I belong to a Hematology Interest Group and always enjoy seeing the case studies and questions that other techs post. This group is multinational so I see posts from techs all over the world. It’s interesting to see the similarities and differences in standard operating practices and the roles techs play in different areas and different countries. It’s also interesting to see that we all come across the same types of problems and difficult specimens! In the last few months in this Hematology Interest Group, I have seen many questions and comments about resolving clumped platelets, and am therefore using this opportunity to shed some light on these tricky specimens. The case I am presenting, and the photos, are courtesy of Abu Jad Caesar, who is a Lab manager at Medicare Laboratories – Tulkarm branch, in Palestine.
The patient had a CBC performed on a Nihon Kohden 6410. WBC was 12.7 x 103μL, impedance platelet count was 20,000/μL on initial run, other parameters appeared within normal limits. The sample was warmed and a Na Citrate tube was requested to rule out pseudothrombocytopenia. After warming, the EDTA was rerun with a platelet count of 0/μL. The Na Citrate tube was run, and platelet count from the instrument was 189,000/μL. (Figure 1) Because of the blood:anticoagulant ratio in the Na Citrate tube, a multiplier of 1.1 was applied, thus making the Na Citrate platelet count 207,900/μL. Slides were made, stained and examined. Image 1 shows the clumping in the EDTA tube. Image 2 shows the smear from the Na Citrate tube, with no visual clumping.
The CBC was reported with the following comments: Platelet clumping observed, 2 samples drawn to rule out thrombocytopenia. EDTA whole blood smear had many platelet clumps noted (EDTA induced thrombocytopenia). Conclusion: Platelets are adequate and estimated to be about 200,000/μL.



Platelet counts in the normal range don’t usually give us too much trouble in reporting, even if some clumping is present, mainly because they are normal. Adequate platelet counts fall within a typical reference range of about 150- 450 x 103/μL. If there are instrument flags for a platelet abnormal scattergram or platelet clumps, it is recommended to repeat testing by another method. If the initial count is performed by impedance counting, many analyzers can also report optical or fluorescent platelet counts. With impedance counting, very small RBCs or fragments may be counted as platelets, thus giving a falsely increased platelet count. With optical counting, large platelets can be counted as RBCs, thus giving a falsely decreased count. Some Sysmex hematology analyzers use impedance and optical counts and also feature fluorescent platelet counts which use a platelet specific dye and give accurate platelet counts without the interferences of other methods. A normal platelet count, even with clumping seen on a smear, is still usually estimated to be normal (or may occasionally be increased.)
Thrombocytopenia, on the other hand, can be a challenge in the hematology laboratory. With thrombocytopenia, physicians need an accurate count to diagnose, treat or monitor patients. Even a small increase or decrease can be significant when there is a severe thrombocytopenia. With fewer platelets, every platelet counts!
One of the first questions we must ask with an apparent thrombocytopenia is if this is a true thrombocytopenia or if it is pseudothrombocytopenia (PTCP). A true thrombocytopenia represents a patient with a low platelet count who may need monitoring or medical intervention. It can be dangerous to miss true thrombocytopenia but is also dangerous to report a low platelet count in a patient with a spurious thrombocytopenia who is not actually thrombocytopenic. Pseudothrombocytopenia, or spurious thrombocytopenia, is defined as an artificially or erroneously low platelet count. In PTCP, the low platelet count is due to clumps that are counted as 1 platelet. (These large clumps can also be counted as WBCs, thus giving a falsely increased WBC count.)
We can divide PTCP into 2 categories Platelet clumping is most commonly caused by pre-analytic errors such as over-filled or under-filled EDTA tubes, clotted specimens, or a time delay between sample collection and testing. Techs should check the tube for clots and sample volume and do a delta check to help differentiate thrombocytopenia and PTCP. But, with an apparent ‘good’ sample, the next step would be a smear review. If there are clumps seen on the smear, then we need to decide what caused the clumps. Is it the first category, one of these common pre-analytical issues, or is it the 2nd category of PTCP, an in vitro agglutination of platelets? Conditions that can cause this in vitro agglutination of platelets include cold agglutinins, multiple myeloma, infections, anticardiolipin antibodies, high immunoglobulin levels, abciximab therapy and EDTA induced pseudothrombocytopenia. (EDTA-PTCP) Of these, EDTA induced pseudothrombocytopenia is the most common cause. (Nakashima, 2016).
When techs talk about platelet clump issues, it is usually because we are looking for ways to resolve or to accurately estimate the platelet count in these samples, and there doesn’t seem to be one easy answer. The clumping makes precise counting impossible and even estimates can be very tricky. How can we estimate these counts? Do we simply report the presence of clumping with “appear normal”, “decreased” or “increased”? Or, should we break our estimates into more ranges to give physicians more valuable information? And, what if the provider wants an actual count in order to give the patient the best care possible and we can’t resolve the clumping? What can we do to provide a count? Some of the first steps recommended include vortexing the sample for 2 minutes to break up platelet clumps, then re-analyzing. Warming samples may also help to resolve platelet clumps, particularly in samples with cold agglutinins or that have had a delay in testing and have been transported or stored at room temperature or below. If clumps persist and recollecting the sample still yields platelet clumping, then pre-analytical error can be ruled out an EDTA induced pseudothrombocytopenia may be suspected. Many labs will have an alternate tube drawn or use another method to help resolve the clumping.
So, what is EDTA induced thrombocytopenia (EDTA-PTCP)? This is not representative of a particular clinical picture, and is not diagnostic for any disorder or drug therapy, but is a laboratory phenomenon due to presence of EDTA dependent IgM/IgG autoantibodies. These antibodies bind to platelet membrane glycoproteins in presence of EDTA. EDTA induces and enhances this binding by exposing these glycoproteins to the antibodies. (Geok Chin Tan, 2016) Though it is an in vitro phenomenon, patients with certain conditions, such as malignant neoplasms, chronic liver disease, infection, pregnancy, and autoimmune diseases, do have increased risk of EDTA-PTCP. However, EDTA-PTCP has also been observed in patients who are disease free. (Zhang, 2018)
What are some alternate methods to help resolve EDTA induced platelet clumping challenges? Probably the most common is to redraw the sample in a Na Citrate tube. Both EDTA and Na Citrate tubes should be drawn. In a true EDTA-PTCP, as seen in our case study, you should see clumps on the smear made from the EDTA tube and no clumps on the smear made from the Na Citrate tube. Because of the volume of the anticoagulant in the Na Citrate tube you must also apply the dilution factor of 1.1 to the count from the Na Citrate tube to get an accurate platelet count. Note, however, that hematology analyzers are FDA approved and validated for use with EDTA tubes. If you wish to use a different anticoagulant, the method must be validated in your laboratory. Note also that alternate methods will generally only resolve EDTA -PTCP, and not clumping due to other cold agglutinins, medication or disorders. In addition, anticoagulant induced thrombocytopenia is not limited to EDTA. It can also occur with citrate and heparin. In a study, it was found that up to 17% of patients with an EDTA -PTCP also exhibited this phenomenon with citrate. In fact, researchers have found, and we have found in our own validations, that some samples that do not clump in EDTA actually DO clump in Na Citrate. Thus, alternate tubes may not resolve all platelet clumping. (Geok Chin Tan, 2016)
Some labs have validated ACD (Citric acid, trisodium citrate, dextrose) anticoagulant tubes for EDTA-PTCP. Using this method, the EDTA tube and ACD must be run in parallel and a conversion factor applied, reflecting the difference in sample dilution in the 2 tubes. A parameter such as the RBC must be chosen to make this comparison. Using a formula that divides the RBC in EDTA by the RBC in ACD gives a ratio that reflects the dilutional differences between anticoagulants. This ratio can then be multiplied by the ACD platelet count to obtain the ACD corrected platelet count. (CAP Today, 2014). Some sources have recommended ACD tubes because the incidence of clumping with Na Citrate can be frustratingly high. It is theorized that the more acidic ACD tube may prevent platelet clumping better than Na Citrate. (Manthorpe, 1981)
Less commonly used tubes are CTAD (trisodium citrate, theophylline, adenosine, dipyridamole) and heparin. CTAD acts directly on platelets and inhibits platelet factor 4 thus minimizing platelet activation. Downsides to CTAD tubes are that they are light sensitive and must be stored in the dark, and can be costly. They also alter the blood/additive dilution ratio so calculations must be used, as seen with Na Citrate and ACD. Heparin tubes are less commonly found to be beneficial in resolving platelet clumping issues because heparin can active platelets. Heparin tubes are also more expensive, so have not generally been a first choice for EDTA-PTCP.
I have heard from techs that their labs have very good results using amikacin added to EDTA tubes to prevent spuriously low platelet counts in patients with EDTA-PTCP. Amikacin should be added to the EDTA tube within 1 hour after draw and testing is stable for up to 4 hours at room temperature. Results of a study done in 2011 showed that the addition of amikacin to the EDTA tube produced rapid dissociation of the platelet clumps with little or no effect on morphology or indicies. This method has proved very promising for reporting accurate platelet counts in patients with multianticoagulant induced PTCP. (Zhou, 2011)
The last anticoagulant tube that I have seen mentioned by many techs in the hematology interest group are Sarstedt ThromboExact tubes. I have seen many posts from techs who use these and they seem to have a very good success rate. ThromboExact tubes contain magnesium salts and are specifically designed to determine platelet counts in cases of PTCP. They are currently validated only for platelet counts and samples are stable for 12 hours after collection. Interestingly, before automated hematology analyzers, magnesium was the anticoagulant of choice for manual platelet counts. EDTA-PTCP has been recognized since EDTA automated platelet counts were introduce in the 1970s. A 2013 study in Germany used ThromboExact tubes with excellent results for resolving multianticoagulant induced PTCP. These tubes became commercially available during the study, in 2013. (Schuff-Werner, 2013) Unfortunately for us in the United States, these tubes are not available in the US. I was recently at a conference and went up to the Sarstedt representatives and asked about these tubes. I was told that they are available in parts of Europe and Asia but are not FDA approved in the US. I asked very hopefully if they were looking at getting FDA approval and was unfortunately told that “they didn’t think they had the market for them to pursue approval.”
Whichever alternative method your lab chooses to use, it is recommended to draw an EDTA and the alternate tube together. This way the 2 counts and the presence or absence of clumping in the tubes can be compared. We have many patients who had one incidence of clumping, yet when the provider orders a Na Citrate platelet count, we get a new draw of both EDTA and Na Citrate tubes together, and there is no flagging or clumping seen with EDTA. In these cases it is appropriate to result the EDTA results as there is no evidence of EDTA-PTCP.
When a patient has a low PLT count without any hematologic disease, family history, and/or bleeding-tendency identified, and pre-analytical errors have been ruled out, PTCP should be considered. This does not mean that a patient with PTCP will have a normal platelet count after the clumping is resolved. As stated above, many patients with EDTA-PTCP have hematological or other disorders and may be truly thrombocytopenic. Resolving the clumping in these patients allows us to give the provider an accurate platelet count, which is very important in thrombocytopenic patients.
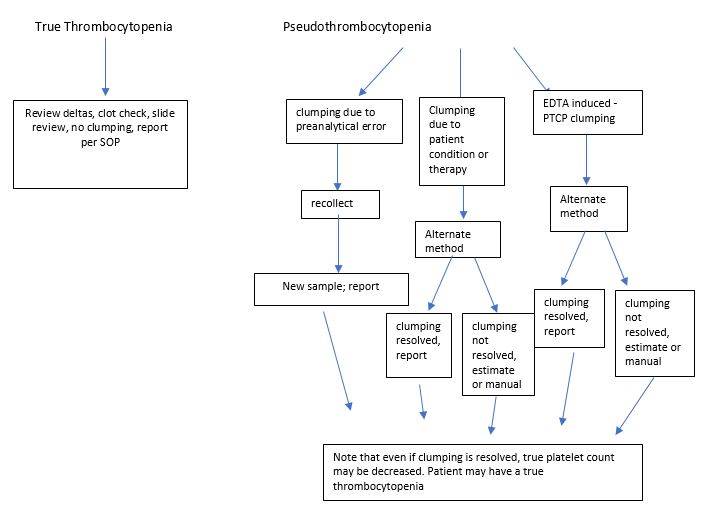
The flow chart below (Figure 4) shows some things to consider when dealing with platelet clumping. It is our goal to resolve clumping so that we can report an accurate platelet count in a timely fashion. In the laboratory where I work, I have validated Na citrate tubes, but these seem to resolve clumping in less than 50% of patients. As a last resort, to get an accurate platelet count, some articles have suggested collecting a fingerstick and performing manual counts. I did include this in the chart as an option for multianticoagulant PTCP, however, due to the difficulty in collecting a good specimen and the subjectivity of counts, along with problems associated with necessary calculations, our pathologists have decided that we will not do manual platelet counts. For this reason, I am currently involved in platelet clumping monitoring and will be conducting a small internal study to compare ACD, CTAD and Na Citrate tubes in parallel. Depending on those results we may also then test amikacin. If we come to any enlightened conclusions I’ll write another short blog with our results!
Thanks again to Abu Jad Caesar, lab manager at Medicare Laboratories – Tulkarm branch, in Palestine, who provided me with this textbook perfect case of PCTP, which was easily resolved by collecting in Na Citrate. We wish they all read the textbooks and were as cooperative!
References
- CAP Today, January 2014. accessed online http://www.captodayonline/qa-column-0114
- Manthorpe R, Kofod B, et al. Pseudothrombocytopenia, In vitro studies on the underlying mechanisms. Scand J Haematol 1981; 26:385-92
- Nakashima MO, Kottke-Marchant K. Platelet Testing: In: Kottke-Marhchant K, ed. An Algorithmic Approach to Hemostasis Testing, 2nd ed. CAP Press; 2016:101
- Schuff-Werner,Peter, et al. Effective estimation of correct platelet counts in pseudothrombocytopenia using an alternative anticoagulant based on magnesium salt. Brit J of Haematol Vol 162, Issue 5. June 29, 2013
- Tan, Geok Chin et al. Pseudothrombocytopenia due to platelet clumping: A Case Report and Brief Review of the Literature. Case Reports in Hematology. Volume 2016
- Lixia Zhang, MMed,* Jian Xu, MD,* Li Gao, MMed, Shiyang Pan, MD, PhD. Spurious Thrombocytopenia in Automated Platelet Count. Laboratory Medicine 49:2:130-133. 2018
- Zhou,Xiamian, et al. Amikacin can be added to blood to reduce the fall in platelet count. Am Journal of Clinical pathology, Vol 136, Issue 4, Oct 2011.

-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
