on Twitter @JasmineSaleh.
–Kamran M. Mirza, MD, PhD, MLS(ASCP)CM is an
Assistant Professor of Pathology and Laboratory Medicine, Medical
Education and Applied Health Sciences at Loyola University Chicago
Stritch School of Medicine and Parkinson School for Health Sciences and
Public Health. A past top 5 honoree in ASCP’s Forty Under 40, Dr. Mirza
was named to The Pathologist’s Power List of 2018 and placed #5 in the
#PathPower List 2019. Follow him on twitter @kmirza.
The patient is a 50 year old male who
presented to urgent care with 5 days of fevers, chills, and myalgias. He reports
no known tick bites, or prior treatment for tickborne illness, he travels
frequently for work and has been in Pittsburgh, Omaha, Philadelphia, Charlotte,
and Long Island over the past 3 months and is frequently outside golfing in
Vermont and while traveling. At urgent care he had a CBC, CMP and urinalysis.
His CBC was remarkable for leukopenia with absolute neutropenia (WBC count
2,790; Absolute neutrophil count 390) and thrombocytopenia (platelet count 26,000/cmm).
His CMP was remarkable for a mildly elevated AST (66U/L) and total bilirubin
(2.4mg/dL). A peripheral blood smear was made which revealed ring forms in his
red blood cells. BINAX testing for malaria was negative. The next day he
presented to the emergency department with left upper quadrant abdominal pain,
night sweats, fatigue, fever, and blood in his urine where is was informed of
his CBC results and was immediately started on azithromycin and atovaquone. Given
the severity of his presentation a co-infection with Anaplasma phagocytophilum (Anaplasmosis) was suspected though the PCR
testing was negative.
Laboratory
Identification
Image 1. Giemsa stain of thin blood smears showing intracellular (left) and extracellular (right) ring-form organisms.
Thick and thin blood smears (recommended) were prepared
which showed both intra and extracellular organisms with in normal sized red
blood cells. BINAX testing for malaria was negative. Given the appearance and
presence both within and outside the cell a diagnosis of Babesiosis was made.
Discussion
Babesiosis in the United States is caused by the microscopic
parasite Babesia microti. Occasional cases caused by other species of Babesia
have been detected (1). Babesia microti is spread by Ixodes
scapularis ticks (also called blacklegged ticks or deer ticks) (1,2). Transmission
mainly occurs in parts of the Northeast and upper Midwest; and it usually peaks
during the warm months (1). Because Babesia
shares a vector and geographic distribution with Borrelia burgdorferi (Lyme disease) coinfection of ticks with these
two organisms can be seen in up to 40% of ticks and though the incidence of
Babesiosis is much lower; up to 10% of Connecticut patients with seropositivity
for Lyme disease are also seropositive for Babesia
(2).
Most infections are probably asymptomatic. Manifestations of
disease include fever, chills, sweating, myalgias, fatigue, hepatosplenomegaly,
and hemolytic anemia. Symptoms typically occur after an incubation period of 1
to 4 weeks, and can last several weeks. The disease is more severe in patients
who are immunosuppressed, splenectomized, and/or elderly (1,3).
During a blood meal, a Babesia-infected tick
introduces sporozoites into the human host (1,3). Sporozoites enter
erythrocytes and undergo asexual replication (budding). Multiplication of the
blood stage parasites is responsible for the clinical manifestations of the
disease (1). Humans are dead-end hosts and there is probably little, if any,
subsequent transmission that occurs from ticks feeding on infected persons (1).
However, human to human transmission is well recognized to occur through blood
transfusions (1). Diagnosis is often rendered by direct visualization on thick
and thin blood smears. Because the percent parasitemia is often low, the
organisms can be easily missed, especially by automated hematology analyzers
(3). Molecular methods such as PCR can be performed (3), but are not
recommended as the first line test as the blood parasite exam with thick and
thin blood smears are clinically sensitive in patients with symptomatic disease.
Most mild cases of Babesiosis will resolve spontaneously
without treatment, especially in patient with a spleen (1,3). Treatment for
more severe disease includes either azithromycin and atovaquone or clindamycin
and quinine (1,3). If patients are severely immunocompromised and/or
splenectomized can be treated with exchange transfusion in addition to
antimicrobials (3).
-Casey Rankins, DO, is
a 3rd year Anatomic and Clinical Pathology resident at the
University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
I belong to a Hematology Interest Group and always enjoy
seeing the case studies and questions that other techs post. This group is multinational
so I see posts from techs all over the world. It’s interesting to see the
similarities and differences in standard operating practices and the roles
techs play in different areas and different countries. It’s also interesting to
see that we all come across the same types of problems and difficult specimens!
In the last few months in this
Hematology Interest Group, I have seen many questions and comments about
resolving clumped platelets, and am therefore using this opportunity to shed
some light on these tricky specimens. The case I am presenting, and the photos,
are courtesy of Abu Jad Caesar, who is a Lab manager at Medicare Laboratories – Tulkarm branch, in
Palestine.
The patient had a CBC performed
on a Nihon Kohden 6410. WBC was 12.7 x 103μL, impedance platelet count was 20,000/μL on initial run, other parameters appeared within normal
limits. The sample was warmed and a Na Citrate tube was requested to rule out pseudothrombocytopenia.
After warming, the EDTA was rerun with a platelet count of 0/μL. The Na Citrate tube was run, and platelet count from the
instrument was 189,000/μL. (Figure 1)
Because of the blood:anticoagulant ratio in the Na Citrate tube, a multiplier
of 1.1 was applied, thus making the Na Citrate platelet count 207,900/μL. Slides were made, stained and examined. Image 1 shows
the clumping in the EDTA tube. Image 2 shows the smear from the Na Citrate
tube, with no visual clumping.
The CBC was reported with the following comments:
Platelet clumping observed, 2 samples drawn to rule out thrombocytopenia. EDTA
whole blood smear had many platelet clumps noted (EDTA induced
thrombocytopenia). Conclusion: Platelets are adequate and estimated to be about
200,000/μL.
Figure 1. Results from warmed EDTA tube (left) and Na Citrate tube (right). Image 1. Clumped platelets seen with EDTA. Image 2. Normal platelet count with no clumping seen with Na Citrate.
Platelet counts in the normal range don’t usually give us too
much trouble in reporting, even if some clumping is present, mainly because
they are normal. Adequate platelet counts fall within a typical reference range
of about 150- 450 x 103/μL.
If there are instrument flags for a platelet abnormal scattergram or platelet
clumps, it is recommended to repeat testing by another method. If the initial
count is performed by impedance counting, many analyzers can also report
optical or fluorescent platelet counts. With impedance counting, very small
RBCs or fragments may be counted as platelets, thus giving a falsely increased
platelet count. With optical counting, large platelets can be counted as RBCs,
thus giving a falsely decreased count. Some Sysmex hematology analyzers use
impedance and optical counts and also feature fluorescent platelet counts which
use a platelet specific dye and give accurate platelet counts without the
interferences of other methods. A normal platelet count, even with clumping
seen on a smear, is still usually estimated to be normal (or may occasionally be
increased.)
Thrombocytopenia, on the other hand, can be a challenge in
the hematology laboratory. With thrombocytopenia, physicians need an accurate
count to diagnose, treat or monitor patients. Even a small increase or decrease
can be significant when there is a severe thrombocytopenia. With fewer
platelets, every platelet counts!
One of the first questions we must ask with an apparent
thrombocytopenia is if this is a true thrombocytopenia or if it is pseudothrombocytopenia
(PTCP). A true thrombocytopenia represents a patient with a low platelet count
who may need monitoring or medical intervention. It can be dangerous to miss
true thrombocytopenia but is also dangerous to report a low platelet count in a
patient with a spurious thrombocytopenia who is not actually thrombocytopenic. Pseudothrombocytopenia,
or spurious thrombocytopenia, is defined as an artificially or erroneously low
platelet count. In PTCP, the low platelet count is due to clumps that are
counted as 1 platelet. (These large clumps can also be counted as WBCs, thus
giving a falsely increased WBC count.)
We can divide PTCP into 2 categories Platelet
clumping is most commonly caused by pre-analytic errors such as over-filled or
under-filled EDTA tubes, clotted specimens, or a time delay between sample
collection and testing. Techs should check the tube for clots and sample volume
and do a delta check to help differentiate thrombocytopenia and PTCP. But, with
an apparent ‘good’ sample, the next step would be a smear review. If there are
clumps seen on the smear, then we need to decide what caused the clumps. Is it the
first category, one of these common pre-analytical issues, or is it the 2nd
category of PTCP, an in vitro agglutination of platelets? Conditions that can
cause this in vitro agglutination of platelets include cold agglutinins,
multiple myeloma, infections, anticardiolipin antibodies, high immunoglobulin
levels, abciximab therapy and EDTA induced pseudothrombocytopenia. (EDTA-PTCP) Of
these, EDTA induced pseudothrombocytopenia is the most common cause. (Nakashima,
2016).
When techs talk about platelet clump issues, it is usually
because we are looking for ways to resolve or to accurately estimate the
platelet count in these samples, and there doesn’t seem to be one easy answer.
The clumping makes precise counting impossible and even estimates can be very
tricky. How can we estimate these counts? Do we simply report the presence of
clumping with “appear normal”, “decreased” or “increased”? Or, should we break
our estimates into more ranges to give physicians more valuable information?
And, what if the provider wants an actual count in order to give the patient
the best care possible and we can’t resolve the clumping? What can we do to
provide a count? Some of the first steps recommended include vortexing the
sample for 2 minutes to break up platelet clumps, then re-analyzing. Warming
samples may also help to resolve platelet clumps, particularly in samples with
cold agglutinins or that have had a delay in testing and have been transported
or stored at room temperature or below. If clumps persist and recollecting the
sample still yields platelet clumping, then pre-analytical error can be ruled
out an EDTA induced pseudothrombocytopenia may be suspected. Many labs will
have an alternate tube drawn or use another method to help resolve the
clumping.
So, what is EDTA induced thrombocytopenia
(EDTA-PTCP)? This is not representative of a particular
clinical picture, and is not diagnostic for any disorder or drug therapy, but
is a laboratory phenomenon due to presence of EDTA dependent IgM/IgG autoantibodies.
These antibodies bind to platelet membrane glycoproteins in presence of EDTA. EDTA
induces and enhances this binding by exposing these glycoproteins to the antibodies.
(Geok Chin Tan, 2016) Though it is an
in vitro phenomenon, patients with certain conditions, such as malignant
neoplasms, chronic liver disease, infection, pregnancy, and autoimmune
diseases, do have increased risk of EDTA-PTCP. However, EDTA-PTCP has also been
observed in patients who are disease free. (Zhang, 2018)
What are some alternate methods to help resolve EDTA induced
platelet clumping challenges? Probably the most common is to redraw the sample
in a Na Citrate tube. Both EDTA and Na Citrate tubes should be drawn. In a true
EDTA-PTCP, as seen in our case study, you should see clumps on the smear made
from the EDTA tube and no clumps on the smear made from the Na Citrate tube. Because
of the volume of the anticoagulant in the Na Citrate tube you must also apply
the dilution factor of 1.1 to the count from the Na Citrate tube to get an
accurate platelet count. Note, however, that hematology analyzers are FDA
approved and validated for use with EDTA tubes. If you wish to use a different
anticoagulant, the method must be validated in your laboratory. Note also that
alternate methods will generally only resolve EDTA -PTCP, and not clumping due
to other cold agglutinins, medication or disorders. In addition, anticoagulant
induced thrombocytopenia is not limited to EDTA. It can also occur with citrate
and heparin. In a study, it was found that up to 17% of patients with an EDTA -PTCP
also exhibited this phenomenon with citrate. In fact, researchers have found,
and we have found in our own validations, that some samples that do not clump
in EDTA actually DO clump in Na Citrate. Thus, alternate tubes may not resolve
all platelet clumping. (Geok Chin Tan, 2016)
Some labs have validated ACD (Citric acid, trisodium citrate,
dextrose) anticoagulant tubes for EDTA-PTCP. Using this method, the EDTA tube
and ACD must be run in parallel and a conversion factor applied, reflecting the
difference in sample dilution in the 2 tubes. A parameter such as the RBC must
be chosen to make this comparison. Using a formula that divides the RBC in EDTA
by the RBC in ACD gives a ratio that reflects the dilutional differences
between anticoagulants. This ratio can then be multiplied by the ACD platelet
count to obtain the ACD corrected platelet count. (CAP Today, 2014). Some
sources have recommended ACD tubes because the incidence of clumping with Na
Citrate can be frustratingly high. It is theorized that the more acidic ACD
tube may prevent platelet clumping better than Na Citrate. (Manthorpe, 1981)
Less commonly used tubes are CTAD (trisodium citrate,
theophylline, adenosine, dipyridamole) and heparin. CTAD acts directly on
platelets and inhibits platelet factor 4 thus minimizing platelet activation. Downsides
to CTAD tubes are that they are light sensitive and must be stored in the dark,
and can be costly. They also alter the blood/additive dilution ratio so
calculations must be used, as seen with Na Citrate and ACD. Heparin tubes are
less commonly found to be beneficial in resolving platelet clumping issues
because heparin can active platelets. Heparin tubes are also more expensive, so
have not generally been a first choice for EDTA-PTCP.
I have heard from techs that their labs have very good
results using amikacin added to EDTA tubes to prevent spuriously low platelet
counts in patients with EDTA-PTCP. Amikacin should be added to the EDTA tube
within 1 hour after draw and testing is stable for up to 4 hours at room
temperature. Results of a study done in 2011 showed that the addition of
amikacin to the EDTA tube produced rapid dissociation of the platelet clumps
with little or no effect on morphology or indicies. This method has proved very
promising for reporting accurate platelet counts in patients with
multianticoagulant induced PTCP. (Zhou, 2011)
The last anticoagulant tube that I have seen mentioned by
many techs in the hematology interest group are Sarstedt ThromboExact tubes. I
have seen many posts from techs who use these and they seem to have a very good
success rate. ThromboExact tubes contain magnesium salts and are specifically designed
to determine platelet counts in cases of PTCP. They are currently validated
only for platelet counts and samples are stable for 12 hours after collection.
Interestingly, before automated hematology analyzers, magnesium was the
anticoagulant of choice for manual platelet counts. EDTA-PTCP has been
recognized since EDTA automated platelet counts were introduce in the 1970s. A
2013 study in Germany used ThromboExact tubes with excellent results for
resolving multianticoagulant induced PTCP. These tubes became commercially
available during the study, in 2013. (Schuff-Werner, 2013) Unfortunately for us
in the United States, these tubes are not available in the US. I was recently
at a conference and went up to the Sarstedt representatives and asked about
these tubes. I was told that they are available in parts of Europe and Asia but
are not FDA approved in the US. I asked very hopefully if they were looking at
getting FDA approval and was unfortunately told that “they didn’t think they
had the market for them to pursue approval.”
Whichever alternative method your lab chooses to use, it is
recommended to draw an EDTA and the alternate tube together. This way the 2
counts and the presence or absence of clumping in the tubes can be compared. We
have many patients who had one incidence of clumping, yet when the provider orders
a Na Citrate platelet count, we get a new draw of both EDTA and Na Citrate tubes
together, and there is no flagging or clumping seen with EDTA. In these cases
it is appropriate to result the EDTA results as there is no evidence of
EDTA-PTCP.
When a patient has a low PLT count without any
hematologic disease, family history, and/or bleeding-tendency identified, and
pre-analytical errors have been ruled out, PTCP should be considered. This
does not mean that a patient with PTCP will have a normal platelet count after
the clumping is resolved. As stated above, many patients with EDTA-PTCP have
hematological or other disorders and may be truly thrombocytopenic. Resolving
the clumping in these patients allows us to give the provider an accurate
platelet count, which is very important in thrombocytopenic patients.
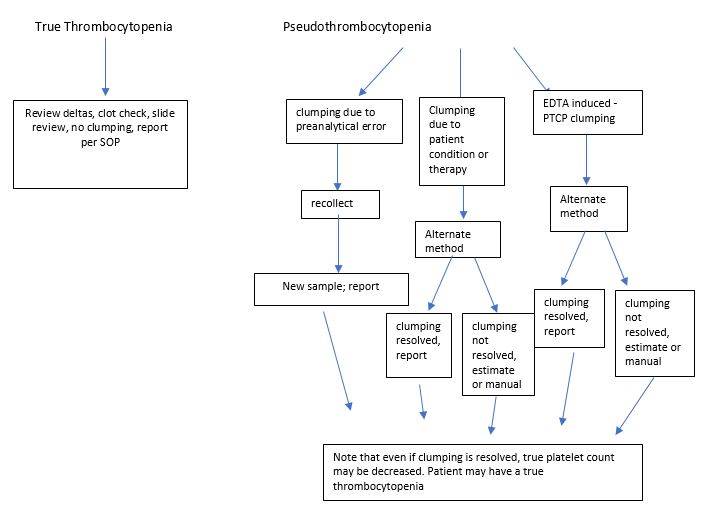
The flow chart below (Figure 4) shows some things to
consider when dealing with platelet clumping. It is our goal to resolve
clumping so that we can report an accurate platelet count in a timely fashion. In
the laboratory where I work, I have validated Na citrate tubes, but these seem
to resolve clumping in less than 50% of patients. As a last resort, to get an
accurate platelet count, some articles have suggested collecting a fingerstick
and performing manual counts. I did include this in the chart as an option for
multianticoagulant PTCP, however, due to the difficulty in collecting a good
specimen and the subjectivity of counts, along with problems associated with
necessary calculations, our pathologists have decided that we will not do
manual platelet counts. For this reason, I am currently involved in platelet
clumping monitoring and will be conducting a small internal study to compare
ACD, CTAD and Na Citrate tubes in parallel. Depending on those results we may
also then test amikacin. If we come to any enlightened conclusions I’ll write
another short blog with our results!
Thanks again to Abu Jad Caesar, lab manager at Medicare Laboratories – Tulkarm branch, in Palestine, who provided me with this textbook perfect
case of PCTP, which was easily resolved by collecting in Na Citrate. We wish
they all read the textbooks and were as cooperative!
Figure 2. Flowchart for resolving and reporting of thrombocytopenia.
Manthorpe
R, Kofod B, et al. Pseudothrombocytopenia, In vitro studies on the underlying
mechanisms. Scand J Haematol 1981; 26:385-92
Nakashima
MO, Kottke-Marchant K. Platelet Testing: In: Kottke-Marhchant K, ed. An
Algorithmic Approach to Hemostasis Testing, 2nd ed. CAP Press;
2016:101
Schuff-Werner,Peter, et al.
Effective estimation of correct platelet counts in pseudothrombocytopenia using
an alternative anticoagulant based on magnesium salt. Brit J of Haematol Vol
162, Issue 5. June 29, 2013
Tan,
Geok Chin et al. Pseudothrombocytopenia due to platelet clumping: A Case Report
and Brief Review of the Literature. Case Reports in Hematology. Volume 2016
Lixia Zhang, MMed,* Jian Xu, MD,* Li
Gao, MMed, Shiyang Pan, MD, PhD. Spurious Thrombocytopenia in Automated
Platelet Count. Laboratory Medicine 49:2:130-133. 2018
Zhou,Xiamian,
et al. Amikacin can be added to blood to reduce the fall in platelet count. Am
Journal of Clinical pathology, Vol 136, Issue 4, Oct 2011.
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated
from Merrimack College in N. Andover, Massachusetts with a BS in
Medical Technology and completed her MS in Clinical Laboratory Sciences
at the University of Massachusetts, Lowell. She has worked as a Medical
Technologist for over 30 years. She’s worked in all areas of the
clinical laboratory, but has a special interest in Hematology and Blood
Banking. When she’s not busy being a mad scientist, she can be found
outside riding her bicycle.